The Supreme Court on Friday upheld a key Affordable Care Act requirement that insurance companies cover certain preventative measures recommended by an expert panel.
Justices upheld the constitutionality of the provision in a 6-3 decision and protected access to preventative care for about 150 million Americans.
The justices found that the secretary of the Department of Health and Human Services has the power to appoint and fire members of the U.S. Preventative Services Task Force (USPSTF).
The cases started when a small business in Texas and some individuals filed a lawsuit against the panel’s recommendation that pre-exposure prophylaxis (PreP) for HIV be included as a preventative care service.
They argued that covering PreP went against their religious beliefs and would “encourage homosexual behavior, intravenous drug use, and sexual activity outside of marriage between one man and one woman.”
The plaintiffs further argued that the USPSTF mandates are unconstitutional because panel members are “inferior officers” who are not appointed by the president or confirmed by the Senate.
While the panel is independent, they said that since their decisions impact millions of people members should be confirmed.
A U.S. district judge in 2023 ruled that all preventative-care coverage imposed since the ACA was signed into law areinvalid and a federal appeals court judge ruled in agreement last year.
The Biden administration appealed the rulings to the Supreme Court, and the Trump administration chose to defend the law despite its long history of disparaging Obamacare.
Though public health groups celebrated the ruling Friday, some noted another potential outcome.
“While this is a foundational victory for patients, patients have reason to be concerned that the decision reaffirms the ability of the HHS secretary, including our current one, to control the membership and recommendations of the US Preventive Services Task Force that determines which preventive services are covered,” Anthony Wright, executive director of Families USA, said in a statement.
“We must be vigilant to ensure Secretary Kennedy does not undo coverage of preventive services by taking actions such as his recent firing of qualified health experts from the CDC’s independent vaccine advisory committee and replacing them with his personal allies.”
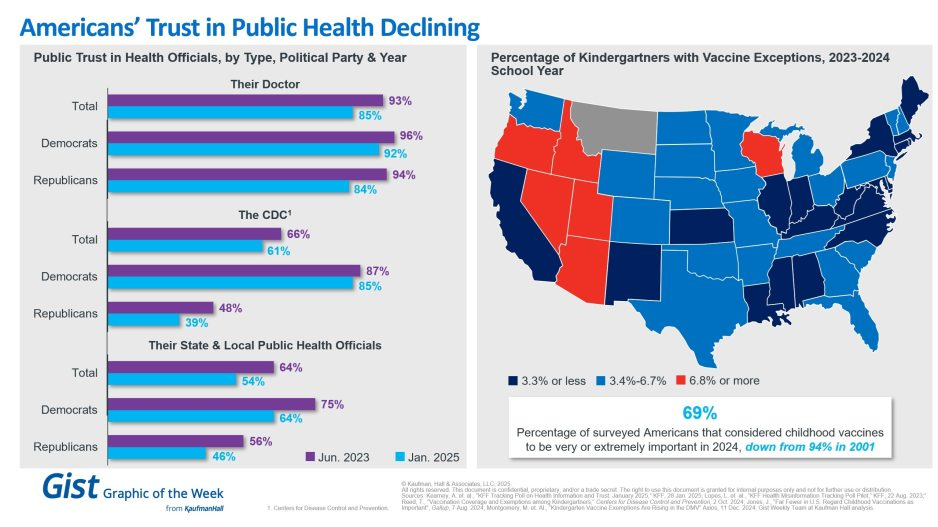
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
Last week, President-elect Donald Trump announced that Robert F. Kennedy, Jr. would be his nominee for Secretary of Health and Human Services (HHS). He followed this up on Tuesday with his selection of Dr. Mehmet Oz as his nominee for the Centers for Medicare and Medicaid Services (CMS) Administrator. If confirmed, the two men would replace Xavier Becerra and Chiquita Brooks-LaSure, respectively.
Kennedy, who ended his independent presidential campaign and endorsed Trump in August, has become known for his heterodox views on public health, including vaccine skepticism and opposition to water fluoridization.
Dr. Oz, first famous as a TV personality and more recently a Republican candidate for Pennsylvania Senator, is a strong proponent of Medicare Advantage, having co-authored an op-ed advocating for “Medicare Advantage for All” in 2020.
The Gist:
These nominees, especially Kennedy, hold a number of personal beliefs at odds with the public health consensus.
They are both likely to be confirmed, however, as the last cabinet nominee to be rejected by the Senate was John Tower in 1989. (This does not include nominees who have chosen to withdraw themselves from consideration, as former Representative Matt Gaetz has just done.)
Should they be confirmed, they will be responsible for implementing not their own but President Trump’s agenda, the specific priorities of which also remain relatively undefined.
However, possible consensus points between Trump and his nominees include public health cuts and deregulation, greater scrutiny of pharmaceutical companies, and a favoring of Medicare Advantage over traditional Medicare.
A surge in COVID-19 infections has swept the country this summer, upending travel plans and bringing fevers, coughs and general malaise. It shows no immediate sign of slowing.
While most of the country and the federal government has put the pandemic in the rearview mirror, the virus is mutating and new variants emerging.
Even though the Centers for Disease Control and Prevention (CDC) no longer tracks individual infection numbers, experts think it could be the biggest summer wave yet.
So far, the variants haven’t been proven to cause a more serious illness, and vaccines remain effective, but there’s no certainty about how the virus may yet change and what happens next.
The highest viral activity right now is in the West, according to wastewater data from the CDC, but a “high” or “very high” level of COVID-19 virus is being detected in wastewater in almost every state. And viral levels are much higher nationwide than they were this time last year and started increasing earlier in the summer.
Wastewater data is the most reliable method of tracking levels of viral activity because so few people test, but it can’t identify specific case numbers.
Part of the testing decline can be attributed to pandemic fatigue, but experts said it’s also an issue of access.Free at-home tests are increasingly hard to find. The government isn’t distributing them, and private insurance plans have not been required to cover them since the public health emergency ended in 2023.
COVID has spiked every summer since the start of the pandemic. Experts have said the surge is being driven by predictable trends like increased travel and extreme hot weather driving more people indoors, as well as by a trio of variants that account for nearly 70 percent of all infections.
Vaccines and antivirals can blunt the worst of the virus, and hospital are no longer being overwhelmed like in the earliest days of the pandemic.
But there remains a sizeable number of people who are not up-to-date on vaccinations. There are concerns that diminished testing and low vaccination rates could make it easier for more dangerous variants to take hold.
“One of the things that’s distinctive about this summer is that the variants out there are extraordinarily contagious, so they’re spreading very, very widely, and lots of people are getting mild infections, many more than know it, because testing is way down,” said William Schaffner, a professor of preventive medicine and infectious diseases at Vanderbilt University.
That contagiousness means the virus is more likely to find the people most vulnerable — people over 65, people with certain preexisting conditions, or those who are immunocompromised.
In a July interview with the editor-in-chief of MedPage Today, the country’s former top infectious diseases doctor, Anthony Fauci, said people in high-risk categories need to take the virus seriously, even if the rest of the public does not.
“You don’t have to immobilize what you do and just cut yourself off from society,” Fauci said. “But regardless of what the current recommendations are, when you are in a crowded, closed space and you are an 85-year-old person with chronic lung disease or a 55-year-old person who’s morbidly obese with diabetes and hypertension, then you should be wearing a mask when you’re in closed indoor spaces.”
Schaffner said hospitalizations have been increasing in his region for at least the past five weeks, which surprised him.
“I thought probably they had peaked last week. Wrong. They went up again this week. So at least locally, we haven’t seen the peak yet. I would have expected this summer increase … to have plateaued and perhaps start to ease down. But we haven’t seen that yet,” he said.
Still, much of the country has moved on from the pandemic and is reacting to the surge with a collective shrug. COVID-19 is being treated like any other respiratory virus, including by the White House.
President Biden was infected in July. After isolating at home for several days and taking a course of the antiviral Paxlovid, he returned to campaign trial.
Biden is 81, meaning he’s considered high risk for severe infection. He received an updated coronavirus vaccine in September, but it’s not clear if he got a second one, which the CDC recommends for older Americans.
Updated vaccines that target the current variants are expected to be rolled out later this fall, and the CDC recommends everyone ages 6 months and older should receive one.
As of May, only 22.5 percent of adults in the United States reported having received the updated 2023-2024 vaccine that was released last fall and tailored to the XBB variant dominant at that time.
The immunity from older vaccines wanes over time, and while it doesn’t mean people are totally unprotected, Schaffner said, the most vulnerable should be cautious. Many people being infected now have significantly reduced immunity to the current mutated virus, but reduced immunity is better than no immunity.
People with healthy immune systems and who have previously been vaccinated or infected are still less likely to experience the more severe infections that result in hospitalization or death.
Almost “none of us are naive to COVID, but the people where the protection wanes the most are the most frail, the immunodeficient, the people with chronic underlying illnesses,” Schaffner said.
As seasonal virus activity surges across the United States, experts stress the importance of preventive measures – such as masking and vaccination – and the value of treatment for those who do get sick.
Tens of thousands of people have been admitted to hospitals for respiratory illness each week this season. During the week ending December 23, there were more than 29,000 patients admitted with Covid-19, about 15,000 admitted with the flu and thousands more with respiratory syncytial virus, or RSV, according to data from the US Centers for Disease Control and Prevention.
Nationally, Covid-19 levels in wastewater, a leading measure of viral transmission, are very high – higher than they were at this time last year in every region, CDC data shows. Weekly emergency department visits rose 12%, and hospitalizations jumped about 17% in the most recent week.
And while Covid-19 remains the leading driver of respiratory virus hospitalizations, flu activity is rising rapidly. The CDC estimates that there have been more than 7 million illnesses, 73,000 hospitalizations and 4,500 deaths related to the flu this season, and multiple indicators are high and rising.
RSV activity is showing signs of slowing in some parts of the US, but many measures, including hospitalization rates, remain elevated. Overall, young children and older adults are most affected.
“It’s a wave of winter respiratory pathogens, especially respiratory viruses. So it’s Covid, it’s flu, and we can’t diminish the importance of RSV,” said Dr. Peter Hotez, dean of the National School of Tropical Medicine at the Baylor College of Medicine. “So it’s a triple threat, and arguably a fourth threat because we also have pneumococcal pneumonia, which complicates a lot of these virus infections.”
Respiratory virus activity has been on the rise for weeks. Now, flu-like activity is high or very high in two-thirds of the United States, including California, New York City and Washington, as well as throughout the South and Northeast, according to the CDC.
“Remember, all of these numbers are before people got together for the holidays,” Hotez said. “So don’t be disappointed or surprised that we even see a bigger bump as we head into January.”
Vaccines can help prevent severe illness and death, but uptake remains low this season – despite a historic first, with vaccines available to protect against each of the three major viruses. Just 19% of adults and 8% of children have gotten the latest Covid-19 vaccine, and 17% of adults 60 and older have gotten the new RSV vaccine, CDC data shows. Less than half of adults and children have gotten the flu vaccine this season.
“We have, as a population, underutilized both influenza and the updated Covid vaccines, unfortunately,” said Dr. William Schaffner, an infectious disease expert at Vanderbilt University. “But it’s not too late to get vaccinated, because these viruses are going to be around for a while yet.”
According to the CDC, hospital bed capacity remains “stable” nationally, including within intensive care units. But with high levels of respiratory viruses, hospitals in at least five states are returning to requiring masks.
Mass General Brigham spokesman Timothy Sullivan said it will require masking for health-care staff who interact directly with patients starting Tuesday, and patients and visitors will be “strongly encouraged to wear a facility-issued mask.”
In Wisconsin, UW Health and UnityPoint Health – Meriter have expanded mask policies to cover more people. UW requires all staff, patients and visitors to wear a mask for patient interactions in clinic settings, including waiting areas and exam rooms.
UnityPoint Health – Meriter says masks continue to be required for team members and visitors in patient rooms.
Bellevue, a public hospital in New York City, said on social media last week that it had reinstated its mandatory masking policy due to an uptick in respiratory illnesses.
In Pennsylvania, the University of Pittsburgh Medical Center has required everyone to wear a mask when entering or inside since December 20. The systemwide masking policies were adjusted to “address the increase of respiratory virus cases” but may change when there is a “marked decrease in respiratory health cases,” according to the health care system.
An order posted last week by the Los Angeles County Health Officer requires all health-care personnel and visitors to mask while in contact with patients or in patient-care areas, based on the CDC’s categorization of Covid-19 hospital admission levels.
During the week ending December 23, more than 230 US counties were considered to have “high” levels of Covid-19 hospital admissions, defined by the CDC by at least 20 new hospital admissions for every 100,000 people. Nearly a thousand other counties, about a third of the country, have “medium” Covid-19 hospital admission levels, with at least 10 admissions for every 100,000 people.
Vaccines and masks can help reduce the risk of severe illness before getting sick, but treatments are also available to help prevent people from getting very sick if they do become infected.
Antiviral treatments for Covid-19, such as Paxlovid, and flu, such as Tamiflu, can be especially helpful for people who are more likely to get very sick, including people who are 50 or older and those with certain underlying conditions, such as a weakened immune system, heart disease, obesity, diabetes or chronic lung disease.
“If more people at higher risk for severe illness get treatment in a timely manner, we will save lives,” the CDC said in a recent blog post. But “not enough people are taking them.”
Seasonal respiratory virus activity can be hard to predict, but CDC forecasts suggest that hospitalization rates will continue at elevated levels for weeks and that this season, overall, will probably result in a similar number of hospitalizations as last season.
“One of the ways to help us all go into a happy new year is for us to be as protected as we can against these viruses,” Schaffner said.
“Of course, I continue to recommend vaccination, prudent use of the mask by high-risk people and, should you become sick, do not go to work and spread the virus further. Call your health care provider, because you may have some treatment available that will get you healthier sooner.”
Two pioneers of mRNA research — the technology that helped the world tame the virus behind the Covid-19 pandemic — won the 2023 Nobel Prize in medicine or physiology on Monday.
Overcoming a lack of broader interest in their work and scientific challenges, Katalin Karikó and Drew Weissman made key discoveries about messenger RNA that enabled scientific teams to start developing the tool into therapies, immunizations, and — as the pandemic spread in 2020 — vaccines targeting the SARS-CoV-2 coronavirus. Moderna and the Pfizer-BioNTech partnership unveiled their mRNA-based Covid-19 shots in record time thanks to the foundational work of Karikó and Weissman, helping save millions of lives.
Karikó, a biochemist, and Weissman, an immunologist, performed their world-changing research on the interaction between mRNA and the immune system at the University of Pennsylvania, where Weissman, 64, remains a professor in vaccine research. Karikó, 68, who later went to work at BioNTech, is now a professor at Szeged University in her native Hungary, and is an adjunct professor at Penn’s Perelman School of Medicine.
The duo will receive 11 million Swedish kronor, or just over $1 million. Their names are added to a list of medicine or physiology Nobel winners that prior to this year included 213 men and 12 women.
The award was announced by Thomas Perlmann, secretary general of Nobel Assembly, in Stockholm. Perlmann said he had spoken to both laureates, describing them as grateful and surprised even though the pair has won numerous awards seen as precursors and had been tipped as likely Nobel recipients at some point.
Every year, the committee considers hundreds of nominations from former Nobel laureates, medical school deans, and prominent scientists from fields including microbiology, immunology, and oncology. Members try to identify a discovery that has altered scientists’ understanding of a subject. And according to the criteria laid out in Alfred Nobel’s will, that paradigm-shifting discovery also has to have benefited humankind.
The Nobel committee framed Karikó and Weissman’s work as a prime example of complementary expertise, with Karikó focused on RNA-based therapies and Weissman bringing a deep knowledge about immune responses to vaccines.
But it was not an easy road for the scientists. Karikó encountered rejection after rejection in the 1990s while applying for grants. She was even demoted while working at Penn, as she toiled away on the lower rungs of academia.
But the scientists persisted, and made a monumental discovery published in 2005 based on simply swapping out some of the components of mRNA.
With instructions from DNA, our cells make strands of mRNA that are then “read” to make proteins. The idea underlying an mRNA vaccine then is to take a piece of mRNA from a pathogen and slip it into our bodies. The mRNA will lead to the production of a protein from the virus, which our bodies learn to recognize and fight should we encounter it again in the form of the actual virus.
It’s an idea that goes back to the 1980s, as scientific advances allowed researchers to make mRNA easily in their labs. But there was a problem: The synthetic mRNA not only produced smaller amounts of protein than the natural version in our cells, it also elicited a potentially dangerous inflammatory immune response, and was often destroyed before it could reach target cells.
Karikó and Weissman’s breakthrough focused on how to overcome that problem. mRNA is made up of four nucleosides, or “letters”: A, U, G, and C. But the version our bodies make includes some nucleosides that are chemically modified — something the synthetic version didn’t, at least until Karikó and Weissman came along. They showed that subbing out some of the building blocks for modified versions allowed their strands of mRNA to sneak past the body’s immune defenses.
While the research did not gain wide attention at the time, it did catch the attention of scientists who would go on to found Moderna and BioNTech. And now, nearly 20 years later, billions of doses of mRNA vaccines have been administered.
For now, the only authorized mRNA products are the Covid-19 shots. But academic researchers and companies are exploring the technology as a potential therapeutic platform for an array of diseases and are using it to develop cancer vaccines as well as immunizations against other infectious diseases, from flu to mpox to HIV. An mRNA vaccine is highly adaptable compared to earlier methods, which makes it easier to alter the underlying recipe of the shot to keep up with viral evolution.
As she gained global fame, Karikó has been open about the barriers she encountered in her scientific career, which raised broader issues about the challenges women and immigrants can face in academia. But she’s said she always believed in the potential of her RNA research.
“I thought of going somewhere else, or doing something else,” Karikó told STAT in 2020, recalling the moment she was demoted. “I also thought maybe I’m not good enough, not smart enough. I tried to imagine: Everything is here, and I just have to do better experiments.”
On Monday, the Food and Drug Administration authorized new COVID vaccines from Moderna and Pfizer-BioNTech, and the Centers for Disease Control and Prevention followed Tuesday by recommending the shots be given as a single dose for most people five years of age and older. Children older than six months but younger than five, as well as completely unvaccinated people of any age, may be eligible for multiple doses.
These vaccines were formulated to target the XBB.1.5. variant,
which was the dominant strain in January but has since receded, although initial results suggest they remain effective against all currently circulating variants. Pharmacies and healthcare providers are expected to have the updated vaccines available by early next week.
The Gist: Due to the end of the COVID public health emergency in May, this COVID vaccination campaign will be the first not directly bankrolled by the federal government.
While insurers are still required to cover vaccinations without cost-sharing, the uninsured may find free shots, which the Biden administration says it will still provide at certain locations, harder to access.
Unlike past COVID boosters, reframing this shot as an annual vaccine that patients receive along with their flu shots should help with the rollout, as around 50 percent of Americans got a flu shot in 2022 while only 17 percent received the bivalent COVID booster.
With COVID cases and hospitalizations currently rising, promoting widespread uptake is critical to dampening a likely winter COVID spike.
However, public health officials will have to overcome many Americans’ wearied indifference toward COVID to motivate them to get vaccinated.