Cartoon – Artificial Intelligence

Nonprofit hospitals are bracing for a challenging few months as healthcare and social assistance job vacancies remain high against a backdrop of low unemployment, Fitch Ratings said in an Oct. 25 update.
Healthcare and social assistance job openings fell for two consecutive months to 7.7 percent as of August, but the number of openings remains above the highest level recorded before the COVID-19 pandemic.
One encouraging sign is the slowly declining number of quits — 2.3 percent (486,000 quits) in August 2022 compared with a peak of 3.1 percent (626,000 quits) in November 2021. However, current quit rates remain high and are on track to exceed last year, according to Fitch.
“[not-for-profit] hospital quits will need to normalize to well below pre-pandemic levels in order to reduce staffing shortages and a reliance on contract/temporary labor,” Fitch Director Richard Park said in the news release.
The labor shortage saw hospital employees’ average weekly earnings increase 21.1 percent since February, significantly higher than the 13.6 percent earnings growth of overall private sector employees, according to Fitch. But ambulatory healthcare services employees’ earnings increased by only 12.6 percent over the same period.
“Wage increases and employee recruitment challenges may amplify the role of ambulatory care in the overall healthcare sector and continue the acceleration of inpatient care to outpatient settings,” Mr. Park said.
Due to the ongoing recess leading to the midterm elections, very important legislation introduced in September, H.R. 8800 – Supporting Medicare Providers Act of 2022, has stalled.
This critical, bipartisan legislation would stabilize Medicare for physicians and patients because it:
https://www.axios.com/2022/10/20/midterm-election-voters-health-care
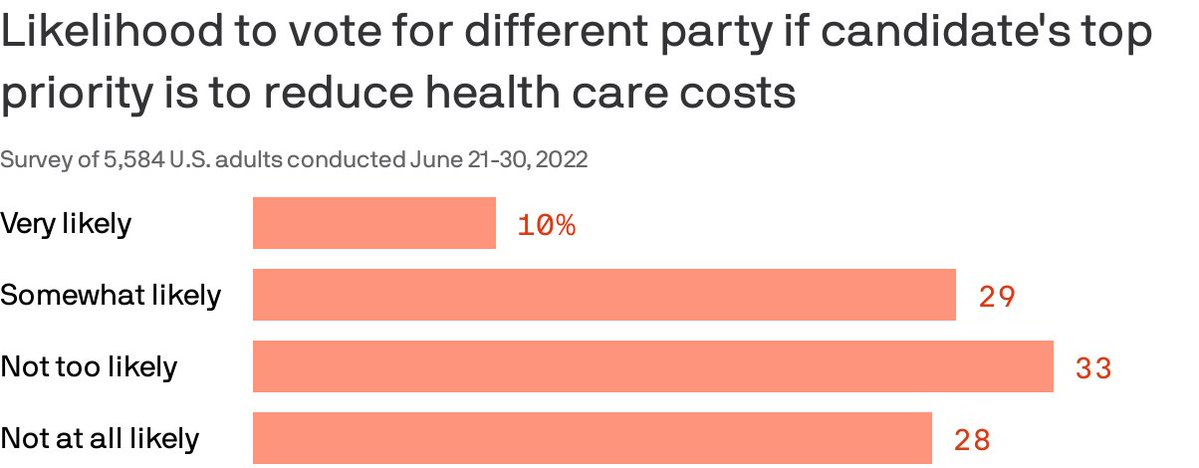
Almost 40% of Americans are willing to split their ticket and vote for a candidate from the opposing party who made a top priority of lowering health costs, according to a Gallup/West Health poll published Thursday.
Why it matters: Though candidates haven’t been talking much about medical costs in the run-up to the midterms, the issue remains enough of a priority that it could erode straight party-line voting.
By the numbers: 87% of Americans polled said a candidate’s plan to reduce the cost of health care services was very or somewhat important in casting a vote.
Of note: Democratic voters were more likely than Republicans to say they would cross party lines because health costs are a top priority. Four in 10 Democrats said they were likely to do so compared to about 1 in 5 Republicans.
https://www.axios.com/2022/10/21/bidens-effort-lower-drug-prices

The next phase of the Biden administration’s bid to curb rising drug costs is in the hands of an under-the-radar federal office called the Center for Medicare and Medicaid Innovation (CMMI).
Driving the news: The center will publish a report within three months on how it can use new payment and delivery models to lower drug costs and boost access to treatments for beneficiaries of the two government health programs, per a recent executive order from President Biden.
Zoom in: CMMI was created through the Affordable Care Act to experiment with new ways of paying for and delivering health care.
Be smart: The expectation is the center will tackle the prices health providers pay for Medicare drugs like infusions or injectables. Under the Inflation Reduction Act, the government can’t negotiate prices for these drugs until 2028.
Refining policies from recent congressional action on Medicare prescription drug pricing could also be on the agenda.
Flashback: CMMI has tried to tackle drug prices under previous administrations, with mixed success.
Reality check: It could take some time to get new drug pricing experiments up and running.
Don’t forget: The Centers for Medicare and Medicaid Services, the center’s parent, will continue its own work on drug pricing as it implements policies from the Inflation Reduction Act.
Zoom out: Expect to see more from CMMI in the next couple years, on drug pricing reforms and other federal health care policy issues.
https://mailchi.mp/tradeoffs/research-corner-5267789?e=ad91541e82

Earlier this month, the Biden administration officially extended the federal public health emergency (PHE) declaration it had set in place for COVID-19. That means the PHE provisions will stay in effect for another 90 days — until mid-January at least.
When the PHE does end, a number of rules developed in response to the pandemic will sunset. One of those is a provision that temporarily requires states to let all Medicaid beneficiaries remain enrolled in the program — even if they have become ineligible during the pandemic.
Estimates suggest that millions could lose Medicaid coverage when this emergency provision ends. Among those who would lose coverage because they are no longer eligible for the program, about one-third are expected to qualify for subsidized coverage on the Affordable Care Act (ACA) marketplaces. Most others are expected to get coverage through an employer. It remains an open question, though, how many people will successfully transition to these other plans.
A recent paper by health economics researcher Laura Dague and colleagues in the Journal of Health Politics, Policy, and Law sheds light on these dynamics. The authors used a prior change in eligibility in Wisconsin’s Medicaid program to estimate how many people successfully transitioned to a private plan when their Medicaid eligibility ended.
Wisconsin’s Medicaid program is unique. Back in 2008 — before the ACA passed — Wisconsin broadly expanded Medicaid eligibility for non-elderly adults. After the ACA came into effect, Wisconsin reworked its Medicaid program in a way that made about 44,000 adults (mostly parents) with incomes above the federal poverty line ineligible for the program. To remain insured, they would have to switch to private coverage (via Obamacare or an employer).
Using data from the Wisconsin All-Payer Claims Database (APCD), the researchers found that:
This paper has several limitations. Health insurers are not required to participate in Wisconsin’s APCD, so the authors may not be capturing all successful transitions from Medicaid to private insurance. The paper also does not distinguish between different types of private insurance: Some coverage gains may have resulted from employer-based insurance rather than the ACA marketplace.
Still, the findings suggest that when a large number of Wisconsin residents lost Medicaid eligibility in 2014, many were not able to transition from Medicaid to private coverage. Wisconsin’s experience can help us understand what might happen when the national public health emergency ends and Medicaid programs resume removing people from their rolls.