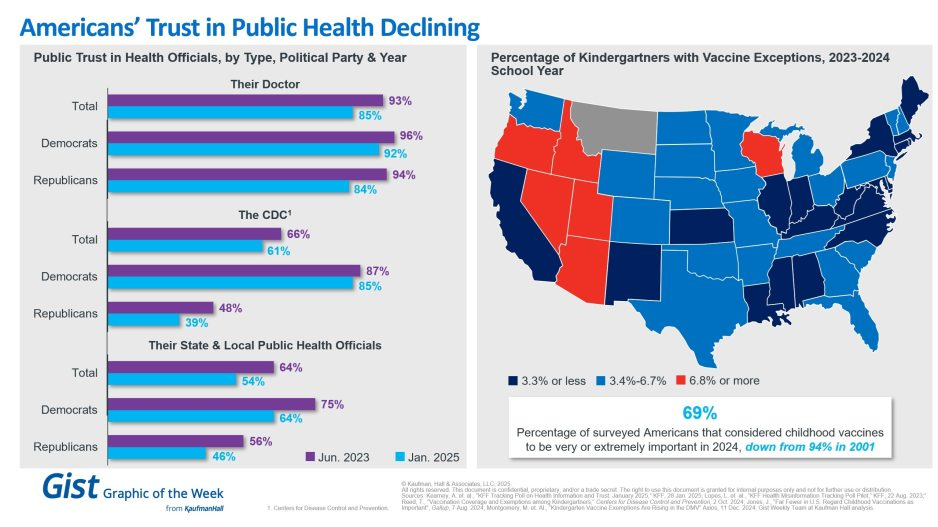
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
Albert Einstein determined that time is relative. And when it comes to healthcare, five years can be both a long and a short amount of time.
In August 2018, I launched the Fixing Healthcare podcast. At the time, the medium felt like the perfect auditory companion to the books and articles I’d been writing. By bringing on world-renowned guests and engaging in difficult but meaningful discussions, I hoped the show would have a positive impact on American medicine. After five years and 100 episodes, now is an opportune time to look back and examine how healthcare has improved and in what ways American medicine has become more problematic.
Here’s a look at the good, the bad and the ugly since episode one of Fixing Healthcare:
The Good
Drug breakthroughs and government actions headline medicine’s biggest wins over the past five years.
At first, health experts expressed doubts that Pfizer, Moderna and others could create a safe and effective Covid-19 vaccine with messenger RNA (mRNA) technology. After all, no one had succeeded in more than two decades of trying.
Thanks in part to Operation Warp Speed, the government-funded springboard for research, our nation produced multiple vaccines within less than a year. Previously, the quickest vaccine took four years to develop (mumps). All others required a minimum of five years.
The vaccines were pivotal in ending the coronavirus pandemic, and their success has opened the door to other life-saving drugs, including those that might prevent or fight cancer. And, of course, our world is now better prepared for when the next viral pandemic strikes.
Weight-Loss Drugs
Originally designed to help patients manage Type 2 diabetes, drugs like Ozempic have been helping people reverse obesity—a condition closely correlated with diabetes, heart disease and cancer.
For decades, America’s $150 billion a year diet industry has failed to curb the nation’s continued weight gain. So too have calls for increased exercise and proper nutrition, including restrictions on sugary sodas and fast foods.
In contrast, these GLP-1 medications are highly effective. They help overweight and obese people lose 15 to 25 pounds on average with side effects that are manageable for nearly all users.
The biggest stumbling block to their widespread use is the drug’s exorbitant price (upwards of $16,000 for a year’s supply).
Drug-Pricing Laws
With the Inflation Reduction Act of 2022, Congress took meaningful action to lower drug prices, a move the CBO estimates would reduce the federal deficit by $237 billion over 10 years.
It’s a good start. Americans today pay twice as much for the same medications as people in Europe largely because of Congressional legislation passed in 2003.
That law, the Medicare Prescription Drug Price Negotiation Act, made it illegal for Health and Human Services (HHS) to negotiate drug prices with manufacturers—even for the individuals publicly insured through Medicare and Medicaid.
Now, under provisions of the new Inflation Reduction Act, the government will be able to negotiate the prices of 10 widely prescribed medications based on how much Medicare’s Part D program spends. The lineup is expected to include prescription treatments for arthritis, cancer, asthma and cardiovascular disease. Unfortunately, the program won’t take effect until 2026. And as of now, several legal challenges from both drug manufacturers and the U.S. Chamber of Commerce are pending.
The Bad
Spiking costs, ongoing racial inequalities and millions of Americans without health insurance make up three disappointing healthcare failures of the past five years.
Cost And Quality
The U.S. spends nearly twice as much on healthcare per citizen as other countries, yet our nation lags 10 of the wealthiest countries in medical performance and clinical outcomes. As a result, Americans die younger and experience more complications from chronic diseases than people in peer nations.
As prices climb ever-higher, at least half of Americans can’t afford to pay their out-of-pocket medical bills, which remain the leading cause of U.S. bankruptcy. And with rising insurance premiums alongside growing out-of-pocket expenses, more people are delaying their medical care and rationing their medications, including life-essential drugs like insulin. This creates a vicious cycle that will likely prolong today’s healthcare problems well into the future.
Health Disparities
Inequalities in American medicine persist along racial lines—despite action-oriented words from health officials that date back decades.
Today, patients in minority populations receive unequal and inequitable medical treatment when compared to white patients. That’s true even when adjusting for differences in geography, insurance status and socioeconomics.
Racism in medical care has been well-documented throughout history. But the early days of the Covid-19 pandemic provided several recent and deadly examples. From testing to treatment, Black and Latino patients received both poorer quality and less medical care, doubling and even tripling their chances of dying from the disease.
The problems can be observed across the medical spectrum. Studies show Black women are still less likely to be offered breast reconstruction after mastectomy than white women. Research also finds that Black patients are 40% less likely to receive pain medication after surgery. Although technology could have helped to mitigate health disparities, our nation’s unwillingness to acknowledge the severity of the problem has made the problem worse.
Uninsurance
Although there are now more than 90 million Americans enrolled in Medicaid, there are still 30 million people without any health insurance. This disturbing reality comes a full decade after the passage of the Affordable Care Act.
On Capitol Hill, there is no plan in place to reduce the number of uninsured.
Moreover, many states are looking to significantly rollback their Medicaid enrollment in the post-Covid era. Kaiser Family Foundation estimates that between 8 million and 24 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provisions implemented during the pandemic. Without coverage, people have a harder time obtaining the preventive services they need and, as a result, they suffer more chronic diseases and die younger.
The Ugly
An overall decrease in longevity, along with higher maternal mortality and a worsening mental-health crisis, comprise the greatest failures of U.S. healthcare over the past five years.
Life Expectancy
Despite radical advances in medical science over the past five years, American life expectancy is back to where it was at the turn of the 20th century, according to CDC data.
Alongside environmental and social factors are a number of medical causes for the nation’s dip in longevity. Research demonstrated that many of the 1 million-plus Covid-19 deaths were preventable. So, too, was the nation’s rise in opioid deaths and teen suicides.
Regardless of exact causation, Americans are living two years less on average than when we started the Fixing Healthcare podcast five years ago.
Maternal Mortality
Compared to peer nations, the United States is the only country with a growing rate of mothers dying from childbirth. The U.S. experiences 17.4 maternal deaths per 100,000 live births. In contrast, Norway is at 1.8 and the Netherlands at 3.0.
The risk of dying during delivery or in the post-partum period is dramatically higher for Black women in the United States. Even when controlling for economic factors, Black mothers still suffer twice as many deaths from childbirth as white women.
And with growing restrictions on a woman’s right to choose, the maternal mortality rate will likely continue to rise in the United States going forward.
Mental Health
Finally, the mental health of our country is in decline with rates of anxiety, depression and suicide on the rise.
These problems were bad prior to Covid-19, but years of isolation and social distancing only aggravated the problem. Suicide is now a leading cause of death for teenagers. Now, more than 1 in every 1,000 youths take their own lives each year. The newest data show that suicides across the U.S. have reached an all-time high and now exceed homicides.
Even with the expanded use of telemedicine, mental health in our nation is likely to become worse as Americans struggle to access and afford the services they require.
The Future
In looking at the three lists, I’m reminded of a baseball slugger who can occasionally hit awe-inspiring home runs but strikes out most of the time. The crowd may love the big hitter and celebrate the long ball, but in both baseball and healthcare, failing at the basics consistently results in more losses than wins.
Over the past five years, American medicine has produced a losing record. New drugs and surgical breakthroughs have made headlines, but the deeper, more systemic failures of American healthcare have rarely penetrated the news cycle.
If our nation wants to make the next five years better and healthier than the last five, elected officials and healthcare leaders will need to make major improvements. The steps required to do so will be the focus of my next article.
A new CDC study has found that the Covid-19 bivalent booster reduces the risk of symptomatic infection from the most common subvariant circulating in the U.S. right now by about half.
Additional new data, set to be published on the CDC website on Wednesday, also shows that individuals who received an updated vaccine reduced their risk of death by nearly 13 fold, when compared to the unvaccinated, and by two fold when compared to those with at least one monovalent vaccine but no updated booster.
CDC officials said during a briefing on Wednesday that the new findings were “reassuring.” But only 15.3 percent of eligible Americans — or about 50 million people — have received the new shot, which was rolled out in September.
Meanwhile, the highly transmissible Omicron subvariant XBB.1.5 — nicknamed “the Kraken” by some — is now the dominant SARS-CoV-2 strain in the U.S., projected by the CDC to make up just over 49 percent of cases in the country as of last week.
Earlier this month, the WHO said XBB.1.5 is the most transmissible variant to date, and is circulating in dozens of countries. Though a catastrophic wave has not emerged in the U.S. yet, there has nevertheless been a spike in deaths this month, with an average of 564 people dying of Covid-19 each day as of Jan. 18, compared with an average of 384 around the same time in December.
The new vaccine efficacy study, which used data from the national pharmacy program for Covid testing, found that the bivalent booster provided 48 percent greater protection against symptomatic infection from the XBB and XBB.1.5 subvariants among people who had the booster in the previous two to three months, compared with people who had only previously received two to four monovalent doses.
It also provided 52 percent greater protection against symptomatic infection from the BA.5 subvariant, though according to CDC estimates, BA.5 only accounted for about 2 percent of U.S. cases last week.
CDC officials cautioned that the findings reflected a population-level rate of protection, and that individual risk of infection varies.
“It’s hard to interpret it as an individual’s risk, because every individual is different,” said Ruth Link-Gelles, the author of the vaccine effectiveness study published in MMWR Wednesday. “Their immune system is different, their past history of prior infection is different. They may have underlying conditions that put them at more or less risk of COVID-19 disease.”
She also said it was unclear, given the limitations of the study, how long the bivalent booster protection will last.
“It’s too early to know how waning will happen with the bivalent vaccine,” she said. “What we’ve seen in the past is that your protection lasts longer for more severe illness. So even though you may have diminished protection over time against symptomatic infection, you’re likely still protected against more severe disease for a longer period of time.”
Hospitals across the country are being hit with a spike in respiratory syncytial virus (RSV) and influenza cases, while still dealing with a steady flow of COVID admissions, in what’s been dubbed a “tripledemic”. The graphic above uses hospitalization data from the Centers for Disease Control and Prevention (CDC) to show that each disease has been sending similar shares of the population to hospitals across late fall, with flu hospitalizations having just overtaken COVID admissions after Thanksgiving.
These numbers reflect that we’re experiencing the worst RSV season in at least five years, and we’re set to endure the worst flu season since 2009-10.As RSV is most severe in very young children, its recent surge has revealed another capacity shortage in our nation’s hospitals: pediatric beds. From 2008 to 2018, pediatric inpatient bed counts fell by 19 percent, as hospitals shifted resources to higher revenue services.
This strategy has now come to a head in many parts of the country, as RSV has driven pediatric bed usage rates to a recent high. (The Department of Health and Human Services’ pediatric capacity data only dates back to August 2020.) With three straight weeks of declining RSV hospitalizations, there is reason to hope that pediatric care units will soon feel a reprieve. However, flu season has yet to reach its peak, prompting calls for a return to widespread mask-wearing and a renewed emphasis on flu shots, given that more than half of Americans have not yet gotten vaccinated this season.
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.
A storm of these proportions should demand not only crisis clinical measures, but also community prevention efforts. Yet instead of deploying public health strategies to weather the storm, the U.S. is abandoning them.
Even before the arrival of the so-called tripledemic, U.S. health systems were on the brink. But as the fall surge of illness threatens to capsize teetering hospitals, the will to deploy public health measures has also collapsed. Pediatricians are declaring “This is our March 2020” and issuing pleas for help while public health efforts to flatten the curve and reduce transmission rates of Covid-19 — or any infectious disease — have effectively evaporated. Unmanageable patient volumes are seen as inevitable, or billed as the predictable outcome of an “immunity debt,” despite considerable uncertainty surrounding the scientific underpinnings and practical utility of this concept.
The Covid-19 pandemic should have left us better prepared for this moment. It helped the public to understand that respiratory viruses primarily spread through shared indoor air. Public health practices to stop the spread of Covid-19 — such as masking, moving activities outdoors, and limiting large gatherings during surges — were incorporated into the daily routines of many Americans. RSV and flu are also much less transmissible than Covid-19, making them easier to control with common-sense public health practices.
Instead of dialing up those first-line practices as pediatric ICUs overflow and classrooms close, though, the U.S. is relying on its precious and fragile last lines of defense to combat the tripledemic: health care professionals and medical facilities.
Warnings and advisories recently issued by U.S. public health leaders, clinical leaders, politicians, and the media have consistently neglected to mention masking as a powerful short-term public health strategy that can blunt the surge of viral illness. Instead, recent guidance has exclusively promoted handwashing and cough etiquette. These recommendations run counter to recent calls to build on improved understanding of the transmission of respiratory viruses.
In the U.S.’s efforts to “move on” from thinking about Covid, it has created a “new normal” that is deeply abnormal — one in which we normalize resorting to crisis measures, such as treating patients in tents, instead of using common-sense public health strategies. Treating Covid like the flu — or the flu like Covid — has effectively meant that we treat neither illness as if it were a serious threat to health systems and to public health. Mobilizing Department of Defense troops and Federal Emergency Management Agency personnel to cover health system shortfalls is apparently more palatable than asking people to wear masks.
The tripledemic has already claimed its first child deaths in the U.S., adding to a large ongoing death toll from Covid. Allowing health systems to reach the brink of collapse will lead to many more preventable deaths among pediatric and other vulnerable patients who can’t access the care they need.
By any accounting, these losses are shocking and tragic. But they should strike us as particularly abhorrent and shameful because the tripledemic is a crisis that leaders, health agencies, and institutions have, in a sense, chosen. Over the past year, the Biden administration and its allies have repeatedly encouraged the public to stand down on public health measures, with the President even stating in September that “the pandemic is over.” By moving real risks out of view and failing to push for more robust measures to mitigate Covid, these messages have put the country on a path to its present circumstances, in which pediatric RSV patients are transferred to hospitals hundreds of miles away because there is no capacity to treat them in their own communities.
Living with viruses should mean embracing simple public health measures rather than learning to live with staggering levels of illness and death. Leaders in public health and medicine should issue timely and appropriate guidance that reflects the latest science instead of second-guessing the prevailing winds in public opinion. Instead of self-censoring their recommendations out of fear of political consequences, they should continue to promote the full range of public health strategies, including masking in crowded indoor public places during surges.
The tripledemic should bring renewed urgency to policies that will reduce the toll of seasonal illness on health, education, and the economy. Improvements in indoor air quality in public spaces, including schools, child care centers, and workplaces, can limit the spread of diseases and have many demonstrated health and economic benefits, yet the U.S. continues to lack standards to guide infrastructure or workplace safety standards. Paid leave enabling workers to stay home when they are ill can reduce the transmission of disease as well as loss of income, yet the U.S. is one of the only high-income countries without universal paid sick leave or family medical leave.
Greater effort must also be made to increase vaccination coverage for flu and Covid and bring an RSV vaccine online as quickly as possible. Only about half of high-risk adults under 65 received a flu shot last year, a gap that can be closed with more energetic vaccination campaigns. Reducing annual flu deaths using a broader range of strategies enabled by the pandemic — rather than pegging Covid deaths to them — should be the goal.
Amid the many sobering stories of the tripledemic, there is some good news. As the experience of Covid-19 has shown, it is possible to limit the toll of respiratory viruses like flu and RSV. However, this work requires resources, appropriate policies, and political will. Americans don’t need to accept winter disease surges and overrun health systems as an inevitable new normal. Instead, the country should see the tripledemic as a call to reinvigorate public health strategies in response to these threats to the health of our communities.
A new COVID calamity is hammering China, with a surge in infections prompting a return of lockdowns, including in some manufacturing areas that supply the West.
China reported a record number of infections this week, amid lockdowns and mass testing that are fueling unrest and darkening the country’s economic outlook. Schools in Beijing returned to online teaching.
Why it matters: In addition to the human misery for the world’s most populous country, the effects will be felt around the globe, Axios China author Bethany Allen-Ebrahimian reports from Taipei.
Supply chains are likely to be disrupted, causing prices to rise in an already rocky global economy.
Rare protests broke out today in China’s far western Xinjiang region. Crowds shouted at hazmat-suited guards after a deadly fire triggered anger by prolonged COVID lockdowns, Reuters reports.
“End the lockdown!” shouted protesters in the Xinjiang capital Urumqi, where an apartment fire killed 10.
What’s happening: The moment of truth for China’s zero-COVID policy has finally come.
Either party leaders will need to plunge much of the country into draconian lockdowns, as we saw at the beginning of the pandemic — or they’ll decide it’s time to learn to live with COVID.
Reality check: China’s doctors have warned Xi Jinping that the healthcare system isn’t prepared for the huge outbreak likely to follow the easing of strict anti-COVID measures, the Financial Times reports.
Chinese-made vaccines, which don’t use the mRNA technology employed by many produced by the West, aren’t as effective compared to those made in the U.S. And China has worrisomely low vaccination rates among older people.
But the number of cases in China is actually still very low for anywhere but China.
The big picture: “Zero COVID” restrictions have damaged the economy and undermined people’s trust in government.
That’s a stark about-face from the height of the pandemic. Then, many Chinese people felt the tight central control had protected them better than any other governance model in the world.
But it’s that very model that has plunged China into its current predicament. Xi tied his reputation, and the party’s legitimacy, to the success of “zero COVID.”
Between the lines: Chinese leaders made a huge, politically motivated mistake. They resisted the import of Western-made mRNA vaccines (including Pfizer and Moderna) for its citizens. These vaccines were only recently made available to foreigners.
That’s likely because of Beijing’s big vaccine diplomacy push: Chinese officials touted their own vaccines as the best and safest.
It was politically unpalatable to admit “defeat,” and allow Chinese people to get more effective — but Western-made — jabs.
China is facing an increasingly precarious situation as new COVID cases soar and the population seems to be hitting a breaking point with the government’s stringent zero-tolerance policies.
Why it matters: The world’s most populous nation has massive vulnerabilities heading into this winter, starting with the fact the vast majority of its population has yet to be exposed to the virus and has little ‘natural immunity.’
China’s vaccines didn’t work well compared to those distributed in the West, and the government refused to approve foreign vaccines and doesn’t have a version to combat Omicron.
Vaccine uptake was particularly low among the elderly.
And now, public outrage over new COVID lockdown restrictions has fueled rare protests, Axios’ Herb Scribner writes, with residents demanding the government to lift restrictions quickly and some calling for President Xi Jinping’s resignation.
State of play: Overall, China’s number of reported COVID cases and COVID deaths are far lower than other nations, but there have been recent reported spikes in overall numbers of cases and some new deaths.
It came after the Chinese government announced some easing of its zero-COVID policy, such as reducing mass testing and quarantine requirements, earlier this month.
Reality check: China’s doctors have warned that the health care system isn’t prepared for the huge outbreak likely to follow any easing of public health measures, Axios’ Bethany Allen-Ebrahimian writes.
That includes worries the nation doesn’t have enough ICU bed capacity to handle such outbreaks, according to the Financial Times.
Between the lines: Another concern is the potential evolution of a new, more dangerous variant if there’s a huge surge of infections, Christian Drosten, Germany’s most prominent virologist, told Bloomberg.
“Xi Jinping knows very well that he can’t simply let the virus loose,” Drosten said. “The Chinese population first needs to be as well vaccinated as we are.”
Be smart: China’s officials are scrambling to address the vaccine problem.
For instance, they are launching more aggressive vaccine drives and limiting movement among at-risk groups, including the elderly, the Washington Post reports.
But they have yet to open up the availability of mRNA vaccines from Pfizer-BioNTech and Moderna, opting to focus on their own, per the Post.
The bottom line: China’s zero-COVID policy has kept cases in China relatively low compared to the rest of the world.
But even as the societal and economic consequences of shutdowns become apparent, it faces a very difficult path ahead in unwinding strict public health policies.
Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
Can bivalent boosters prevent another surge of infections?
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
How much additional protection do updated shots provide?
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Will we see an increase in vaccine uptake?
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”