

Cartoon – In Denial

Stillwater Medical Center in Oklahoma has ended all in-network contracts with Medicare Advantage plans amid financial challenges at the 117-bed hospital, the Stillwater News Press reported Oct. 14.
Humana and BCBS of Oklahoma were notified that their members will no longer receive in-network coverage after Jan. 1, 2023.
“BCBSOK is willing to work with Stillwater Medical Center in finding solutions that will allow Payne County residents continued local access to Medicare Advantage providers,” a BCBS spokesperson told the newspaper.
The hospital said it made the decision after facing rising operating costs and a high prior authorization burden for the MA plans.
“This was a very tough financial decision for the Stillwater Medical leadership team. Our cost to operate has increased 26 percent over the past 2 years,” Tamie Young, vice president of revenue cycle at SMC, told the News Press. “Financial challenges are increased by a 22 percent denial of service rate from Medicare Advantage plans. This is in comparison to a less than 1 percent denial rate from traditional Medicare.”

There are few easy ways to cut expenses. But in hospitals and health systems, there are quieter ways.
Workforce reductions are never painless — or never should be, especially for those doing the reducing. Involuntary job loss is one of the most stressful events workers and families experience, carrying mental and physical health risks in addition to the disruption it poses to peoples’ short- and long-term life plans.
But as health systems find themselves in untenable financial positions and looming risk of an economic recession, job cuts and layoffs in hospitals and health systems are increasingly likely. In a report released Oct. 18 from Kaufman Hall based on response from 86 health system leaders, 46 percent said labor costs are the largest opportunity for cost reduction — up significantly from the 17 percent of leaders who said the same last year.
Job cuts at hospitals may seem counterintuitive given the nation’s widely known shortages of healthcare workers. But as hospitals weather one of their most financially difficult years, some are reducing their administrative staff, eliminating vacant jobs and reorganizing or shrinking their executive teams to curb costs.
Decisions to reduce administrative labor tend to garner quieter reactions compared to budgetary decisions to end service lines or close sites of patient care, including hospitals. While the implications of administrative shakeups may be felt throughout a health system, the disruption they pose to patients is less immediately palpable. Few people know the name of their community hospitals’ senior vice presidents, but most do know how many minutes it takes to travel to a nearby site of care for an appointment during a workday or a tolerable amount of time to wait for said appointment.
It doesn’t hurt that hospital and health systems’ administrative ranks have ballooned compared to their patient-facing counterparts. While the number of practicing physicians in the U.S. grew 150 percent between 1975 and 2010, the number of healthcare administrators increased 3,200 percent in the same period. More broadly, administrative spending accounts for 15 to 30 percent of healthcare spending in the U.S. and at least half of that “does not contribute to health outcomes in any discernible way,” according to a report published Oct. 6 in Health Affairs.
A couple of health systems have denoted their plans to cut nonclinical employees and jobs in the past week.
Cleveland-based University Hospitals announced efforts to reduce system expenses by $100 million Oct. 12, including the elimination of 326 vacant jobs and layoffs affecting 117 administrative employees. The workforce reduction comes as the 21-hospital system faces a net operating loss of $184.6 million from the first eight months of 2022.
Sioux Falls, S.D.-based Sanford Health is laying off an undisclosed number of staff, a decision the organization’s top leader says is “to streamline leadership structure and simplify operations” in certain areas, the Argus Leader reported Oct. 19. Bill Gassen, president and CEO of Sanford Health, also said the layoffs primarily affect nonclinical areas and that they will “not adversely impact patient or resident care in any way.”
These developments are only several days old, but have not yet triggered any newsworthy follow-up developments or pushback. Cost reduction efforts that close facilities or reduce services tend to — on the other hand — catalyze scrutiny, debate and conflict in communities that can span for months and even years.
Look to Atlanta. Marietta, Ga.-based Wellstar unexpectedly announced on Aug. 31 that its 460-bed Atlanta Medical Center will end operations on Nov. 1, with plans to progressively wind down services leading up to that date. The system attributed the decision to the $107 million loss incurred operating the hospital over the last 12 months. Noteworthy is that the system has said that 1,430 (82 percent) of Atlanta Medical Center workers affected by the facility’s impending closure have accepted job offers at other Wellstar Health System facilities.
Since, the decision to close one of Atlanta’s level 1 trauma centers has drawn attention from Georgia’s governor and gubernatorial candidate, congressional members and Atlanta Mayor Andre Dickens, who in a town hall Oct. 19 said that in closing Atlanta Medical Center, “Wellstar said they don’t want to be in the business of urban healthcare.”
The decision has also spilled over to affect area hospitals, namely Atlanta’s public Grady Health System, which received a $130 million cash infusion from the state and reported a 30 percent increase in patient volume after the emergency department of Atlanta Medical Center closed.
Health systems have a lot to weigh. Their administrative layers are thick, varied and necessary to a degree, meaning this broad category of workers still poses tough decisions when it comes to cost containment efforts. But in a very simple view, laying off people who care for patients will only hurt health systems’ chances of recruiting and retaining clinical talent — in a time when no health systems’ odds of doing so are especially outsized.
https://mailchi.mp/cd392de550e2/the-weekly-gist-october-21-2022?e=d1e747d2d8
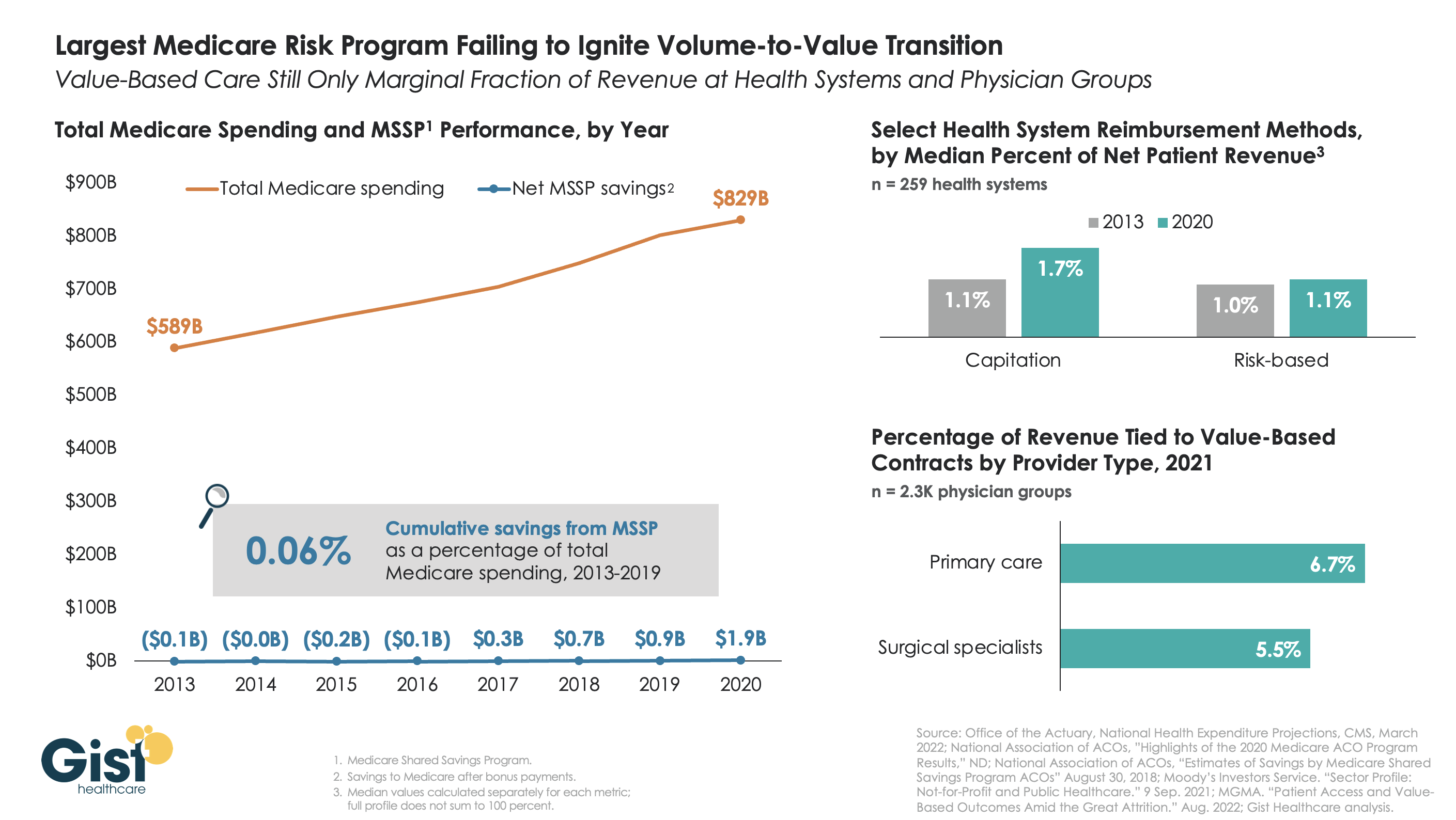
The belief that healthcare should, and would, transition from “volume to value” was a key pillar of the Affordable Care Act (ACA). However, with more than a decade of experience and data to consider, there is little indication that either Medicare or the healthcare industry at large has meaningfully shifted away from fee-for-service payment. Using data from the National Association of Accountable Care Organizations, the graphic below shows that the Medicare Shared Savings Program (MSSP)—the largest of the ACA’s payment innovations, with over 500 accountable care organizations (ACOs) reaching 11M assigned beneficiaries—has led to minimal savings for Medicare. In its first eight years, MSSP saved Medicare only $3.4B, or a paltry 0.06 percent, of the $5.6T that it spent over that time.
Policymakers had hoped that a Medicare-led move to value would prompt commercial payers to follow suit, but that also hasn’t happened. The proportion of payment to health systems in capitated or other risk-based arrangements barely budged from 2013 to 2020—remaining negligible for most organizations, and rarely amounting to enough to influence strategy. The proportion of risk-based payment for doctors is slightly higher, but still far below what is needed to enable wholesale change in care across a practice.
While Medicare has other options if it wants to increase value-based payment, like making ACOs mandatory, it’s harder to see how the trend in commercial payment will improve, as large payers, who are buying up scores of care delivery assets themselves, seem to have little motivation to deal providers in on risk.
While financial upside of moving to risk hasn’t been significant enough to move the market to date, we aren’t suggesting health systems throw out their population management playbook—to meet mounting cost labor pressures, systems must deliver lower cost care, in lower cost settings, with lower cost staff, just to maintain economic viability moving forward.
https://mailchi.mp/cd392de550e2/the-weekly-gist-october-21-2022?e=d1e747d2d8

In a concerning New York Times article, reporter Gina Kolata relates the findings of a recent Health Affairs study that convened focus groups of physicians to anonymously discuss the ways they provide—or too often, don’t provide—care to disabled patients. Many admitted to avoiding seeing patients in wheelchairs and complained about having to provide accommodations to speech-impaired patients, citing the high costs of adapting their clinic operations while dealing with disruptions to workflow. People with disabilities interviewed for the article, including Harvard professor of medicine Dr. Lisa Iezzoni, who ran the study, found its results confirmed impressions of widespread bias against the disabled, which is pervasive across healthcare.
The Gist: Reducing disparities in access and quality of care for disabled people often receives less attention than reducing economic, racial, and gender disparities. What’s revealing about this piece is how these disparities among disabled patients manifest, ranging from personal biases (physicians not wanting or knowing how to care for certain groups of disabled people) to structural challenges (constraints of time, money, and facilities needed for proper care). However, for disabled patients, these factors result in an often substandard and unacceptable healthcare experience, which must be addressed head-on by physician and health system leaders.
https://mailchi.mp/cd392de550e2/the-weekly-gist-october-21-2022?e=d1e747d2d8

In a press release, London-based telemedicine provider Babylon Health said it intends to divest Meritage Medical Network, its 1,800-physician independent practice association located in Northern and Central California. Babylon claims the sale will allow it to better focus on its core business model of digital-first, value-based care contracts. After going public last year at $4.2B, Babylon’s valuation has fallen over 95 percent.
The Gist: Yet another highly touted healthcare startup with digital-first “solutions” has announced a massive pullback in its care footprint. As we wrote about Bright Health last week, these companies have failed to meet investor demands, and must now shutter services or sell assets to buy time to prove their core business model can actually turn a profit.
In Babylon’s case, integrating established physician practices into a digital-first, value-based care model was always going to be costly, challenging and time-consuming—too slow to deliver the returns demanded by an increasingly difficult investor market.
https://www.advisory.com/daily-briefing/2022/10/19/cash-pay-hospitals

Amid new price transparency laws and growing consumer demand, more hospitals are adding cash pay options for certain health care services instead of just accepting insurance, Nora Tepper writes for Modern Healthcare—and some hospital officials say these offerings are “only going to go up” in the future.
Providers advertising cash pay rates for their services used to be considered an “anomaly,” Tepper writes. Now, the No Surprises Act, the federal price transparency law, and changing consumer expectations may make cash-only payments for health care services more common.
“The market is going there,” said Larry Van Horn, associate professor of management, law, and health policy and executive director of health affairs at Vanderbilt University. “You’ve got direct primary care, you’ve got physicians going and moving into cash pay. You’re gonna have to sit there at some point and say, ‘Wait a minute, they’re taking my business.'”
Although some hospitals and health systems that serve certain populations—such as Pomerene Hospital in Ohio with Amish and Anabaptist patients and the University of Texas MD Anderson Cancer Center with medical tourists—have long had cash-pay systems, it is still a relatively new concept for most providers in the United States.
According to data from Medscape, which surveyed more than 17,000 clinicians, just 17% of clinicians used cash-only, concierge, or direct-pay primary care models in 2020. Primary care providers (PCPs) made up the largest proportion of providers accepting cash pay, with 10% of practices charging patients a flat monthly fee for unlimited services.
“[S]ome providers embracing the cash pay revolution say their bottom line benefits from faster reimbursement, lower administration costs and higher patient retention,” Tepper writes.
In a 2020 report from the Society of Actuaries, almost all PCPs who operated under self-pay models reported “better or much better” personal and professional satisfaction compared to those under a traditional fee-for-service system. In addition, 34% of respondents reported “better or much better” earnings under a direct payment model.
According to Tepper, hospitals generally offer self-paying patients, who have typically been uninsured individuals or those with high-deductible health plans, lower rates for services compared to commercial insurers since they don’t have to handle administrative work or collections.
In a 2021 study published in JAMA Network Open, researchers analyzed rates for “shoppable” services at 922 hospitals and found that the proportion of hospitals that had lower cash prices than their median commercial negotiated rate ranged from 38.4% for liver tests to 68.5% for C-sections.
During the pandemic, more insured patients began to inquire about what services they could pay cash for, leading some health systems to create new payment models for certain procedures.
For example, Deaconess Health System launched an in-house bundled payment program, which includes cardiology, radiology, and urgent care services, in July 2020. The first year, the health system sold 130 bundled services, which increased to 351 in 2021, and 489 as of August 2022.
For any services not covered by the program, Deaconess offers a 50% discount on cash payments compared to its insurer rate. However, self-paying patients are required to pay the full cost of a procedure upfront.
“The patient has decided to take a bet on themselves,” said Steve Russell, VP and chief revenue cycle officer at Deaconess. “They have a high deductible, they don’t think they’re going to reach that threshold and their thought is, ‘If I don’t use my insurance, what kind of discount can you give me?'”
Separately, CommonSpirit Health‘s Catholic Health Initiatives (CHI) launched its own bundled cash price program in 2018 after noticing that many patients with high-deductible plans would defer care due to affordability concerns. The health system also advertises and sells its services on MDsave, an online marketplace that allows consumers to shop for health care procedures.
“With the No Surprises Act and the price transparency regulations, this has to be something that we offer,” said Jeanette Wojtalewicz, SVP and CFO at CHI Health’s Midwest division. “You’ll see more of this coming.”
According to Aaron Miri, SVP and chief digital and information officer at Baptist Health South Florida, although few patients are currently paying directly for health care services, the industry is heading towards that direction, which means health systems need to be prepared to meet the demand.
“When you look at the directionality of demand, this is only going to go up,” Miri said. “Patients are going to start seeing their total estimated bill and say, ‘I want to spend my $500 at a health system that was really transparent with me, and made me feel comfortable, versus the health system down the road that I’ve always gone to, but that simply can’t tell me what my actual amount due is.”
To make it easier for patients to directly pay for procedures, some health systems, including Baptist Health, have updated their payment options by adding Apple Pay, Google Pay, or other online payment systems instead of just accepting payment in-person or by phone.
However, even as direct payment models become more common, some insurers are “using their leverage to slow adoption of cash pay,” Tepper writes.
Kimberly Scaccia, VP of revenue management at MercyHealth, said some of the health system’s contracts with insurers prohibit it from offering cash discounts to insured patients.
“Some of the smaller payers, they’re fine with removing [cash pay restrictions],” Scaccia said. “Some of the very, very large payers, they simply will not allow it.”
In addition, Matthew Fiedler, a senior fellow of economic studies at the USC-Brookings Schaeffer Initiative for Health Policy, said clinicians may also be concerned about insurers asking to pay the lower cash rate during contract renewals or jeopardizing a provider’s network position.
“An insurer could say, ‘We’re gonna put this provider out-of-network, but we’re gonna put them in a preferred out-of-network position in our benefit design, where the cost-sharing is not that onerous, because we know they have this really good cash price,'” Fiedler said.

