
As booster shots become available in the United States, many Americans are scrambling to get them. But are these shots the best use of our resources? Who really benefits from them and what is the most prudent way to use our vaccine supplies?
As booster shots become available in the United States, many Americans are scrambling to get them. But are these shots the best use of our resources? Who really benefits from them and what is the most prudent way to use our vaccine supplies?

A first COVID shot will give kids some protection, but none of them will be fully vaccinated until the beginning of December.
For many, many months now, 7-year-old Alain Bell has been keeping a very ambitious list of the things he wants to do after he gets his COVID-19 shots: travel (to Disneyworld or Australia, ideally); play more competitive basketball; go to “any restaurants that have french fries, which are my favorite food,” he told me over the phone.
These are very good kid goals, and they are, at last, in sight. On Tuesday evening, about as early as anyone in the general public could, Alain nabbed his first dose of Pfizer’s newly cleared pediatric COVID-19 vaccine. The needle delivered “a little poke,” he said, but also a huge injection of excitement and relief. Since his father, a critical-care physician, was vaccinated last December (the first time I interviewed Alain), “I’ve been impatient,” Alain said. “I really wanted to get mine.” Now he is finally on his way to joining the adults. When he heard on Tuesday that his shot was imminent, he let out a scream of joy, at “a pitch I have never heard him use before,” his mother, Kristen, told me.
There’s an air of cheer among the grown-ups as well. “It’s cause for celebration,” says Angie Kell, who lives in Utah with her spouse and their soon-to-be-vaccinated 6-year-old son, Beck. Their family, like many others, has been reining in their behavior for months to accommodate their still-vulnerable kid, unable to enjoy the full docket of post-inoculation liberties that so many have. Once Beck is vaccinated, though, they can leave mixed-immunity limbo: “We might have an opportunity to live our lives,” Kell told me.
The past year has been trying for young children, a massive test of patience—not always a kid’s strongest skill. And there’s yet another immediate hurdle to clear: the plodding accumulation of immunological defense. Alain has another 15 days to go until his second dose; after that, it’ll be two more weeks before he reaches a truly excellent level of protection. Only then, on December 7, will he count as fully vaccinated by CDC standards and be able to start adopting the behavioral changes the agency has green-lit. In the intervening weeks, he and the many other 5-to-11-year-olds in his position will remain in a holding pattern. Their wait isn’t over yet.
The timing of this semi-immune stretch might feel particularly frustrating, especially with the winter holidays approaching: At this point, essentially no young kids are slated to be fully vaccinated by Thanksgiving or Hanukkah, except the ones who were enrolled in clinical trials. One shot can offer a level of protection, but experts advise waiting to change behavior for a reason—the extra safeguards that set in about two weeks after the second shot really are that much better, and absolutely worth sitting tight for.
“It takes time for immune cells to get into a position where they’re ready to pounce,” Gigi Gronvall, a senior scholar at the Johns Hopkins Center for Health Security, told me. COVID-19 vaccines teach immune cells to thwart the coronavirus, a process that, like most good boot camps, takes many days to unfold. The second shot is essential to clinch the lesson in the body’s memory, encouraging cells to take the threat more seriously for longer. Immune cells also improve upon themselves over time—the more, the better in these early stages. Gronvall’s own 11-year-old son is also about to get his first shot, and she doesn’t want to risk stumbling so close to the finish line. “I can’t know exactly what his immune system is going to do” after the first dose alone, she said.
Evidence from Pfizer’s original clinical trial, conducted only in adults, hinted that a first, decent defensive bump takes hold after the first shot. Kit Longley, Pfizer’s senior manager of science media relations, pointed to those data when I asked how kids at various points along the vaccination timeline should be approaching behavioral change. “Protection in the vaccinated cohort begins to separate from the placebo arm as early as 12 to 14 days after the first dose,” he told me.
The adult clinical-trial data were collected last year, though, long before the rise of the Delta variant. A more recent study, conducted in the United Kingdom, showed that one dose of Pfizer reduced the risk of symptomatic COVID-19 by only 35.6 percent when the cause was Delta, and by only 47.5 percent with Alpha. (And remember that those numbers apply best on a population scale—not for a single, individual child.) After adding a second dose, though, effectiveness rocketed up to about 90 or 95 percent against either variant. “You really need two doses for adequate, good protection,” Samuel Dominguez, a pediatric-infectious-disease specialist at Children’s Hospital Colorado, told me.
Immunity is so far looking strong in young kids: In a recent trial of thousands of children ages 5 to 11, Pfizer’s vaccine was more than 90 percent effective at blocking symptomatic cases of COVID-19, including ones caused by Delta. Longley said Pfizer expects that the timing of protection will be similar between children and adults—a first dose should lower everyone’s risk to some degree. But the company’s pediatric trial picked up only a few COVID-19 cases; none of them occurred until about three weeks after the first dose was given, or later. So it’s hard to say anything definitive about when “enough” immunity really kicks in for kids.
Some parents are counting on a level of early protection from one shot, including my cousin Joanne Sy, whose 8-year-old son, Jonah, received his first injection on Friday. “He will have good immunity after one dose,” she told me, hopefully enough to guard him on a trip they’re taking to New York for Thanksgiving two weeks from now. “We’re still going to be cautious,” Sy told me: They’ll be watching the Macy’s Thanksgiving Day Parade from a hotel room rather than the streets, and wearing masks, at least on the plane. “But we just need to move forward.”
The calculus is playing out differently for Christy Robinson of Arlington, Virginia, who will again be “hunkering down” with her husband and two daughters, June and Iris, 7 and 5, respectively, this Thanksgiving. The kids got their first Pfizer shot on Saturday, setting their household up for full, full vaccination by mid-December, just in time to hold an indoor gathering with their aunts, uncles, and cousins for Christmas. (Some quick arithmetic: To be fully vaccinated by December 25, a kid would need their first dose by November 20.) June’s also eager to “see my friends inside, because it’s cold outside,” she told me—plus go to movie theaters, and Build-A-Bear, and a trampoline park, and IHOP, and the nail salon.
By the end of this conversation, Robinson looked amused and maybe a little regretful that my question had prompted such an extravagant list. As their mother, she’s especially excited for the possibility of no longer having to quarantine her daughters after viral exposures at school. Heftier decisions are ahead too. She and her husband are still weighing whether to bring their daughters into closer, more frequent indoor contact with their grandparents, who are vaccinated but could still get seriously sick if someone ferries the virus into their midst.
And that risk—of transmitting the virus—is worth keeping in mind, with so much SARS-CoV-2 “still circulating around,” cautions Tina Tan, a pediatrician and infectious-disease specialist at Northwestern University. Immunized people are at much lower risk of picking up the virus and passing it on. There still aren’t enough of them, though, to reliably tamp down spread; uptake of shots among young kids, too, is expected to be sluggish in the months to come. Even fully vaccinated families won’t be totally in the clear while our collective defenses remain weak.
That doesn’t mean Thanksgiving has to be a bust—or even a repeat of 2020, before the vaccines rolled out. The Bells will be cautiously gathering with a few loved ones; all the adults in attendance will be immunized and everyone will get tested beforehand. “Then they can come inside the house, mask off,” Taison Bell, Alain’s father, told me. None of those measures is completely reliable on its own; together, though, they’ll hopefully keep the virus out.
The road ahead might feel a little bumpy for Alain, who’s celebrating his 8th birthday at the end of November, a few days after his second shot. (He’s getting the gift of immunity this year, his father joked.) The Bells will do something special “around when he hits full vaccination,” Kristen said, “with something Alain hasn’t gotten to do in the last two years.” But Alain, who has asthma, which can make COVID-19 worse, knows that his own injections won’t wipe the slate clean for him, or those around him. Some people in his neighborhood have caught the virus even after getting vaccinated, and he understands that he could too.
Alain will keep masking, and treading carefully at school, and even a bit at home. His 3-year-old sister, Ruby, hasn’t yet been able to get a shot. (I asked her how she felt about Alain’s vaccine; she responded, almost imperceptibly, “Jealous.”) Until another regulatory green light comes, she will still be waiting, which means that her family will be too.

The number of COVID-19 hospitalizations among older Americans dropped significantly since the vaccine rollout at the start of the year, new federal data show.
Why it matters: The vaccines have worked extremely well for one of the most vulnerable demographics. Roughly 97% of people 65 and older have at least one vaccine dose, and more than 85% of that age group is fully vaccinated, according to the CDC.
Yes, but: Certain portions of the Medicare population continue to be more susceptible to severe COVID-19 and hospitalization than others.

Pfizer’s COVID-19 vaccine is nearly 91 percent effective at preventing symptomatic infections in children between ages 5 and 11, according to a study released by the FDA Oct. 22.
The study involved 2,268 children given COVID-19 vaccines that are one-third the dosage of the vaccines given to people ages 12 and up. They were given two doses spaced three weeks apart, the same as the adult version of the vaccine. It found that the children developed antibody levels just as strong as older children and adults given the full dosage.
The FDA’s Vaccines and Related Biological Products Advisory Committee is set to meet Oct. 26 to discuss the evidence and vote on whether to recommend FDA authorization for the shots in kids ages 5 to 11.
The CDC’s vaccine advisory panel is set to meet the first week of November to discuss recommending the shots for the age group. That means shots for kids ages 5 to 11 could be authorized in the first week of November. There are about 28 million children in the age group in the U.S.
The vaccines will come in orange capped vials to make them easily distinguishable from adult doses, according to ABC News.
Find the full study results here.

As the now ubiquitous Delta variant continues to mutate, it’s spawned a new descendant that’s spread in the U.K. and made its way to the U.S.
The Delta sublineage, known as AY.4.2, is characterized by two “S-gene mutations” on A222V and Y145H, both located on the gene that encodes the spike glycoprotein of SARS-CoV-2.
CDC Director Rochelle Walensky, MD, acknowledged during the White House’s latest COVID-19 Response Team press briefing that the AY.4.2 sublineage has been identified “on occasion” in the U.S. without increased frequency or clustering to date.
Since August, AY.4.2 with these mutations has appeared in a total of three cases in the U.S.: in California, North Carolina, and Washington, D.C., according to Outbreak.info, which collects COVID-19 sequencing data from GISAID, a global genomic data-sharing initiative.
“At this time, there is no evidence that the sub-lineage AY.4.2 impacts the effectiveness of our current vaccines or therapeutics, and we will continue to follow up,” Walensky said.
Experts think the new Delta sublineage is slightly more transmissible, but say it’s likely less worrisome than its predecessor Alpha or Delta variants, which made bigger jumps in transmissibility. There’s a level of uncertainty over its exact advantage in spreading, however.
“There was a bit of a hope that Delta had, ideally, reached a kind of bound in transmissivity, so that will be a bit of a disappointment,” said Francois Balloux, PhD, computational biologist at University College London and director of the UCL Genetics Institute, in an interview.
Balloux predicted that at some point, almost everyone will be exposed to the “already so bloody transmissible” Delta variant, which makes up around 80% of sequenced cases in the U.K. He said AY.4.2 could be up to 15% more transmissible.
A lower estimate comes from Christina Pagel, PhD, the director of University College of London’s Clinical Operational Research Unit. On Twitter, she said that AY.4.2 could be up to 10% more transmissible: “We don’t know if it’s (a bit) more transmissible than other Delta strains *or* if it just got caught up in some superspreader events that seeded it.” That is, a large gathering of people could have amplified the effect of a strain that wasn’t intrinsically better at spreading.
“No reason to think it’s more immune evasive & might well be nothing. Something to keep an eye on but not panic over,” Pagel added.
The CDC lists AY.1 and AY.2 in its COVID Data tracker, and AY lineages generally under its “Variants of Concern” classification, but does not list AY.4 or AY.4.2 specifically. Balloux said that in the U.K., unlike the U.S., the genetic sequencing effort is nationally centralized. This makes it easier to track variants more quickly and accurately.
AY.4.2 was first spotted this spring in the U.K., where it represents 14,247 cases for a cumulative prevalence of 1% there at the time of publication, according to Outbreak.info.
The U.K. Health Security Agency reported on October 15 that AY.4.2 “is currently increasing in frequency” and that it made up 6% of the sequences analyzed. Balloux estimated that a more up-to-date number would be 7% to 8% because of a week-long lag in sequencing.
Notably, AY.4.2 spreads despite being characterized by S-gene mutations that are not known to make the virus intrinsically more transmissible. “Fundamentally, these are two very boring mutations,” Balloux said.
He clarified that this strain of SARS-CoV-2 is not “Delta plus” because it lacks a different mutation that defined that sublineage.
COVID-19 cases have declined nationwide for the fourth consecutive week, according to the CDC’s COVID data tracker weekly review published Oct. 15.
Nine numbers to know:
Reported cases
1. The nation’s current seven-day case average is 84,555, a 12.5 percent decrease from the previous week’s average.
Hospitalizations
2. The current seven-day hospitalization average for Oct. 6-12 is 6,659, an 8.8 percent drop from the previous week’s average.
Vaccinations
3. About 218 million people — 65.6 percent of the total U.S. population — have received at least one dose of the COVID-19 vaccine, and more than 188.3 million people, or 56.7 percent of the population, have gotten both doses.
4. About 9.3 million booster doses in fully vaccinated people have been reported.
5. The seven-day average number of vaccines administered daily was 841,731 as of Oct. 14, a 11.3 percent decrease from the previous week.
Variants
6. Based on projections for the week ending Oct. 9, the CDC estimates the delta variant accounts for more than 99 percent of all U.S. COVID-19 cases.
Deaths
7. The current seven-day death average is 1,241, down 13.4 percent from the previous week’s average. Some historical deaths have been excluded from these counts, the CDC said.
Testing
8. The seven-day average for percent positivity from tests is 5.7 percent, down 4.1 percent from the previous week.
9. The nation’s seven-day average test volume for the week of Oct. 1-7 was about 1.49 million, down 5.4 percent from the prior week’s average.

Conventional wisdom says that if you’re vaccinated and you get a breakthrough infection with the coronavirus, you can transmit that infection to someone else and make that person sick.
But new evidence suggests that even though that may happen on occasion, breakthrough infections might not represent the threat to others that scientists originally thought.
Ross Kedl, an immunologist at the University of Colorado School of Medicine, will point out to anyone who cares to listen that basic immunology suggests the virus of a vaccinated person who gets infected will be different from the virus of an infected unvaccinated person.
That’s because vaccinated people have already made antibodies to the coronavirus. Even if those antibodies don’t prevent infection, they still “should be coating that virus with antibody and therefore helping prevent excessive downstream transmission,” Kedl says. And a virus coated with antibodies won’t be as infectious as a virus not coated in antibodies.
In Provincetown, Mass., this summer, a lot of vaccinated people got infected with the coronavirus, leading many to assume that this was an example of vaccinated people with breakthrough infections giving their infection to other vaccinated people.
Kedl isn’t convinced.
“In all these cases where you have these big breakthrough infections, there’s always unvaccinated people in the room,” he says.
In a recent study from Israel of breakthrough infections among health care workers, the researchers report that in “all 37 case patients for whom data were available regarding the source of infection, the suspected source was an unvaccinated person.”
It’s hard to prove that an infected vaccinated person actually was responsible for transmitting their infection to someone else.
“I have seen no one report actually trying to trace whether or not the people who were vaccinated who got infected are downstream — and certainly only could be downstream — of another vaccinated person,” Kedl says.
There’s new laboratory evidence supporting Kedl’s supposition. Initially, most vaccine experts predicted that mRNA vaccines like the ones made by Pfizer and Moderna that are injected into someone’s arm muscle would generate only the kinds of antibodies that circulate throughout the body.
But that might not be the whole story.
“I think what was the big surprise here is that the mRNA vaccines are going beyond that,” says Michal Caspi Tal, until recently an instructor at Stanford University’s Institute for Stem Cell Biology and Regenerative Medicine and now a visiting scientist at the Massachusetts Institute of Technology.
What Tal has found is that in addition to the circulating antibodies, there was a surprisingly large amount of antibodies in mucosal membranes in the nose and mouth, two of the primary entry points for the coronavirus.
Immunologist Jennifer Gommerman of the University of Toronto found this as well.
“This is the first example where we can show that a local mucosal immune response is made, even though the person got the vaccine in an intramuscular delivery,” Gommerman says.
If there are antibodies in the mucosal membranes, they would likely be coating any virus that got into the nose or throat. So any virus that was exhaled by a sneeze or a cough would likely be less infectious.
Gommerman says that until now, it seemed likely that a vaccine that was delivered directly to the mucosal tissue was the only way to generate antibodies in the nose or throat.
“Obviously a mucosal vaccination would be great too. But at least we’re not sitting ducks,” Gommerman says. “Otherwise everyone would be getting breakthrough infection.”
Now, these studies by Gommerman and Tal have yet to undergo peer review, and some have already suggested that the antibodies they have described may not confer true mucosal immunity.
But there’s other evidence that a vaccinated person’s breakthrough infection may not transmit efficiently to others.
Marion Pepper, an immunologist at the University of Washington, says a recent study from the Netherlands looked at how well virus from vaccinated people could infect cells in the lab.
Pepper says the answer was not well.
“If you actually isolate virus from people who are getting a secondary infection after being vaccinated, that virus is less good at infecting cells,” Pepper says. “It’s not known why. Is it covered with an antibody? Maybe. Has it been hit by some other kind of immune mediators, cytokines, things like that? Maybe. Nobody really knows. But the virus does seem to be less viable coming from a vaccinated person.”
More studies are emerging that suggest there’s something different about the virus coming from a vaccinated person, something that may help prevent transmission.
Whatever it is, the University of Colorado’s Kedl says it’s one more reason that getting vaccinated is a good idea.
“Because you’re going to be even more protected yourself. And you’re going to be better off protecting other people.”
Kedl says that’s what you call a win-win situation.

n addition to treating an influx of Covid-19 patients, many hospitals are struggling with what one administrator calls a “triple whammy” of financial burdens—stemming from plummeting revenue, higher labor costs, and reduced relief funds, Christopher Rowland reports for the Washington Post.
In areas with low vaccination rates, particularly in southern and rural communities, hospitals have been overwhelmed with Covid-19 patients, exacerbating labor shortages as workers burn out or leave for more lucrative positions, Rowland reports.
“The workforce issue is just dire,” Stacey Hughes, EVP of government relations and policy for the American Hospital Association (AHA), said. “The delta variant has wreaked significant havoc on hospitals and health systems.”
In Louisiana, Mary Ellen Pratt, CEO of St. James Parish Hospital, said many nurses quit due to the grueling conditions as Covid-19 cases spiked. “I didn’t have any extra money to incentivize my staff to pick up additional shifts,” she said. “This is coming out of bottom-line money I don’t have.”
Separately, Lisa Smithgall, SVP and chief nursing executive at Ballad Health, said the health system—which has 21 hospitals in eastern Tennessee and southwestern Virginia—has faced similar problems retaining staff amid Covid-19 surges.
“We knew we were at risk in our region because of where we live and because of our vaccination rate being so poor,” Smithgall said. “At one point, we were seeing four or five nurse resignations per week. They couldn’t do it again; they emotionally didn’t have it. They were so upset with our community.”
To fill in these growing gaps in their workforce, many hospitals have had to turn to costly contract workers, Rowland reports—a significant financial burden that further strains hospitals’ resources.
For example, Ballad Health went from hiring fewer than 75 contract nurses before the pandemic to 150 in August 2020 and 450 in August 2021. Moreover, according to Smithgall, contract nurses previously made double or triple what permanent staff nurses made, but now Ballad sometimes has to pay up to seven times as much for contract nurses as hospitals compete for workers to fill shifts.
Many hospitals, including those in areas with high vaccination rates, have delayed elective surgeries, a crucial source of revenue, amid nationwide surges in Covid-19 cases, Rowland reports—further compounding financial struggles for many organizations.
On Aug. 26, Ballad Health postponed a long list of elective surgeries—including hernia repair, cardiac and interventional radiology procedures, joint replacements, and nonessential spine surgery—to preserve space in its hospitals and conserve workers. Ballad is now allowing elective surgeries again, but only for a limited number of procedures that do not require overnight stays.
Similarly, St. Charles Health System in Oregon postponed elective surgeries in August “while we responded to a surge that was significantly greater and much more sudden than the surge in 2020,” Matt Swafford, the health system’s VP and CFO, said.
According to Swafford, the health system lost $5 million a week through August and September, around $1 million of which was repayment of emergency advances on Medicare reimbursements from last year.
“I don’t think anybody saw this level of surge coming in 2021 after what we saw in 2020,” he said. “We’re just not equipped to be able to simultaneously respond to the urgent needs of the community [for more typical surgeries and care] at the same time that a third of our beds are occupied by highly infective Covid patients.”
Further compounding the issue, according to Moody’s Investors Service, is that the provider relief funds that previously made up 43% of operating cash flow at nonprofit and government-run hospitals in the United States are now dwindling down.
In addition, the latest portion of provider relief funds to be distributed must be based on expenses incurred by hospitals before March 31, 2021, which don’t account for months of the delta surge, Rowland reports.
Premier, a group purchasing and technology company serving more than 4,000 hospitals and health systems, analyzed payroll data of 650 hospitals and found that U.S. hospitals have spent a total of $24 billion a year during the pandemic to cover excess labor costs, primarily for overtime and contract nurses. This was an increase of 63% from October 2019 to July 2021, Rowland reports, with hospitals in the Upper Midwest and across the South seeing the largest increases.
“It’s going to leave them huge deficits that they are going to have to work out of for years to come,” Michael Alkire, Premier’s CEO, said.
https://www.advisory.com/daily-briefing/2021/08/09/delta-surge
Last spring, my Advisory Board colleagues and I were optimistic that the United States could be trending toward a “good” outcome in the Covid-19 pandemic. But now, the delta variant is coursing through the country. And if you’re anything like me, you’re probably asking yourself just how worried we should be. When will we hit a peak and see hospitalizations—which are on the rise in many parts of the country—decline? Amid the constant headlines of case numbers, vaccine efficacy, mask mandates, and other Covid-19 news, I think it’s crucial to step back and ask: What factors really matter?
Let’s be very specific about which factors we should be following—and which we should deprioritize. Below, I’ve identified seven factors to pay close attention to and two factors that may be more distracting than helpful.
Your top resources for Covid-19 readiness
1. The transmissibility of the delta variant in the United States
One of the most striking factors underlying the delta surge is its heightened transmissibility—this is the most transmissible Covid-19 variant we have seen yet. The delta variant, B.1.617.2, now accounts for over 83% of new infections in the United States. And unlike past variants, this one is spreading among both vaccinated and unvaccinated individuals. In fact, CDC documents recently revealed that vaccinated individuals may spread the virus just as easily as unvaccinated people, given similar levels of viral load between the two groups.
The 6 biggest Covid-related myths we’ve seen, busted
There is also a third group of people that we know even less about in the context of the variant’s transmissibility: people who are unvaccinated but potentially have some degree of natural immunity from previous coronavirus infection. Nobody knows exactly how long their immunity will last and what levels of protection they have against the delta variant. But early research has indicated that natural immunity may not supply sufficient protection against the delta variant.
Understandably, this is all worrisome. But it is important to consider the effect of infection on different populations. And that brings us to our next factor.
2.Vaccine effectiveness against serious illness from delta—and uptake among unvaccinated individuals
No vaccine can provide 100% protection—and it’s important to remember that most vaccines are designed to prevent serious illness and death, NOT to prevent infection. That is why media reports about fully vaccinated individuals getting infected with the delta variant can be misleading. The important indicator to watch for is not necessarily the infection rate, but how many of those infections lead to serious illness or death. If a breakthrough infection is usually asymptomatic or mildly symptomatic, the main concern is spreading the variant to at-risk populations—namely, unvaccinated people and those with weakened immune systems or underlying medical conditions.
The bad news is, we don’t currently have great data on this. The latest CDC data showed that less than 0.004% of fully vaccinated individuals had a breakthrough case that led to hospitalization and less than 0.001% died from a breakthrough case of Covid-19. But CDC Director Rochelle Walensky later clarified that those numbers are based on data from January through June, meaning they do not take into account the worst of the delta variant surge, which picked up in earnest in late June and early July.
But there is some reason to be optimistic: Among the 469 breakthrough cases tracked from the Provincetown outbreak in early July, only four led to hospitalization—and there were zero deaths. And preliminary studies from around the globe suggest that all three vaccines available in the United States still offer protection from the delta variant: two doses of Pfizer-BioNTech is 88% effective at preventing symptomatic Covid-19 and 96% effective against hospitalization, a single dose of Moderna’s two-dose vaccine is 72% effective at preventing symptomatic Covid-19, and Johnson & Johnson’s single-dose vaccine is 85% effective at preventing severe disease. Even among those vaccinated individuals who do end up in the hospital, we can look at new data from Singapore showing that patients hospitalized due to the delta variant are less likely to require supplemental oxygen and clear the virus faster relative to unvaccinated patients. All of this is reassuring as the data suggests vaccines are largely keeping their promise to stave off serious disease, hospitalizations, and death.
Radio Advisory episode: Vaccinating the globe, the ultimate systemness challenge
This early research suggests that vaccine uptake will remain one of the most crucial factors in determining how worrisome the current surge is—and how it will impact the health care delivery system. After several months of decline, the national vaccination rate is now at its highest level in over a month, and we are observing the most notable increases in vaccine uptake in states with the highest case rates.
3. Vaccine immunity duration
The delta variant has not only prompted a renewed push to increase vaccinations among the previously unvaccinated, but it has also raised questions about the duration of immunity among those who may have been vaccinated several months ago. While the latest data on vaccine duration is not specific to the delta variant, it does suggest that overall efficacy may begin to decline around the six-month mark.
That information, coupled with the increase in breakthrough infections since the delta variant emerged, has accelerated the debate over whether booster shots are needed. Federal regulators are currently researching whether a booster shot is required, and recently announced plans to accelerate extra vaccine doses to immunocompromised individuals. We expect that this is an area where the research will continue to evolve quickly—researchers are learning more on a week-by-week basis. We’ll be keeping a close eye on what the latest research says and how the federal government responds in developing a plan for potential booster shots.
4. Severe Covid-19 cases among children under 12
Rates of Covid-19 infection and severe illness have been relatively low among children. However, it’s worth noting that small numbers of children have been hospitalized from the virus, and it can cause long-term side effects like MIS-C and “long Covid-19.” CDC has not yet released data showing delta variant symptoms among children, but some children’s hospitals have reported increases in hospitalizations related to the delta variant.
Webinar series: ‘Stay Up to Date’ on the latest with Covid-19
Pfizer and Moderna are in the process of clinical trials testing the safety of their vaccines for children under 12. But it may be months before those trials lead to decisions, and children in some parts of the country have already begun to return to school in person. Without a vaccine, a child’s only practical defense against spreading and getting the virus is following public health guidelines like hand washing and mask wearing. But some states—Iowa, Florida, Montana, Arizona, and North Dakota—have passed laws that prevent local governments from mandating masks. Many more states have passed laws making mask mandates harder to implement, like the Kansas law allowing citizens to sue their local government over Covid-19 restrictions.
As school resumes in the United States, we will have to pay close attention to the transmissibility Covid-19 among unvaccinated children, the severity of such cases among children, and the potential long-term effects.
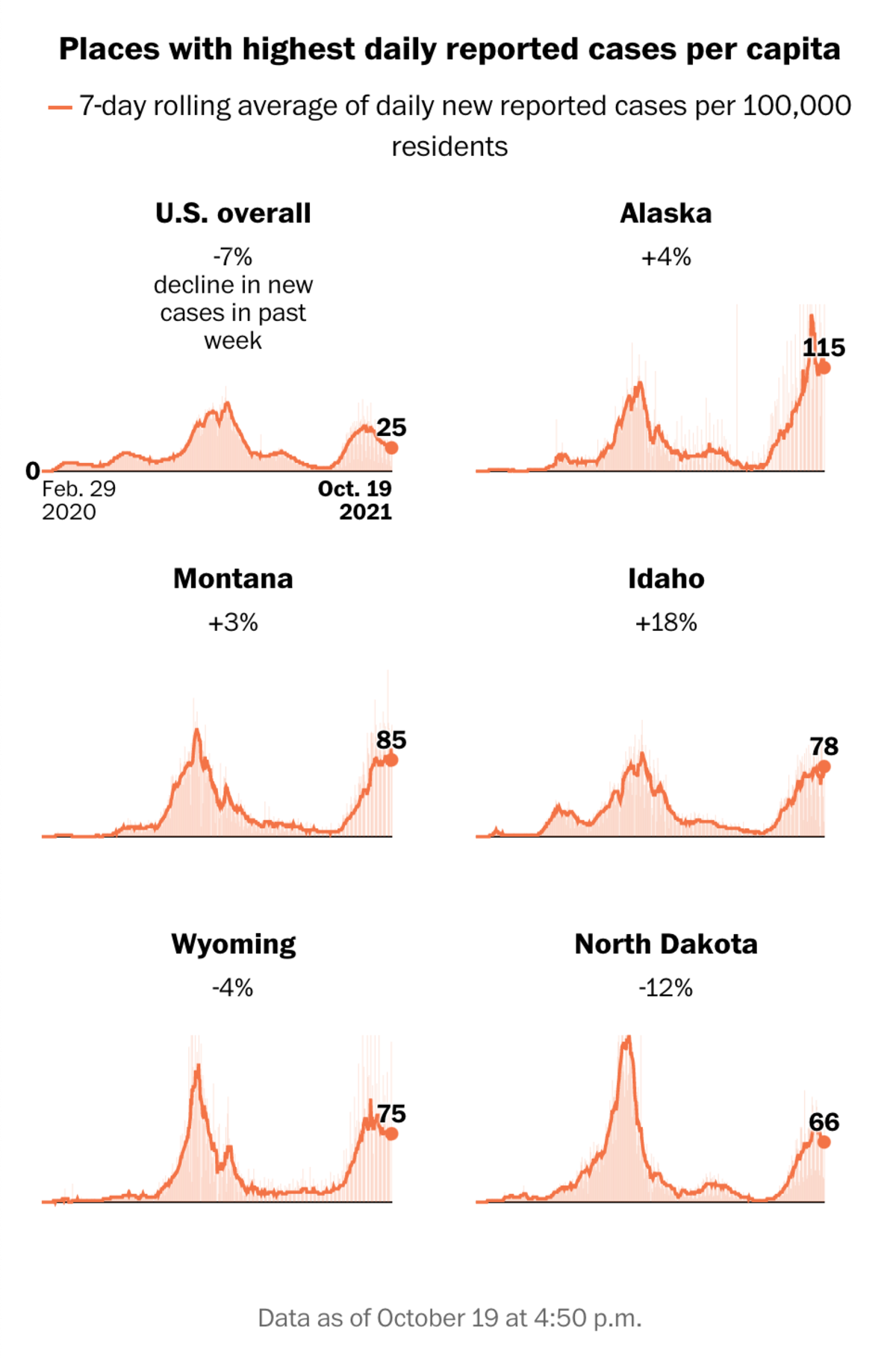
5. Hospitalization rates, particularly at the local level
Plain and simple—the higher the number of hospitalizations, the more worried we should be. Hospitalizations tell us how many people have more severe cases of Covid-19. But they also tell us what level of strain the U.S. health care system is under.
So, what are we seeing right now? CDC’s latest 7-day average shows nearly 50,000 people hospitalized across the United States, which is similar to rates seen last summer. Unsurprisingly, there is regional variation, with some states experiencing worse flareups than others. Most of the highly impacted regions have low vaccination rates: On Monday, there were more Covid-19 hospitalizations in Florida than at any other time in the pandemic. In Louisiana, hospitalizations have spiked to “never-before-seen levels,” breaking the previous record set in January—and leading to expectations that facilities will be overwhelmed again. As we move forward, we may see “hyperlocal outbreaks,” where low-vaccination regions surrounded by high vaccination areas could end up with concentrated outbreaks.
Toolkit: Covid-19 vaccine communications readiness assessment
It’s important to keep an eye on local vaccination rates because it’s clear that unvaccinated individuals and communities are more vulnerable. But that doesn’t mean communities with higher vaccination rates are immune. Given the fact that there is more interconnectedness than ever between communities today, and the fact that we haven’t achieved true herd immunity even in areas with relatively high vaccination rates, even “highly” vaccinated communities could see outbreaks. For example, intensive care units are filling up with Covid-19 patients in Santa Monica, California, where roughly 80% of residents are vaccinated.
At this point, it seems clear that there will be a heightened strain on hospitals relative to the previous few months of “calm”—and data from abroad suggests it may get worse before it gets better.
6. Covid-19 trends in ‘bellwether countries’
Recent decreases of Covid-19 cases in India and the U.K. are a heartening sign that recovery from a delta surge is possible. In India, cases peaked at over 400,000 a day in May. Last week, they experienced roughly 39,000 daily cases with a 48% decrease in the daily death count—a stark reduction. In the U.K., cases have dropped from roughly 47,000 in mid-July to nearly 27,000 the first week of August, even after their government lifted nearly all Covid-19 restrictions.
Sudden spikes may have been fueled by mass congregations of people: the EuroCup in England, April election rallies in India, and fourth of July celebrations in the United States. The subsequent declines in India and the UK suggest that delta could move through a crowd quickly and limiting large crowd gatherings could help stem the spread. It’s also possible that herd immunity is behind the rapid decrease, due to the combination of vaccination rates and infection levels. That could be a hopeful sign for regions of the U.S. that are struggling with high infection rates now but seeing increases in vaccinations.
But we’ll want to continue watching the research closely. Scientists aren’t yet sure exactly what lead to the rapid declines, meaning we can’t be entirely confident that the United States. will follow the same trajectory as the U.K. and India.
7. Global vaccination rates—and the emergence of new variants
The United States is just one part of an interconnected world. It impacts (and is impacted by) global trends in health. It’s overwhelmingly clear—everything we do is a collaboration, and moving through this pandemic is no exception.
Should you mandate a Covid-19 vaccine for your staff? Ask these 5 questions first.
To date, about 27% of the global population has been vaccinated. The latest vaccination rate is roughly 42.5 million doses per day, which means it will take at least another five months to cover 75% of the world’s population. Just a few short months ago, the global vaccination rate had us estimating we’d need more than 4.6 years to achieve global herd immunity with two-dose vaccine regimens.
Five months is better than 4.6 years, but that assumes the vaccination rate will remain the same. With ongoing vaccine hesitancy and inequitable access in low-resource countries, we shouldn’t just assume this will be the case. If we see a drop in global vaccination rates, we will see an extension in the time it takes to reach a semblance of global herd immunity. The more time we spend in this phase, the more opportunities the coronavirus has to mutate into the next variant. And the next variant could be even more transmissible and deadlier than the delta.
Even with President Biden’s pledge to donate half a billion Pfizer vaccines to 92 low- and lower middle-income countries by June 2022, stronger efforts are needed to see a faster global impact. And efforts to increase the global vaccination rates could mean trade-offs elsewhere. For example, the World Health Organization has pled for a moratorium on booster shots until September to allow lower-resourced nations ability to receive initial vaccinations.
Knowing what not to focus on is just as important as knowing what to focus on. And there are two factors in particular that have grabbed a lot of the headlines—but that actually tell us very little without additional context.
1. Covid-19 case counts
Case counts alone are no longer sufficient for tracking the severity of any variant, or the virus as a whole. But with the advent of the vaccine and better understanding of how to treat the virus, the calculus has changed, and so too should the metrics we give our attention to. It’s been clear for some time that the goal is not necessarily to eliminate Covid-19 (in fact, research increasingly suggests it’s highly likely to become endemic). Instead, we should aim to protect against severe illness and ensure our system has enough capacity to treat sick patients. Severity of illness—and corresponding hospitalization rates—are far more important metrics to track at this point.
‘The Never Again Plan’: Moderna CEO Stéphane Bancel wants to stop the next Covid-19—before it happens
As detailed above, the latest research continues to suggest that vaccines are highly protective in preventing severe illness, even against the delta variant. So as more people get vaccinated, case count numbers are likely to become less accurate. They run the risk of either overestimating the problem (if most cases are only mildly symptomatic) or underestimating the problem (if we miss a lot of asymptomatic people who can still spread the virus to the more vulnerable).
2. The percentage of total infections and hospitalizations that are breakthrough cases
We’ve all seen the recent headlines highlighting the large numbers and percentage of breakthrough infections. Here’s the thing to remember: This is exactly what we would expect to see as vaccination rates increase. The number of breakthrough infections and hospitalizations will increase as more people get vaccinated. The outbreak in Provincetown highlights this well. Yes, roughly 75% of cases were among vaccinated individuals, but most individuals there were vaccinated. Naturally, a high percentage of the cases would be “breakthrough.” And remember, very few were hospitalized and no one died from a breakthrough case as a result of that outbreak.
Breakthrough infections alone are not a bad thing. Breakthrough illness, on the other hand, is more worrisome. If we see the rates of breakthrough illness increase, then it’s time to worry a bit more.
It’s easy to feel overwhelmed with the constant updates related to Covid-19. While there are more than seven factors you could follow, I believe these are the most important right now. And the clear thread that runs through all of these is that vaccines remain one of the key solutions to move through this pandemic. It’s becoming clearer that Covid-19 is unlikely to go away—new variants will arise and so will respective public health measures. But if there is one thing I can confidently say right now, it is that the more vaccinations that are administered in the United States and around the world, the less worried we can all be.
