The Centers for Disease Control and Prevention reported on Monday that 2.1 million doses of coronavirus vaccines have been administered in two weeks. While this might sound like an impressive number, it should set off alarms.
Let’s start with the math. Anthony S. Fauci, the government’s top infectious-disease doctor, estimates that 80 to 85 percent of Americans need to be vaccinated to reach herd immunity. Both the Pfizer and Moderna vaccines require two doses. Eighty percent of the American population is around 264 million people, so we need to administer 528 million doses to achieve herd immunity.
At the current rate, it would take the United States approximately 10 years to reach that level of inoculation. That’s right — 10 years. Contrast that with the Trump administration’s rosy projections: Earlier this month, Health and Human Services Secretary Alex Azar predicted that every American will be able to get the vaccine by the second quarter of 2021 (which would be the end of June). The speed needed to do that is 3.5 million vaccinations a day.
There’s reason to believe the administration won’t be able to ramp up vaccination rates anywhere close to those levels. Yes, as vaccine production increases, more will be available to the states. And Brett Giroir, assistant secretary for health at HHS, argued on Sunday that the 2.1 million administered vaccines figure was an underestimate due to delayed reporting. So let’s be generous and say the administration actually administered 4 million doses over the first two weeks.
But even that would still fall far short of the 3.5 million vaccinations needed per day. In fact, it falls far short of what the administration had promised to accomplish by the end of 2020 — enough doses for 20 million people. And remember, the first group of vaccinations was supposed to be the easiest: It’s hospitals and nursing homes inoculating their own workers and residents. If we can’t get this right, it doesn’t bode well for the rest of the country.
Here’s what concerns me most: Instead of identifying barriers to meeting the goal, officials are backtracking on their promises. When states learned they would receive fewer doses than they had been told, the administration said its end-of-year goal was not for vaccinations but vaccine distribution. It also halved the number of doses that would be available to people, from 40 million to 20 million. (Perhaps they hoped no one would notice that their initial pledge was to vaccinate 20 million people, which is 40 million doses, or that President Trump had at one point vowed to have 100 million doses by the end of the year.) And there’s more fancy wordplay that’s cause for concern: Instead of vaccine distribution, the administration promises “allocation” in December. Actual delivery for millions of doses wouldn’t take place until January, to say nothing of the logistics of vaccine administration.
The vaccine rollout is giving me flashbacks to the administration’s testing debacle. Think back to all the times Trump pledged that “everyone who wants a test can get one.” Every time this was fact-checked, it came up false. Instead of admitting that there wasn’t enough testing, administration officials followed a playbook to confuse and obfuscate: They first attempted to play up the number of tests done. Just like 2 million vaccines in two weeks, 1 million tests a week looked good on paper — until they were compared to the 30 million a day that some experts say are needed. The administration then tried to justify why more tests weren’t needed. Remember Trump saying that “tests create cases” or the CDC issuing nonsensical testing guidance?
When that didn’t work, Trump officials deflected blame to the states. Never mind that there should have been a national strategy or that states didn’t have the resources to ramp up testing on their own. It was easier to find excuses than to admit that they were falling short and do the hard work to remedy it.
Instead of muddying the waters, the federal government needs to take three urgent steps. First, set up a real-time public dashboard to track vaccine distribution. The public needs to know exactly how many doses are being delivered, distributed and administered. Transparency will help hold the right officials accountable, as well as target additional resources where they are most needed.
Second, publicize the plan for how vaccination will scale up so dramatically. States have submitted their individual plans to the CDC, but we need to see a national strategy that sets ambitious but realistic goals.
Third, acknowledge the challenges and end the defensiveness. The public will understand if initial goals need to be revised, but there must be willingness to learn from missteps and immediately course-correct.
I remain optimistic that vaccines will one day end this horrific pandemic that has taken far too many lives. To get there, we must approach the next several months with urgency, transparency and humility.
Colorado officials on Tuesday reported the first known case in the United States of a person infected with the coronavirus variant that has been circulating rapidly across much of the United Kingdom and has led to a lockdown of much of southern England.
Scientists have said the variant is more transmissible but does not make people sicker.
The Colorado case involves a man in his 20s, who is in isolation in Elbert County, about 50 miles southeast of Denver, and has no travel history, according to a tweet from the office of Gov. Jared Polis (D).
“The individual has no close contacts identified so far but public health officials are working to identify other potential cases and contacts through thorough contact tracing interviews,” the statement said.
A federal scientist familiar with the investigation said the man’s lack of known travel — in contrast with most confirmed cases outside the United Kingdom — indicates this is probably not an isolated case. “We can expect that it will be detected elsewhere,” said the official, who spoke on the condition of anonymity to discuss the broader context of the announcement.
The Centers for Disease Control and Prevention confirmed as much in a statement Tuesday afternoon, saying additional cases with the new variant will be detected in the United States in coming days. The variant’s apparent increase in contagiousness “could lead to more cases and place greater demand on already strained health care resources,” the agency said in a statement.
Researchers have detected the more transmissible variant in at least 17 countries outside the United Kingdom, including as far away as Australia and South Korea, as of Tuesday afternoon. Officials in Canada had previously said they had identified two cases.
Although the U.K. variant appears more contagious, it is not leading to higher rates of hospitalizations or deaths, according to a report from Public Health England, a government agency. Nor is there any sign that people who were infected months ago with the coronavirus are more likely to be reinfected if exposed to the variant, according to the report. All available evidence indicates that vaccines, and immunity built up in the population, should be protective against this variant.
The Colorado case occurred in a county of about 27,000, which is currently classified, along with much of the state, in the “red” level for the virus, denoting serious but not extreme risk.
Two weeks ago, several hundred people gathered at a community church in the county seat of Kiowa to consider whether to pursue legal actions against Polis and other state officials for imposing coronavirus-related restrictions, according to the Elbert County News. County commissioners and the county sheriff have declined to enforce restrictions emanating from Denver.
“I was expecting to see it in ski country first because those areas are where people from across Colorado, the U.S. and internationally, gather,” said Elizabeth Carlton, an assistant professor of environmental and occupational health at the Colorado School of Public Health. The absence of any apparent travel history associated with the infected person, she said, suggests he “can’t be the only case in Colorado.”
Polis, in his statement, called on Coloradans to do everything they could to prevent transmission by wearing masks, standing six feet apart when gathering with others, and interacting only with members of their immediate households.
The arrival of the new variant “doesn’t fundamentally change the nature of the threat,” said Justin Lessler, an epidemiologist at Johns Hopkins Bloomberg School of Public Health. “It’s no more deadly than the virus was before, and it doesn’t look like it infects people who are immune.”
Lessler echoed others, saying he would be “astounded” if this was the only chain of transmission of the new variant in the United States. “We know that the virus spreads easily and quickly between countries,” he said, and the fact that the infected person had no travel history indicates “this strain has gotten here sometime in the past, and there are chains of transmission ongoing.”
The variant has a higher attack rate, according to the U.K. report, which bolsters the hypothesis that the variant has out-competed other versions of the coronavirus and is now the dominant variant across much of the United Kingdom. Among people known to have been exposed to someone already infected with the variant, 15.1 percent became infected. People exposed to someone infected with the non-variant version had a 9.8 percent infection rate.
That difference suggests the variant is more transmissible, though Public Health England said more investigation is needed to bolster the hypothesis.
The working theory among many scientists is that the increased transmissibility of the variant, known as B.1.1.7, is driven by mutations that have altered the spike protein on the surface of the virus. The variant has 17 mutations — eight of which alter the spike protein.
Precisely how those changes are leading to more infections is unknown. The virus may be binding more easily to receptor cells in the human body, or replicating more easily and driving higher viral loads, enhancing viral shedding by someone who is infected. Another possibility is that people are shedding the virus for a longer period, increasing the chances of passing it along.
“Preliminary evidence suggests that the new variant does not cause more severe disease or increased mortality,” Susan Hopkins, a senior medical adviser to Public Health England, said in a statement released Tuesday.
The newly published data echo the findings in a separate study published last week, based on modeling and hospitalization data — and not yet peer-reviewed — that estimated that the variant is 56 percent more transmissible but does not appear to alter the lethality of the virus.
“The good news is that B.1.1.7 does not seem to cause much more severe disease, and there’s no evidence that it is managing to evade the immune system, which means vaccines are expected to protect against it,” William Hanage, an epidemiologists at the Harvard T.H. Chan School of Public Health, said Tuesday after reviewing the new report. “The bad news is that B.1.1.7 does appear to be much more transmissible.”
Officials in the United States have been signaling since last week that the new variant was probably already present in this country.
“I’m not surprised,” Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said Tuesday. “I think we have to keep an eye on it, and we have to take it seriously. We obviously take any kind of mutation that might have a functional significance seriously. But I don’t think we know enough about it to make any definitive statements, except to follow it carefully and study it carefully.”
Research findings on coronavirus variants have been ambiguous at times, and scientists say they are still trying to extract reliable signals from noisy data. There have been several false alarms sounded about virus mutations in the past. A major challenge is discerning whether a virus variant is spreading rapidly because it has a competitive advantage based on genetic and structural differences, or because it is simply lucky, having arrived early to a location or leveraged a few superspreader events to gain dominance.
But with the United Kingdom seeing a severe winter surge of infections, public officials are taking no chances and have effectively locked down southern England, including London. Other countries have banned travelers from the United Kingdom.
The United States, despite having the world’s highest number of documented infections, has a weak track record in publishing genomic sequences, the process that enables researchers to track changes in the virus. Most sequences have been published by academic or private research institutions. By comparison, the United Kingdom has a national health system with a robust surveillance system.
“The U.K. made the decision in the spring to do this. The U.S. has sequencing equipment and infrastructure. As with many things in this pandemic, it was not executed the way it should have been,” said Neville Sanjana, a geneticist at New York University.
All viruses mutate randomly, and over time some of those mutations appear to confer some kind of advantage to the virus as it adapts to the human species. The novel coronavirus, SARS-CoV-2, mutates at a slow rate, and scientists do not think the genetic changes seen in the variant so far are sufficient to allow it to elude the vaccines now being administered to millions of people in many countries. But the coronavirus is a moving target and these mutations require surveillance.
Many scientists call the arrival of more transmissible mutations a wake-up call. “The lack of virus sequencing and case tracking in the USA is a scandal,” said Jeremy Luban, a virologist at the University of Massachusetts Medical School.
Francois Balloux, who directs the Genetics Institute at University College London, on Twitter predicted that within two weeks, enough data will accumulate to determine whether this new variant is indeed more transmissible. Previously, Balloux and his colleagues combed through genome sequences, looking for evidence that common variants had increased transmissibility.
“We don’t see much,” he said, referring to a report published in the journal Nature in November that found no signs of mutations that helped the virus to spread more easily. However, he said he “wouldn’t underestimate the evolutionary potential of SARS-CoV-2.”
President-elect Joe Biden plans to deliver an address on the coronavirus pandemic as the nation experiences what his chief medical adviser on the issue, Anthony S. Fauci, described Tuesday as a surge in cases “that has just gotten out of control in many respects.”
Biden’s remarks, planned Tuesday afternoon in Wilmington, Del., are expected to be his most extensive comments to date since early this month, when he laid out a plan for his first 100 days in office that included imploring all Americans to wear masks.
Fauci, appearing on CNN on Tuesday morning, lamented what he expects to be a post-holiday increase in cases and the strong possibility than January’s caseload will exceed even that of December. “You just have to assume it’s going to get worse,” Fauci said.
Fauci also acknowledged that the rollout of vaccines was not reaching as many Americans as quickly as the 20 million that Trump administration had pledged by the end of the month.
“We certainly are not at the numbers that we wanted to be at the end of December,” said Fauci, director of the National Institute of Allergy and Infectious Diseases. “We are below where we want to be.”
But Fauci, who accepted Biden’s invitation to play an expanded role in his administration, expressed hope that by “showing leadership from the top,” Biden could make an impact — comments that appeared to be implicit criticism of President Trump, who has said little publicly about the crisis since Election Day.
“What he’s saying is that let’s take at least 100 days and everybody, every single person put aside this nonsense of making masks be a political statement or not,” Fauci said of Biden. “We know what works. We know social distancing works. We know avoiding congregant settings works. For goodness sakes, let’s all do it, and you will see that curve will come down.”
Separately Tuesday, Vice President-elect Kamala D. Harris plans to get vaccinated in Washington. Biden received his first shot last week.
In remarks earlier this month, Biden also pledged to distribute 100 million vaccine shots in his first 100 days in office and said he wanted to open as many schools safely during the period as possible. He has also promised to sign an executive order requiring masks to be worn on federal property.
On Monday, Celine Gounder, a member of Biden’s covid-19 advisory board, said during a television appearance that Biden is also considering invoking the Defense Production Act to increase production of coronavirus vaccines,
Appearing on CNBC’s “Squawk Box,” Grounder said Biden could invoke the wartime-production law “to make sure the personal protective equipment, the test capacity and the raw materials for the vaccines are produced in adequate supply.”
During his CNN appearance, Fauci said that getting children back to school safely should remain an imperative, despite rising caseloads.
“You can’t have one size fits all, but the bottom line, what I call default position, should be that wherever we are, try as best as we can to get the children back to school and to keep them in school and to have a plan to try and keep them as safe as possible,” he said.
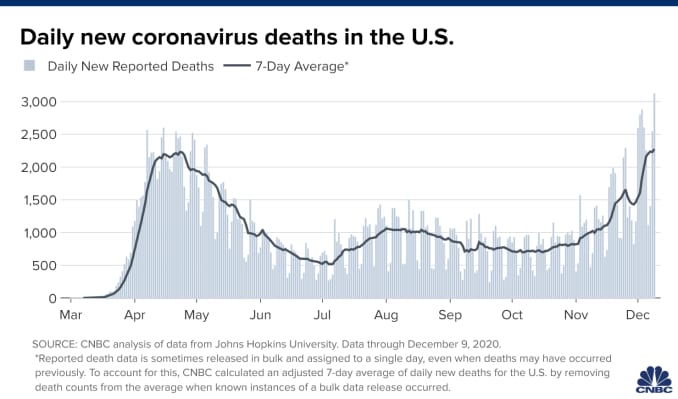
About 200,000 new coronavirus cases have been reported daily in recent weeks, with a record high of 252,431 on Dec. 17.
The nation’s overall caseload surpassed 19 million Sunday, even as the holidays were expected to cause a lag in reporting. Hospitalizations have exceeded 100,000 since the start of December and hit a peak of 119,000 on Dec. 23. Deaths are averaging more than 2,000 a day, with the most ever reported — 3,406 fatalities — on Dec. 17.
After officials in the United Kingdom said Saturday that the variant first identified there was spreading 70 percent faster than others, Google searches about the mutation have spiked. But American public health experts and federal officials say that although it appears that the variant may be more contagious, it is not any more dangerous than others already detected in the United States.
“I don’t think there should be any reason for alarm right now,” Adm. Brett Giroir, who has been in charge of testing, told George Stephanopoulos on ABC’s “This Week.”
Variations to the virus are nothing new, and experts say the novel coronavirus does not mutate as much as influenza, meaning it is less likely that a vaccine would need to be developed every year to keep up with the new strains.
Still, much about this variant remains unknown, such as whether it is a new strain — a functionally different version of the virus.
“The take-home message for right now is that we need to get more information,” said Krutika Kuppalli, an infectious-diseases specialist at the Medical University of South Carolina. “In the meantime, we all need to really double down on our public health measures — wearing masks, remaining physically distanced, avoiding crowds of people.”
Where has the variant been detected?
In September, U.K. researchers discovered the variant’s prevalence when they collected samples from infected people in southeastern England. It seemed to spread quickly.
“This lineage came up quite rapidly,” Nick Loman, one of the researchers and a professor of microbial genomics at the University of Birmingham, told The Washington Post.
Since then, Australia, Denmark and the Netherlands have identified cases of the variant in their countries, the World Health Organization told the BBC. On Sunday, Italian officials announced that a patient returning from Britain “in the last few days” was in isolation after scientists detected the mutation.
In South Africa, health officials said Sunday that a version of the virus similar to the U.K. variant has been found in 80 to 90 percent of samples analyzed since mid-November.
Is the variant already in the United States?
The virus has not been detected in the United States, but officials are watching for developments in Britain, Giroir told Stephanopoulos.
Although guidance from federal agencies discourages traveling to Britain, the United States has not banned travel from there.
“I really don’t believe we need to do that yet,” Giroir said.
But New York Gov. Andrew M. Cuomo (D) pointed out Sunday that it would take only one flight to the United States to spread the mutation, urging federal officials to restrict travel.
“Right now, this variant in the U.K. is getting on a plane and flying to JFK,” Cuomo said on a conference call with reporters.
However, Kuppalli warned that little is known about the effectiveness of a ban, referring to instances in which people rushed to airports and congregated in long lines trying to travel before restrictions were put into effect earlier in the pandemic.
It is also not entirely certain whether the virus gained its foothold in the southeast of England because of its altered genetic markers or through super-spreading events, said Scott Gottlieb, a former head of the Food and Drug Administration.
“It seems like this new strain is more contagious,” Gottlieb said on CBS’s “Face the Nation.” “It doesn’t seem to be any more virulent, any more dangerous than run-of-the-mill covid. The next question is: Will it obviate our natural immunity?”
Will the authorized vaccines still be effective against this variant of the virus?
As of now, experts say there has been no indication that the variant is resistant to the Pfizer and Moderna vaccines authorized by the FDA.
“There is no reason to believe that the vaccines that have been developed will not be effective against this virus as well,” Vivek H. Murthy, President-elect Joe Biden’s nominee for surgeon general, told host Chuck Todd on NBC’s “Meet the Press.” “The bottom line is if you’re at home and hearing this news, it does not change what we do in terms of precautions.”
Although the vaccine remains out of reach for most Americans, following guidance such as social distancing and wearing masks remains the most practical way to prevent transmission.
Congressional leaders have reached an agreement on a $900 billion COVID-19 relief package and $1.4 trillion government funding deal with several healthcare provisions, according to Senate Majority Leader Mitch McConnell, R-Ky., and Minority Leader Chuck Schumer, D-N.Y.
Here are seven things to know about the relief aid and funding deal:
1. Congressional leaders have yet to release text of the COVID-19 legislation, but have shared a few key details on the measure, according to CNBC.Becker’s breaks down the information that has been released thus far.
2. The COVID-19 package includes $20 billion for the purchase of vaccines, about $9 billion for vaccine distribution and about $22 billion to help states with testing, tracing and other COVID-19 mitigation programs, according to Politico.
3. Lawmakers are also expected to include a provision changing how providers can use their relief grants. In particular, the bill is expected to allow hospitals to calculate lost revenue by comparing budgeted revenue for 2020. Hospitals have said this tweak will allow them to keep more funding.
4. The agreement also allocates $284 billion for a new round of Paycheck Protection Program loans.
5. The COVID-19 relief bill also provides$600 stimulus checks to Americans earning up to $75,000 per year and $600 for their children, according to NBC. It also provides a supplemental $300 per week in unemployment benefits.
6. The year-end spending bill includes a measure to ban surprise billing. Under the measure, hospitals and physicians would be banned from charging patients out-of-network costs their insurers would not cover. Instead, patients would only be required to pay their in-network cost-sharing amount when they see an out-of-network provider, according to The Hill.The agreement gives insurers 30 days to negotiate a payment on the outstanding bill. After that period, they can enter into arbitration to gain higher reimbursement.
7. Lawmakers plan to pass the relief bill and federal spending bill Dec. 21.
A Florida taxi driver and his wife had seen enough conspiracy theories online to believe the virus was overblown, maybe even a hoax. So no masks for them. Then they got sick. She died. A college lecturer had trouble refilling her lupus drug after the president promoted it as a treatment for the new disease. A hospital nurse broke down when an ICU patient insisted his illness was nothing worse than the flu, oblivious to the silence in beds next door.
Lies infected America in 2020. The very worst were not just damaging, but deadly.
President Donald J. Trump fueled confusion and conspiracies from the earliest days of the coronavirus pandemic. He embraced theories that COVID-19 accounted for only a small fraction of the thousands upon thousands of deaths. He undermined public health guidance for wearing masks and cast Dr. Anthony Fauci as an unreliable flip-flopper.
But the infodemic was not the work of a single person.
Anonymous bad actors offered up junk science. Online skeptics made bogus accusations that hospitals padded their coronavirus case numbers to generate bonus payments. Influential TV and radio opinion hosts told millions of viewers that social distancing was a joke and that states had all of the personal protective equipment they needed (when they didn’t).
It was a symphony of counter narrative, and Trump was the conductor, if not the composer. The message: The threat to your health was overhyped to hurt the political fortunes of the president.
Every year, PolitiFact editors review the year’s most inaccurate statements to elevate one as the Lie of the Year. The “award” goes to a statement, or a collection of claims, that prove to be of substantive consequence in undermining reality.
It has become harder and harder to choose when cynical pundits and politicians don’t pay much of a price for saying things that aren’t true. For the past month, unproven claims of massive election fraud have tested democratic institutions and certainly qualify as historic and dangerously bald-faced. Fortunately, the constitutional foundations that undergird American democracy are holding.
Meanwhile, the coronavirus has killed more than 300,000 in the United States, a crisis exacerbated by the reckless spread of falsehoods.
PolitiFact’s 2020 Lie of the Year: claims that deny, downplay or disinform about COVID-19.
‘I always wanted to play it down’
On Feb. 7, Trump leveled with book author Bob Woodward about the dangers of the new virus that was spreading across the world, originating in central China. He told the legendary reporter that the virus was airborne, tricky and “more deadly than even your strenuous flus.”
Trump told the public something else. OnFeb. 26, the president appeared with his coronavirus task force in the crowded White House briefing room. A reporter asked if he was telling healthy Americans not to change their behavior.
“Wash your hands, stay clean. You don’t have to necessarily grab every handrail unless you have to,” he said, the room chuckling. “I mean, view this the same as the flu.”
Three weeks later, March 19, he acknowledged to Woodward: “To be honest with you, I wanted to always play it down. I still like playing it down. Because I don’t want to create a panic.”
His acolytes in politics and the media were on the same page. Rush Limbaugh told his audience of about 15 million on Feb. 24 that coronavirus was being weaponized against Trump when it was just “the common cold, folks.” That’s wrong — even in the early weeks, it was clear the virus had a higher fatality rate than the common cold, with worse potential side effects, too.
As the virus was spreading, so was the message to downplay it.
“There are lots of sources of misinformation, and there are lots of elected officials besides Trump that have not taken the virus seriously or promoted misinformation,” said Brendan Nyhan, a government professor at Dartmouth College. “It’s not solely a Trump story — and it’s important to not take everyone else’s role out of the narrative.”
The skeptics cited Centers for Disease Control and Prevention data to claim that only 6% of COVID-19 deaths could actually be attributed to the virus. On Aug. 24, BlazeTV host Steve Deace amplified it on Facebook.
“Here’s the percentage of people who died OF or FROM Covid with no underlying comorbidity,” he said to his 120,000 followers. “According to CDC, that is just 6% of the deaths WITH Covid so far.”
That misrepresented the reality of coronavirus deaths. The CDC had always said people with underlying health problems — comorbidities — were most vulnerable if they caught COVID-19. The report was noting that 6% died even without being at obvious risk.
But for those skeptical of COVID-19, the narrative confirmed their beliefs. Facebook users copied and pasted language from influencers like Amiri King, who had 2.2 million Facebook followers before he was banned. The Gateway Pundit called it a “SHOCK REPORT.”
“I saw a statistic come out the other day, talking about only 6% of the people actually died from COVID, which is very interesting — that they died from other reasons,” Trump told Fox News host Laura Ingraham on Sept. 1.
Fauci, director of the National Institute of Allergy and Infectious Diseases, addressed the claim on “Good Morning America” the same day.
“The point that the CDC was trying to make was that a certain percentage of them had nothing else but just COVID,” he said. “That does not mean that someone who has hypertension or diabetes who dies of COVID didn’t die of COVID-19 — they did.”
Trump retweeted the message from an account that sported the slogans and symbols of QAnon, a conspiracy movement that claims Democrats and Hollywood elites are members of an underground pedophilia ring.
False information moved between social media, Trump and TV, creating its own feedback loop.
“It’s an echo effect of sorts, where Donald Trump is certainly looking for information that resonates with his audiences and that supports his political objectives. And his audiences are looking to be amplified, so they’re incentivized to get him their information,” said Kate Starbird, an associate professor and misinformation expert at the University of Washington.Weakening the armor: misleading on masks
At the start of the pandemic, the CDC told healthy people not to wear masks, saying they were needed for health care providers on the frontlines. But on April 3 the agency changed its guidelines, saying every American should wear non-medical cloth masks in public.
Trump announced the CDC’s guidance, then gutted it.
“So it’s voluntary. You don’t have to do it. They suggested for a period of time, but this is voluntary,” Trump said at a press briefing. “I don’t think I’m going to be doing it.”
Rather than an advance in best practices on coronavirus prevention, face masks turned into a dividing line between Trump’s political calculations and his decision-making as president. Americans didn’t see Trump wearing a mask until a July visit to Walter Reed National Military Medical Center.
In September, the CDC reported a correlation between people who went to bars and restaurants, where masks can’t consistently be worn, and positive COVID-19 test results. Bloggers and skeptical news outlets countered with a misleading report about masks.
On Oct. 13, the story landed on Fox News’ flagship show, “Tucker Carlson Tonight.” During the show, Carlson claimed “almost everyone — 85% — who got the coronavirus in July was wearing a mask.”
“So clearly (wearing a mask) doesn’t work the way they tell us it works,” Carlson said.
That’s wrong, and it misrepresented a small sample of people who tested positive. Public health officials and infectious disease experts have been consistent since April in saying that face masks are among the best ways to prevent the spread of COVID-19.
But two days later, Trump repeated the 85% stat during a rally and at a town hall with NBC’s Savannah Guthrie.
“I tell people, wear masks,” he said at the town hall. “But just the other day, they came out with a statement that 85% of the people that wear masks catch it.”
The assault on hospitals
On March 24, registered nurse Melissa Steiner worked her first shift in the new COVID-19 ICU of her southeast Michigan hospital. After her 13-hour day caring for two critically ill patients on ventilators, she posted a tearful video.
“Honestly, guys, it felt like I was working in a war zone,” Steiner said. “(I was) completely isolated from my team members, limited resources, limited supplies, limited responses from physicians because they’re just as overwhelmed.”
“I’m already breaking, so for f—’s sake, people, please take this seriously. This is so bad.”
Steiner’s post was one of manyemotionalpleas offered by overwhelmed hospital workers last spring urging people to take the threat seriously. The denialists mounted a counter offensive.
On March 28, Todd Starnes, a conservative radio host and commentator, tweeted a video from outside Brooklyn Hospital Center. There were few people or cars in sight.
“This is the ‘war zone’ outside the hospital in my Brooklyn neighborhood,” Starnes said sarcastically. The video racked up more than 1.5 million views.
Starnes’ video was one of the first examples of #FilmYourHospital, a conspiratorial social media trend that pushed back on the idea that hospitals had been strained by a rapid influx of coronavirus patients.
Several internet personalities asked people to go out and shoot their own videos. The result: a series of user-generated clips taken outside hospitals, where the response to the pandemic was not easily seen. Over the course of a week, #FilmYourHospital videos were uploaded to YouTube and posted tens of thousands of times on Twitter and Facebook.
Nearly two weeks and more than 10,000 deaths later, Fox News featured a guest who opened a new misinformation assault on hospitals.
Dr. Scott Jensen, a Minnesota physician and Republican state senator, told Ingraham that, because hospitals were receiving more money for COVID-19 patients on Medicare — a result of a coronavirus stimulus bill — they were overcounting COVID-19 cases. He had no proof of fraud, but the cynical story took off.
Trump used the false report on the campaign trail to continue to minimize the death toll.
“Our doctors get more money if somebody dies from COVID,” Trump told supporters at a rally in Waterford, Mich., Oct. 30. “You know that, right? I mean, our doctors are very smart people. So what they do is they say, ‘I’m sorry, but, you know, everybody dies of COVID.’”
The real fake news: The Plandemic
The most viral disinformation of the pandemic was styled to look like it had the blessing of people Americans trust: scientists and doctors.
In a 26-minute video called “Plandemic: The Hidden Agenda Behind COVID-19,” a former scientist at the National Cancer Institute claimed that the virus was manipulated in a lab, hydroxychloroquine is effective against coronaviruses, and face masks make people sick.
Judy Mikovits’ conspiracies received more than 8 million views in May thanks in part to the online outrage machine — anti-vaccine activists, anti-lockdown groups and QAnon supporters — that push disinformation into the mainstream. The video was circulated in a coordinated effort to promote Mikovits’ book release.
A couple of months later, a similar effort propelled another video of fact-averse doctors to millions of people in only a few hours.
On July 27, Breitbart publisheda clipof a press conference hosted by a group called America’s Frontline Doctors in front of the U.S. Supreme Court. Looking authoritative in white lab coats, these doctors discouraged mask wearing and falsely said there was already a cure in hydroxychloroquine, a drug used to treat rheumatoid arthritis and lupus.
Trump, who had been talking up the drug since March and claimed to be taking it himself as a preventive measure in May, retweeted clips of the event before Twitter removed them as misinformation about COVID-19. He defended the “very respected doctors” in a July 28 press conference.
When Olga Lucia Torres, a lecturer at Columbia University, heard Trump touting the drug in March, she knew it didn’t bode well for her own prescription. Sure enough, the misinformation led to a run on hydroxychloroquine, creating a shortage for Americans like her who needed the drug for chronic conditions.
A lupus patient, she went to her local pharmacy to request a 90-day supply of the medication. But she was told they were only granting partial refills. It took her three weeks to get her medication through the mail.
“What about all the people who were silenced and just lost access to their staple medication because people ran to their doctors and begged to take it?” Torres said.No sickbed conversion
On Sept. 26, Trump hosted a Rose Garden ceremony to announce his nominee to replace the late Ruth Bader Ginsburg on the U.S. Supreme Court. More than 150 people attended the event introducing Amy Coney Barrett. Few wore masks, and the chairs weren’t spaced out.
In the weeks after, more than two dozen people close to Trump and the White House became infected with COVID-19. Early Oct. 2, Trump announced his positive test.
Those hoping the experience and Trump’s successful treatment at Walter Reed might inform his view of the coronavirus were disappointed.
Trump snapped back into minimizing the threat during his first moments back at the White House. He yanked off his mask and recorded a video.
“Don’t let it dominate you. Don’t be afraid of it,” he said, describing experimental and out-of-reach therapies he received. “You’re going to beat it.”
In Trump’s telling, his hospitalization was not the product of poor judgment about large gatherings like the Rose Garden event, but the consequence of leading with bravery. Plus, now, he claimed, he was immune from the virus.
On the morning after he returned from Walter Reed, Trump tweeted a seasonal flu death count of 100,000 lives and added that COVID-19 was “far less lethal” for most populations. More false claims at odds with data — the U.S. average for flu deaths over the past decade is 36,000, and experts said COVID-19 is more deadly for each age group over 30.
When Trump left the hospital, the U.S. death toll from COVID-19 was more than 200,000. Today it is more than 300,000. Meanwhile, this month the president has gone ahead with a series of indoor holiday parties.
The vaccine war
The vaccine disinformation campaign started in the spring but is still underway.
In April, blogs and social media users falsely claimed Democrats and powerful figures like Bill Gates wanted to use microchips to track which Americans had been vaccinated for the coronavirus. Now, false claims are taking aim at vaccines developed by Pfizer and BioNTech and other companies.
A blogger claimed Pfizer’s head of research said the coronavirus vaccine could cause female infertility. That’s false.
An alternative health website wrote that the vaccine could cause an array of life-threatening side effects, and that the FDA knew about it. The list included all possible — not confirmed— side effects.
Social media users speculated that the federal government would force Americans to receive the vaccine. Neither Trump nor President-elect Joe Biden has advocated for that, and the federal government doesn’t have the power to mandate vaccines, anyway.
As is often the case with disinformation, the strategy is to deliver it with a charade of certainty.
“People are anxious and scared right now,” said Dr. Seema Yasmin, director of research and education programs at the Stanford Health Communication Initiative. “They’re looking for a whole picture.”
Most polls have shown far from universal acceptance of vaccines, with only 50% to 70% of respondents willing to take the vaccine. Black and Hispanic Americans are even less likely to take it so far.
Meanwhile, the future course of the coronavirus in the U.S. depends on whether Americans take public health guidance to heart. The Institute for Health Metrics and Evaluation projected that, without mask mandates or a rapid vaccine rollout, the death toll could rise to more than 500,000 by April 2021.
“How can we come to terms with all that when people are living in separate informational realities?” Starbird said.
As the first Americans receive COVID vaccines, supplies remain limited even for the highest-risk populations. And with doses now in the pipeline, states are facing more intense questions about how they will prioritize vaccine delivery across demographic and at-risk groups. The graphic above shows an estimated vaccination timeline, based on the Centers for Disease Control and Prevention’s (CDC) recommended schedule. It illustrates the relative size of different populations in each allocation phase, along with the likely difficulty of targeting them and verifying eligibility. The first phase is divided into three waves (1a, 1b, 1c) for at-risk populations and essential workers, while the second phase includes the rest of the adult population, as well as children (though pediatric clinical trials are still in early stages).
Unsurprisingly, the CDC recommends that those most at risk for infection and severe disease—healthcare workers and nursing home residents—receive the 20M doses available by year’s end.While most states are generally adhering to the initial recommendations on priority groups for phase 1a set by the CDC’s Advisory Committee on Immunization Practices (ACIP), several have made adjustments. At least three are including law enforcement personnel in phase 1a, and others are further categorizing healthcare workers into high-, medium-, and low-risk groups. This weekend, ACIP will reconvene to create its official recommendations for phases 1b and 1c, which include the much larger populations of adults over age 65, and those with high-risk medical conditions.
Beyond eligibility guidelines, larger questions loom. How would someone “verify” that they have a high-risk condition? Who will reach out to older Americans to let them know they are eligible, and where to access the vaccine? As vaccine rollout continues, providers should anticipate the role they will likely play in managing patients “in the queue”, documenting eligible conditions and establishing regular information channels to keep people informed about the current status of vaccine planning and access.
But first, we have a difficult period to get through. This week again saw record-breaking numbers of cases, hospitalizations, and deaths from COVID-19, with Thursday alone bringing more than 238,000 new cases—and a staggering 3,293 fatalities.
Nearly 115,000 Americans are currently hospitalized with COVID, a rise of 16 percent from just two weeks ago, and in many places a precarious capacity situation has turned perilous. Conditions have worsened precipitously in California, with only Tennessee, Oklahoma, and Rhode Island registering more daily COVID cases per 100,000 population than the Golden State, although cases are still on the rise across 80 percent of states and territories.
Intensive care availability in Southern California hit zero, with ICU volume there expected to double or triple by this time next month. The same stresses are playing out in dozens of markets across the country, leading to a staffing sustainability crisis that can’t be solved through paying overtime, cancelling vacations or looking to travel nurses to fill the gaps in a now nationwide crisis. With the Christmas and New Year’s holidays still ahead, experts predictCOVID cases won’t peak until sometime in mid-January, with a peak in hospitalizations and deaths following several weeks after.
Several states and cities tightened restrictions on gatherings and issued new stay-at-home orders, in an effort to keep new cases at a level that allows hospitals to manage through the next several weeks and maintain care quality and access for COVID and non-COVID patients alike. The coming weeks will require every American to take greater precautions than at any time during the course of this pandemic.
On Monday, at Long Island Jewish Medical Center in New York City, critical care nurse Sandra Lindsay rolled up her sleeve andbecame the first American to receive Pfizer and BioNTech’s newly approved COVID vaccine, opening a new front in the nation’s battle with the coronavirus pandemic.
By Friday, nearly 50,000 doses of the vaccine had been administered nationwide, with millions more expected before year’s end. Amid a complex rollout that has already raised questions about the timely distribution of doses, the Food and Drug Administration (FDA) confirmed that it was safe to use every last drop of the Pfizer vaccine, including the excess amount used to fill the five-dose vials of the precious medicine—meaning many vials may have enough to immunize a sixth person.
Based on Thursday’s recommendation from a key panel of experts, the FDA is expected to approve a similar vaccine from Moderna as soon as Friday evening, with doses of that vaccine beginning to be administered by next week. The Moderna vaccine comes in smaller packages with less-demanding storage requirements, making it suitable for a wider distribution across smaller settings and remote areas.
Pharmacy chains CVS and Walgreens were set to begin administering shots to nursing home residents in Ohio, Connecticut, and Florida on Friday, as part of an agreement with the US government to vaccinate staff and residents in 75,000 long-term care facilities nationwide.
In an interview this week, Secretary of Health and Human Services (HHS) Alex Azar said that the vaccine could be widely available to the general public as soon as late February or early March. While it’s surely tempting to fixate on every setback, second guess every decision about prioritization and distribution, and fret over every isolated report of an adverse vaccine reaction, it will be important in the coming weeks to keep the big picture in mind: we are on the way to beating back the coronavirus. The end is nigh.
Britain’s medicine regulator said anyone with a history of anaphylaxis to a medicine or food should not get the Pfizer-BioNTech COVID-19 vaccine, giving fuller guidance on an earlier allergy warning about the shot.
Starting with the elderly and frontline workers, Britain began mass vaccinating its population on Tuesday, part of a global drive that poses one of the biggest logistical challenges in peacetime history.
The Medicines and Healthcare Products Regulatory Agency (MHRA) said there had been two reports of anaphylaxis and one report of a possible allergic reaction since rollout began.
“Any person with a history of anaphylaxis to a vaccine, medicine or food should not receive the Pfizer BioNTech vaccine,” MHRA Chief Executive June Raine said in a statement.
“Most people will not get anaphylaxis and the benefits in protecting people against COVID-19 outweigh the risks… You can be completely confident that this vaccine has met the MHRA’s robust standards of safety, quality and effectiveness.”
Anaphylaxis is an overreaction of the body’s immune system, which the National Health Service describes as severe and sometimes life-threatening.
The fuller guidance, clarifying that the main risk was from anaphylaxis specifically, was issued after consulting experts on allergies. The MHRA had initially advised anyone with a history of a “significant allergic reaction” not to take the shot.
Pfizer and BioNTech said they were supporting the MHRA’s investigation.
Last week, Britain’s MHRA became the first in the world to approve the vaccine, developed by Germany’s BioNTech and Pfizer, while the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) continue to assess the data.
A top U.S. official said on Wednesday that Americans with known severe allergic reactions may not be candidates for Pfizer’s COVID-19 vaccine until more was understood about what had happened.
Canada’s health ministry said it would look at the reported adverse reactions in Britain, but said adverse events were to be expected and would not necessarily change the risk/benefit of the shot, after the country approved the vaccine.
ALLERGIC REACTION
MHRA chief Raine told lawmakers such allergic reactions had not been a feature of the Pfizer’s clinical trials.
Pfizer has said people with a history of severe adverse allergic reactions to vaccines or the candidate’s ingredients were excluded from their late stage trials, which is reflected in the MHRA’s emergency approval protocol.
However, the allergic reactions may have been caused by a component of Pfizer’s vaccine called polyethylene glycol, or PEG, which helps stabilise the shot and is not in other types of vaccines.
Imperial College London’s Paul Turner, an expert in allergy and immunology, who has been advising the MHRA on their revised guidance, told Reuters: “As we’ve had more information through, the initial concern that maybe it affects everyone with allergies is not true.”
“The ingredients like PEG which we think might be responsible for the reactions are not related to things which can cause food allergy. Likewise, people with a known allergy to just one medicine should not be at risk,” Turner told Reuters.
The EMA said in an email that all quality, safety and efficacy data would be taken into account in assessing the vaccine, including data generated outside the EU.
In the United States, the FDA released documents on Tuesday in preparation for an advisory committee meeting on Thursday, saying the Pfizer vaccine’s efficacy and safety data met its expectations for authorization.
The briefing documents said 0.63% of people in the vaccine group and 0.51% in the placebo group reported possible allergic reactions in trials, which Peter Openshaw, professor of experimental medicine at Imperial College London, said was a very small number.
“The fact that we know so soon about these two allergic reactions and that the regulator has acted on this to issue precautionary advice shows that this monitoring system is working well,” he said.
However, Gregory Poland, a virologist and vaccine researcher with the Mayo Clinic in Rochester, Minnesota, said that the MHRA and NHS had overreacted initially.
“I would not have broadened to the degree they did,” he said.
“It’s reasonable to let the world know about this, and to be aware of it in terms of people who have had reactions like this to vaccines. I think to say medicines, foods or any other allergies is past the boundary of science.”