

Cartoon – Being in the Loop


HBO’s critically acclaimed series Succession recently concluded its fourth and final season with a crescendo of family dramatics and falls from grace. If you haven’t seen the finale, bookmark this article for later. It contains spoilers.
Succession, for those unfamiliar, centers on the uber-wealthy Roy family, majority owners of the global media and entertainment subsidiary Waystar Royco. The plot revolves around the bullishly Machiavellian patriarch Logan Roy and his four adult children, each of them seeking (a) control of the family business and (b) their dad’s approval.
During its run, the show’s endless infighting and fascinating archetypes captivated viewers. But the 39-episode series also provided enduring lessons in dysfunctional leadership, which apply directly and saliently to U.S. healthcare.
As with Waystar Royko, the institutions of medicine (hospitals, medical groups, insurers, pharma and med-tech companies) need excellent leadership just to survive. With millions of dollars and hundreds or thousands of jobs resting on the decisions of top administrators, any major flaw can prove fatal—erasing decades of organizational success.
In any industry, poor leadership can undermine performance and threaten livelihoods. In healthcare, poor leadership puts lives at risk. Here are five dangerous types of leadership personalities, each inspired by a character from Succession:
In the show’s second season, Connor, the eldest and oft-forgotten son of Logan Roy, launches his U.S. presidential campaign on a “no-tax” platform. When the eve of election arrives, he’s polling at less than 1%, yet he refuses to step aside, still convinced he is capable of doing the job.
Like Connor, healthcare’s delusional leaders overestimate their abilities. Their ideas are unrealistic and their vision for the future: pure fiction. But no matter how outlandish their outlook, delusional leaders will always find apostles among the disenfranchised who, themselves, feel undervalued and overlooked.
When confronted with the harshness of reality, deluded leaders and their followers double down, insisting that everyone else is myopic. “Just follow and you’ll see,” they demand.
Unless senior executives or board members step in to relieve this leader of power, the organization will be as doomed as Connor Roy’s bid for presidency.
On the surface, Kendall is by far the most capable and experienced candidate to succeed his father. He’s a smart and articulate heir apparent who appears up to the task of CEO.
But underneath the gold plating, his every action is reflexively self-centered. As such, when the time comes to sacrifice something of himself for the good of the company, he freezes and falters, his decisions corrupted by the compulsion to put himself first.
Like Kendall, healthcare’s narcissistic leaders bask in praise and blind loyalty. They reject and punish those who provide honest feedback and fair criticism. Their obsession with status and self-importance blinds them to long-term threats and opportunities, alike.
Unlike delusional leaders, who fail because their vision cuts against the grain of reality, the narcissistic leader’s passion for winning may advance an organization—in the short run. Long-term, however, their flaws will be exposed and weaknesses manipulated by seasoned competitors.
Across four seasons, Kendall can’t fathom that anyone else might be a better choice to run the company. As a result, he underestimates a rival CEO who’s seeking to acquire Waystar, and he overestimates the loyalty of his siblings. In the end, he’s left hopeless and broken.
Roman, the youngest Roy, is brash and witty, but also unpredictable and unrestrained. His penchant for foul language and cutting insults make for good television, but they’re the telltale signs of insecurity and immaturity.
Like all immature leaders, Roman is addicted to novelty and excitement, often acting without regard for the consequences. He’s fast-talking and loud, which makes him likable enough for many to overlook his incompetence. But he’s incapable of filling his father’s shoes.
Immature leaders get promoted before they’re primed and polished. They often lack boundaries and excel at the sport of making others uncomfortable. At times, they seem more interested in causing a scene than creating results. They chase big ideas—if only for the adrenaline rush—but can’t accurately calculate whether the risk of failure is 20% or 80%. This makes them very dangerous as leaders.
In a world of deluded and despotic men, Shiv comes across as the voice of reason. Smart and strategic, relaxed and composed, Shiv carefully cultivates new allies but never establishes an identity of her own. This makes her an excellent political consultant (the job she has) but a poor candidate for CEO (the job she wants).
Political leaders are better at advancing within an organization than advancing the organization itself. Like chameleons, these leaders change with the scenery, shifting alliances and values as organizational power waxes and wanes. While they’re busy focusing on rumors and relationships, they fail to muster real-life business acumen and experience.
Colleagues rarely respect those who play organizational politics. Once political leaders have accrued enough power and advanced their careers to the max, their shallow alliance and inability to drive performance leaves them stranded at the top—with nowhere to go but down.
Not technically a Roy, Tom is Shiv’s husband and an eager aspirant for CEO.
Once appointed head of Waystar’s struggling cruises division, Tom conceals damaging information to protect his father-in-law. He is a willing henchman, ready to sacrifice his ethics for a shot at the corner office. To advance his interest, Tom repeatedly compromises his integrity, first with Logan, then Kendall, and eventually Lukas Matsson, the incoming global CEO who completes the hostile takeover of Waystar.
In what proves to be Tom’s final interview for U.S. CEO, Matsson asks him whether he will be willing to play the role of “pain sponge,” absorbing any negative fallout the company may experience. After he responds positively, Matsson tests him further by mentioning that he’d like to have sex with Shiv. While viewers squirm in their seats, Tom doesn’t object. For him, every compromise is simply a means to an end.
Compromised leaders are skilled at making promises. They seek support by vowing to fulfill wants and palliate pains. Depending on who these leaders aim to please, they’re willing to slash budgets or raise salaries, regardless of the financial impact. Ultimately, they’ll do anything to keep people happy, even if they have to sink the business in the process.
In the final season of Succession, Logan tells his offspring, “I love you, but you are not serious people.” He is both accurate and accountable. Logan was not a serious father and, as a result, his kids were poorly equipped for life and leadership.
The healthcare industry is replete with stories of once-successful institutions falling on hard times under poor leadership. Although there’s no one way to run an organization, all great healthcare leaders share three characteristics:
Leaders have three jobs. They must create a vision, align people around it and motivate them to succeed. To accomplish these tasks, executives may use carrots and sticks, incentives and disincentives, or positive and negative reinforcement. But these tactics will fail unless they reflect a clear mission and purpose.
Years ago, former CMS administrator Don Berwick started a program with an audacious goal of maximizing patient safety and preventing unnecessary deaths. He called it the 100,000 Lives Campaign. And when he spoke of the program, he leaned hard on its righteous mission. Instead of presenting metrics and statistics, he talked about the weddings and graduation ceremonies that parents and grandparents would attend, thanks to the program and the people behind it. Even hard-weathered clinicians in the audience had tears in their eyes.
Financial incentives drive change in healthcare, but rarely achieve the outcomes intended. Everyone engaged in the 100,000 Lives Campaign knew exactly what they needed to accomplish and were motivated to do so.
Bold ideas and glittering promises always capture attention. Words are powerful and relationships can take aspiring leaders far. But when it comes time to turn big plans into action, there is no substitute for a leader who has been there and done it well.
Exceptional performance, not promises, separate great leaders from the rest—and success from failure. In every industry, past performance is the best predictor of future success. Of course, poor leaders can get lucky and even great ones in bad circumstances may fail. But the odds always favor those who have achieved recurring success throughout their careers.
Emerging leaders can work on their weaknesses. Coaching, training and even therapy can help them quell maladaptive behaviors.
But everything changes when an emerging leader becomes the head of an organization and faces a crisis. As risks and pressures intensify, people tend to fall back on approaches and habits they learned in the past, particularly problematic ones. Whenever tested, the Roy children did exactly that.
After Logan’s death early in the final season, the fatal flaws of each Roy child came into clear view. As a result, the Waystar board made the safest choice for successor: none of the above.
Like a true Shakespearean tragedy, the flaws of the characters in Succession exceeded their abilities.
In healthcare, that’s a guaranteed prescription for failure.

Here’s where we are:
Physician income has not kept pace with inflation and administrative costs prompting 70% to leave private practice. Half are now employed by hospitals and another 20% by private equity-backed practice managers. Both trends began before the pandemic in response to tougher financial conditions for physicians across all specialties. While hospitals held their own at the sector level, physicians lost ground. Per CMS’ NHE analysis, from 2000 to 2021:
In tandem with the erosion of finances for medical practices, investments in medical practices by private equity grew. Per Pitchbook, there have been 874 practice acquisitions by PE/Venture backed sponsors in the last 12 years with 20 in the first half of this year alone. Most of these are small ($7.53 million/transaction) and most involve a tuck-in to an existing PE backed platform (i.e., Privia, Sheridan, et al). Rightfully, physicians point out that while hospitals and drug companies have protected their piece of the health care pie successfully for 20 years while physicians have lost ground.
Physicians are not happy and burnout is pervasive. The employment of physicians in hospital and private equity settings has not made life happier for physicians. Per Medscape’s most recent assessment, burnout increased to 53% in 2022–up from 47% in 2021 and 26% since 2018. More than one in five physicians (22%) reported experiencing depression—up from 15% since 2018. They’re anxious about the future and increasingly sensitive to compensation comparisons with professions that require less training and earn more. They’re suspicious of consultants, lawyers and bankers whose experience is limited but fees inexplicably high They’re incensed by executive compensation in hospitals, drug companies, and health insurer settings they deem overpaid and overhyped. And they resent execs in for-profit and private equity companies who achieve astronomical wealth via their stock-option packages earned on the backs of the physicians they control.
The realities are these:
Physicians lack a strong voice. The American Medical Association’s membership includes less than a third of active-practice physicians. It is increasingly under-fire for under-representing primary and preventive health providers in its government-authorized monopoly on coding, its lobbying efforts against scope of practice expansion for APNs and pharmacists, its opposition to medical training innovations that could significantly improve the readiness and effectiveness of the physician workforce and more. The AMA’s influence is strong on a shrinking number of issues and increasingly resonate out of touch on issues that resonate with voters and lawmakers (expanded scope of practice for nurses and pharmacists, price and outcome transparency, et al).
Physicians operate in a buyers’ market but behave like it’s a sellers’ market. Physicians are trained to think of themselves as the hub of a system in which what they say determines what everyone else does…including patients. They are conditioned in medical school, residency and practice to be self-centered and resist efforts via data, clinical practice redesign or even “value-based incentives” to change their behaviors. They despise the notions of price transparency, cost effectiveness and outcome-based comparisons to their peers while calling for more accountability from hospitals, insurers and drug companies. They discount notions of consumerism and self-care and believe report cards over-rate patient experiences since medical practice is uniquely complicated.
Most live in a buyers’ market mentality unwilling/unable to see the sellers’ market healthcare has become. Otherwise, price transparency would be prevalent, operating hours and support services more conducive to the needs of patients and digital investments to maintain connectivity significant…but most don’t.
My take:
The U.S. economy will be testy for the 12 months: bringing down inflation will require interest rate hikes. Unemployment will increase slightly, wage inflation will slow, and the 2024 election cycle will draw unwelcome attention to healthcare spending and its affordability as root causes of growing financial insecurity in American households.
Given this backdrop, the profession of medicine faces a tipping point: become an integral part of the system’s solution or a vestige of its past. That solution should address medicine’s role in…
How value-based and alternative payment models figure into this is anyone’s guess. Some physician organizations (AAPG, NAACO, et al) are all-in for expansion of these while others note their lackluster results to date. And physician calls for a replacement to RVU-based conversion-factor will grow louder as Congress revisits MACRA and how Medicare pays physicians.
These are important and require urgent attention, but they do not elevate the profession to its rightful place at the center of system transformation.
I hold the profession of medicine in high regard. I respect and trust my physicians—Ben, Ben and Blake are trusted friends in my personal journey to health. But their profession as a whole appears stuck in the past and unable to play a central role in the health system transformation. Until and unless new physician leaders with fresh thinking about the entire system step up, the profession’s role will continue to erode.
Playing the victim card and blame game against Medicare, hospitals, insurers, drug companies and everyone else they deem unworthy will not solve the health system’s problems.
I believe conditions are right for physicians to seize the moral high ground and lead the needed reset of the health system but most aren’t ready.
https://mailchi.mp/edda78bd2a5a/the-weekly-gist-june-23-2023?e=d1e747d2d8

With more than two in five American adults considered obese, the potential for GLP-1 agonist drugs like Wegovy, Ozempic, and Mounjaro to revolutionize obesity treatment seems limitless.
In the graphic above, we looked to quantify how much these drugs could potentially change healthcare expenditures and demand. Using Wegovy’s list price of $1.3K per month, a GLP-1 drug prescription for every obese American adult would cost as much as $1.3T annually—30 percent of total US healthcare expenditures.
Analyst projections of GLP-1 drugs forecast revenue to grow by over 5x by 2028, from $3 billion to $16 billion annually. While it’s unlikely that every overweight American will access the drugs, growing use of GLP-1 agonists will likely drive down obesity rates, and downstream care demand could shift in expected and unpredictable ways. Demand for weight-related surgeries, including joint replacements and bariatric surgery, will likely drop. Incidence of chronic diseases like diabetes and cardiovascular disease could also drop, potentially raising life expectancy.
But even if we’re living longer thanks to the new drugs, we’ll still die of something eventually: expect a secondary rise in cancers and Alzheimer’s, as well as surging demand for eldercare. While these effects will take years to materialize, leaders planning for long-term care needs would be wise to consider scenarios where these and other potential “blockbuster” drugs may disrupt demand patterns and spending for a wide range of services.
https://mailchi.mp/edda78bd2a5a/the-weekly-gist-june-23-2023?e=d1e747d2d8

On Tuesday, the US Preventative Services Task Force (USPSTF), which is appointed by an arm of the Department of Health and Human Services, finalized guidance that all adults ages 19 to 64 should be routinely screened for anxiety, even in the absence of symptoms. Last fall, USPSTF proposed a draft version of this guidance, and also finalized its recommendation that children and adolescents ages 8-18 be screened for anxiety. The task force found that anxiety screening for seniors, as well as suicide-risk screening for all adults, lacked conclusive evidence of effectiveness.
The Gist: Policymakers and providers are right to respond to the nationwide increase in anxiety and depression brought on by the pandemic, and regular screenings will help quantify the scope of a problem we face.
However, given the pervasive undersupply of behavioral health practitioners, widespread screenings will only lead to better care if access to treatment can be scaled.
Solutions that take advantage of telemedicine’s success in behavioral health, combined with the tools—and time—to manage mild anxiety in the primary care setting, are critical to provide support for a coming wave of newly identified patients.
https://mailchi.mp/edda78bd2a5a/the-weekly-gist-june-23-2023?e=d1e747d2d8

This month, a panel of expert advisers recommended the Food and Drug Administration (FDA) grant full approval to Leqembi, a drug developed by Eisai and Biogen that targets amyloid plaques in the brain that are linked to the development of Alzheimer’s.
The drug was found to slow cognitive decline in patients by 27 percent over 18 months, though not without some serious side effects, including brain swelling and bleeding. While Leqembi received accelerated FDA approval in January 2023, it is now likely to become the first Alzheimer’s drug that slows the progression of the disease to secure full FDA approval. The Centers for Medicare and Medicaid Services (CMS) recently announced that it intends to cover this new class of Alzheimer’s drugs, as long as prescribing physicians participate in patient registries designed to continue collecting data about the drugs and their efficacy. The FDA is expected to make a final decision on Leqembi by early July.
The Gist: In addition to risks of patient harm, much of the controversy around Leqembi surrounds its $27K list price. Payers, especially Medicare, are worried that it will balloon spending while exposing patients to unaffordable cost-sharing.
With the number of Americans diagnosed annually with Alzheimer’s and other dementias projected to double by 2050, Leqembi has the potential both to help millions and to drive unsustainable spending patterns, and it will be difficult to achieve the former without the latter.
But with full approval likely, a coming frenzy of investor activity to launch memory treatment centers for drug infusion services, capitalizing on the expected huge demand for the drug, seems inevitable.

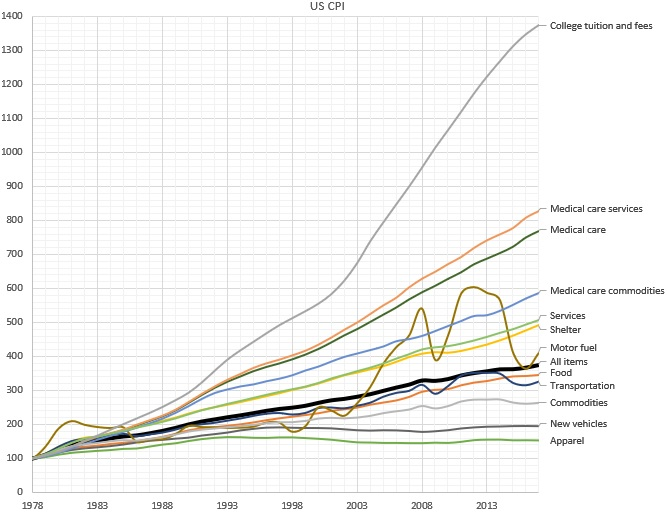
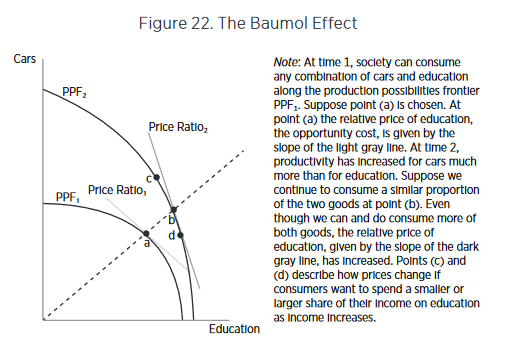
Why does the cost of education and healthcare services continue to rise rapidly, while the cost of goods rise much more slowly? According to economics theory, wages rise when there’s greater productivity; but a rise without an increase in productivity is referred to as “Baumol’s Cost Disease” . In an original study first published in 1966, economist William J. Baumol used the example of a string quartet to illustrate this idea: While the productivity of a given quartet has not increased over time over the last two hundred years, the salary (in nominal and real terms) has increased dramatically.
One way out of this trap is to turn services into goods. Employing a cobbler to make a pair of custom shoes, for instance, is expensive, so we buy factory made shoes: shoes as a good instead of as a service. In doing so, we accept some limitations: a finite set of styles and sizes to choose from; perhaps a less-than-perfect fit for each individual foot; limited styles and customizations — but with the positive trade off in favor of greatly decreased cost. In much the same way, we consume the “good” of the string quartet in the form of a digital recording of a musical piece, instead of the “service” of a live performance. In short, turning services into goods industrializes the process, increasing efficiency and reducing cost.
But is this seemingly alchemical transformation possible in healthcare?
Until today, it’s essentially been accepted as a given that this cost “disease” is incurable where there’s the need for professional, highly trained people performing services — industries like healthcare, education — and therefore drives some of the biggest cost crises of our day, that affect many people in countless ways.
To cure Baumol’s cost disease, we would have to transform the industry’s professional human labor into something that can be manufactured, commoditized, industrialized, and automated. While this has long been an issue in healthcare, for many good and bad reasons, the cure involves bringing more artificial intelligence (AI) to the industry. AI creates a new opportunity: to transform services into goods.
It’s no magic bullet for sure; even our own a16z partners Martin Casado and Matt Bornstein have argued that in enterprise companies, this won’t work, and that AI in this case effectively just replaces human services with different human services with few gains, given all the data cleanup and edge cases involved. But in healthcare, unlike in other industries — like social media content analysis, or self-driving cars — the kind of data labelling needed is actually already an intrinsic part of the healthcare system. In much the same way it is an intrinsic part of Google search — where people choose the most relevant link in the search results, and Google’s AI learns from this, improving with each search — whenever a doctor diagnoses a condition, prescribes a mediation, or interprets an x-ray, that information is then encoded into the electronic health record (EHR). Or, it’s in revenue cycle management — how all bills are paid in healthcare — where people currently perform the manual tasks of identifying what is billable, and to whom. Using AI to learn from these coders (the way, for example, Alpha Health does) means the human work — human labeling — is “free”, since it’s part of what we’re doing anyway.
What’s more, the data is high quality, because when all the doctors in the system are labellers, AI ensures every doctor has the very best teachers in the world — no single doctor alone could ever have that roster of mentors. Training is done on all patients, AI learns from everything, and everybody… and then outputs the results back out to everyone.
AI learns from everything, and everybody… and then outputs the results back out to everyone.
Of course, it’s not a total walk in the park; work needs to be done to integrate this data into the system. One you solve data labelling, you have to train with those labels. Data labelling is just one of the reasons AI based businesses are perceived to have low margins (often requiring an enormous amount of GPU or CPU time, and at great expense. But human training is also expensive: training must often be customized to individuals, and often needs to be redone as employees churn. Because computers are identical, training AI has no such challenges. If you compare the cost of AI training to the cost of executing a simple algorithm, AI training is expensive. If you compare the cost of AI training to the cost of human training, AI is cheap. And, AI training gets exponentially cheaper over time, because of Moore’s Law’s profoundly powerful compounding effects. So even if using AI is at cost parity with a service solution now, the eventual win is obvious. And to some degree, we can commoditize the AI itself as well, for more efficiency, by keeping customization low and training rare with AI.
Another complaint about AI’s ability to transform services into goods is what’s referred to as the “long tail of tasks.” This is the idea that AI won’t be useful if it can only perform a small fraction of what humans can. But in healthcare, even a small fraction of that long tail can have enormous impact. With the right, highly efficient training and labeling, AI can transform perhaps 5% of the human labor of analyzing bills and claims to automate from services to goods. By using AI to learn from medical billing — even just by triaging the “easy” and mundane cases (and escalating the “long tail” of more complex tasks to people as needed) — can bring a dramatic cost savings. Not to mention allowing people to focus on the more higher order aspects of the job, allowing them to deliver better results and service.
We’ve been waiting decades — maybe even centuries — for the ability to reverse Baumol’s Cost Disease in our most service-heavy, yet most critical, industries, such as healthcare.
The transformation of services into goods won’t occur overnight. But Baumol himself couldn’t have foreseen the revolution that AI is creating, any more than someone in the Renaissance anticipating a shoe factory and Moore’s Law since. If applied in the right places, with the right conditions, taking into account the hard realities of the healthcare system, AI can be a vastly powerful lever to pull. We may not cure Baumol’s Cost Disease overnight, but even a small gain in cost and time savings would have huge impacts in healthcare.
https://mailchi.mp/edda78bd2a5a/the-weekly-gist-june-23-2023?e=d1e747d2d8
An in-depth piece co-published this week in New York Magazine chronicles the Kafkaesque working environment of artificial intelligence (AI) annotators, whose “unprecedented feat[s] of tedious and repetitive behavior” have enabled the AI boom. AI learns by training on massive, meticulously labeled datasets, but that training is not some high-tech, futuristic process.
Instead, AI companies of all kinds have secretively hired a vast, global web of millions of low-wage laborers—mostly in the global south—to annotate these large datasets according to precise, convoluted rules sets (one worker reported marking all the knees and elbows in pictures of crowds for 36 hours straight!). AI optimists predict this phase of labor-intensive annotation will pass once the bots advance to the point of automating the annotating process, but most use cases remain far from this goal. Turns out the AI systems are pretty poor students as well: for example, the models need to be explicitly taught the difference between a shirt, and the reflection of a shirt in a mirror, and a shirt on a hangar, and a shirt on a chair, and on and on.
The Gist: If AI needs to be trained by thousands of low-skilled, low-wage workers to identify an elbow, how many doctors will it take to train the algorithms to accurately diagnose a CT scan as cancerous? Thanks to electronic health records, some of this annotation work has been built into the images, but the sensitivity and high price of patient data make it harder to assemble datasets large enough to power the training.
While some remain hopeful that AI has the potential to eventually cure healthcare of Baumol’s cost disease, the path to that point will be paved by significant, tedious manual labor hours performed behind the scenes—adding substantial additional cost and slowing the advent of the long-predicted future of ubiquitous, super-intelligent bots.
