Respiratory syncytial virus, more commonly known as RSV, sends thousands of children to the hospital every year in the U.S. But during September and October 2022, health professionals across the country have watched an unprecedented spike in the number of cases of this usually mild, but occasionally dangerous, respiratory infection in children.Jennifer Girotto is a pharmacist who studies pediatric infectious diseases. She explains how RSV infects the human body, who is most at risk and what might be causing this year’s outbreak to be worse than normal.
1. What is respiratory syncytial virus?
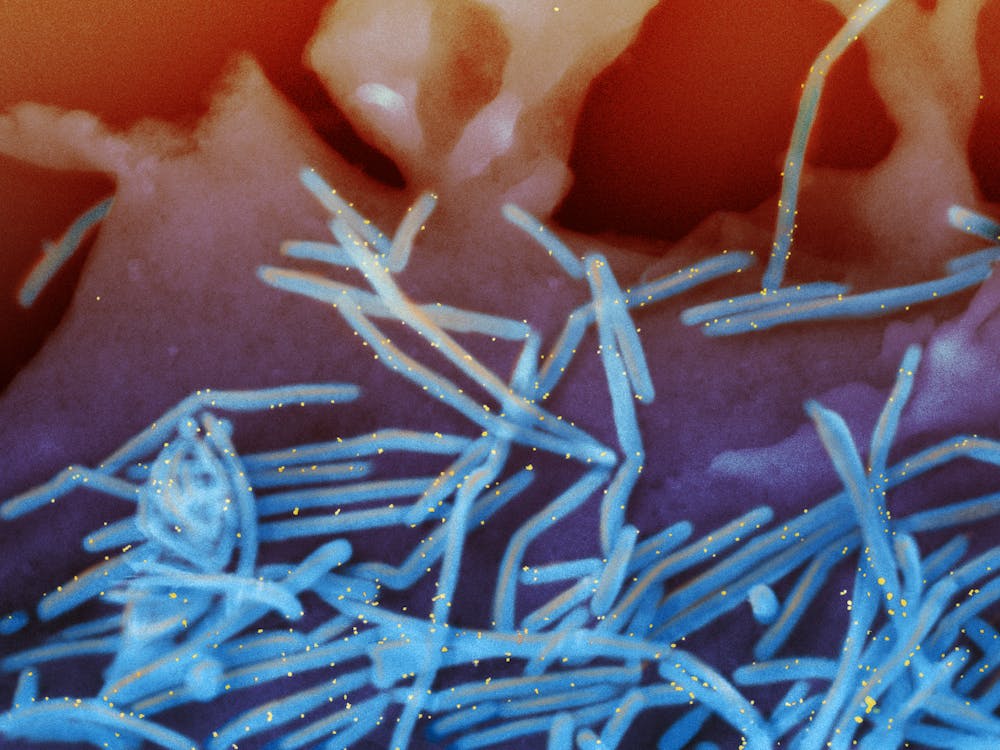
RSV is a common, RNA respiratory virus that affects about 2 million children under 5 years old annually nationwide. Researchers think that most children have been infected by age 2. Like the flu, in most areas of the U.S., RSV usually circulates from November through March and then mostly disappears during the summer months, with only sporadic cases being seen.
For most people, especially those who have had an RSV infection in the past, the virus only causes mild symptoms like cough, runny nose and fever, with instances of wheezing and decreased appetite more common in young children.
But young infants, especially those under 6 months old, born prematurely or with congenital heart, lung or other health issues are at increased risk for more severe symptoms. The U.S. Centers for Disease Control and Prevention estimates that 1% to 2% of infants younger than 6 months who get infected with RSV require hospitalization. In an average year, around 250 children die from the disease.
The main reason RSV sends babies and young children to the hospital is because the virus infects and kills surface cells within small sacs of the lungs. The body responds by increasing the production of mucus and fluid in these areas. But the extra mucus can plug up and obstruct these parts of the lung and make it so that an infant doesn’t get enough oxygen.
A second common cause for hospitalization due to RSV is pneumonia, where a person’s lungs fill up with fluid. The pneumonia can either be triggered by the virus itself or by a secondary, bacterial infection. Finally, some infants get so sick that they struggle to eat and are unable to take in sufficient nutrients, eventually landing them in the hospital.
Health officials aren’t yet sure why the outbreak is so bad this year, but the COVID-19 pandemic may have something to do with it. Some research has shown that seasonality of RSV has shifted. In 2021, RSV infections started much earlier than normal, and over the summer of 2022, they never quite went away. One theory as to why RSV season is starting earlier and hitting harder is that, due to social distancing measures since 2020, an unusually high number of infants and children are experiencing their first exposures and infections at once.
5. How can you protect against catching RSV?
Like colds and the flu, RSV infections spread when people touch dirty surfaces or from respiratory droplets, when an infected person coughs or sneezes.
If someone is sick with symptoms that look like a cold, it may be best to avoid close contact until they feel better, especially if you have young children or high-risk people around.
There are an estimated 19,000 full-time job vacancies across Massachusetts acute care hospitals, according to a survey published Oct. 31 by the Massachusetts Health & Hospital Association.
Hospitals are working to address backlogs and transfer patients to post-acute care settings while skyrocketing labor costs — including a projected $1 billion in travel labor costs this year — are compounding healthcare facilities’ financial woes, according to the report. These challenges are hampering hospital operations as well as leading to care delays and reduced access to care.
Fewer workers mean that fewer beds are available for patients, while the demand for care increases due to deferred care throughout the COVID-19 pandemic, the behavioral health crisis and reduced access to community-based services continue to challenge hospitals throughout the state. At any given time, more than 1,500 patients are in acute hospital beds awaiting placement to a specialized behavioral health bed or post-acute care, according to the MHA.
“Our healthcare system has never been more fragile, and its leaders have never been more concerned about what’s to come in months ahead,” Steve Walsh, president and CEO of the MHA, said in an Oct. 31 news release shared with Becker’s Hospital Review. “They are exhausting every option within their control to confront these challenges, but this is an unsustainable reality and providers are in dire need of support.”
In response to the survey, 37 hospitals — representing 70 percent of the state’s total hospital employment — reported 6,650 vacancies among 47 positions critical to hospital operations and clinical care. The positions range from direct care nurses to lab personnel and clinical support staff. Eighteen of the 47 positions have a vacancy rate greater than 20 percent.
At a 56 percent vacancy rate, licensed practical nurses is the most in-demand position, while home health aides (34 percent), mental health workers (32 percent), infection control nurses (26 percent) and CRNAs (24 percent) are also highly sought after.
Survey respondents identified 6,650 vacancies. The 47 positions included in the survey, which was conducted this summer, account for less than half of all hospital roles. The MHA said it extrapolated that across all positions and hospitals to arrive at an estimated 19,000 vacancies across the state.
Staffing shortages are driving labor costs to an unsustainable level for many hospitals already grappling with margins close to zero or in the red. Hospitals have relied on high-cost temporary staffing to fill critical positions during the pandemic, resulting in average hourly wage rates for travel nurses increasing 90 percent since 2019, according to the report. Massachusetts hospitals reported spending $445 million on temporary registered nurse staffing halfway through the fiscal year, with temporary RN staffing costs increasing 234 percent from fiscal year 2019 to March 2022.
If urgent steps are not taken to address healthcare’s staffing shortage, hospitals will continue to face capacity challenges and overpay for labor, which will lead to fiscal instability, according to Mr. Walsh.
The MHA urged providers, payers, public officials and government agencies to address the workforce crisis by investing in training and education, expanding the workforce pipeline, providing financial support to hospitals and advancing new models of care such as telehealth and at-home care.
Hospitals in the United States are on track for their worst financial year in decades. According to a recent report, median hospital operating margins were cumulatively negative through the first eight months of 2022. For context, in 2020, despite unprecedented losses during the initial months of COVID-19, hospitals still reported median eight-month operating margins of 2 percent—although these were in large part buoyed by federal aid from the Coronavirus Aid, Relief, and Economic Security (CARES) Act.
The recent, historically poor financial performance is the result of significant pressures on multiple fronts. Labor shortages and supply-chain disruptions have fueled a dramatic rise in expenses, which, due to the annually fixed nature of payment rates, hospitals have thus far been unable to pass through to payers. At the same time, diminished patient volumes—especially in more profitable service lines—have constrained revenues, and declining markets have generated substantial investment losses.
While it’s tempting to view these challenges as transient shocks, a rapid recovery seems unlikely for a number of reasons. Thus, hospitals will be forced to take aggressive cost-cutting measures to stabilize balance sheets. For some, this will include department or service line closures; for others, closing altogether. As these scenarios unfold, ultimately, the costs will be borne by patients, in one form or another.
Hospitals Face A Difficult Road To Financial Recovery
There are several factors that suggest hospital margins will face continued headwinds in the coming years. First, the primary driver of rising hospital expenses is a shortage of labor—in particular, nursing labor—which will likely worsen in the future. Since the start of the pandemic, hospitals have lost a total of 105,000 employees, and nursing vacancieshave more than doubled. In response, hospitals have relied on expensive contract nurses and extended overtime hours, resulting in surging wage costs. While this issue was exacerbated by the pandemic, the national nursing shortage is a decades-old problem that—with a substantial portion of the labor force approaching retirement and an insufficient supply of new nurses to replace them—is projected to reach 450,000 by 2025.
Second, while payment rates will eventually adjust to rising costs, this is likely to occur slowly and unevenly. Medicare rates, which are adjusted annually based on an inflation projection, are already set to undershoot hospital costs. Given that Medicare doesn’t issue retrospective corrections, this underadjustment will become baked into Medicare prices for the foreseeable future, widening the gap between costs and payments.
This leaves commercial payers to make up the difference. Commercial rates are typically negotiated in three- to five-year contract cycles, so hospitals on the early side of a new contract may be forced to wait until renegotiation for more substantial pricing adjustments. “Negotiation” is also the operative term here, as payers are under no obligation to offset rising costs. Instead, it is likely that the speed and degree of price adjustments will be dictated by provider market share, leaving smaller hospitals at a further disadvantage. This trend was exemplified during the 2008 financial crisis, in which only the most prestigious hospitals were able to significantly adjust pricing in response to historic investment losses.
Finally, economic uncertainty and the threat of recession will create continued disruptions in patient volumes, particularly with elective procedures. Although health care has historically been referred to as “recession-proof,” the growing prevalence of high-deductible health plans (HDHPs) and more aggressive cost-sharing mechanisms have left patients more exposed to health care costs and more likely to weigh these costs against other household expenditures when budgets get tight. While this consumerist response is not new—research on previous recessions has identified direct correlations between economic strength and surgical volumes—the degree of cost exposure for patients is historically high. Since 2008, enrollment in HDHPs has increased nearly four-fold, now representing 28 percent of all employer-sponsored enrollments. There’s evidence that this exposure is already impacting patient decisions. Recently, one in five adults reported delaying or forgoing treatment in response to general inflation.
Taken together, these factors suggest that the current financial pressures are unlikely to resolve in the short term. As losses mount and cash reserves dwindle, hospitals will ultimately need to cut costs to stem the bleeding—which presents both challenges and opportunities.
Direct And Indirect Consequences For Cost, Quality, And Access To Care
Inevitably, as rising costs become baked into commercial pricing, patients will face dramatic premium hikes. As discussed above, this process is likely to occur slowly over the next few years. In the meantime, the current challenges and the manner in which hospitals respond will have lasting implications on quality and access to care, particularly among the most vulnerable populations.
Likely Effects On Patient Experience And Quality Of Care
Insufficient staffing has already created substantial bottlenecks in outpatient and acute-care facilities, resulting in increased wait times, delayed procedures, and, in extreme cases, hospitals diverting patients altogether. During the Omicron surge, 52 of 62 hospitals in Los Angeles, California, were reportedly diverting patients due to insufficient beds and staffing.
The challenges with nursing labor will have direct consequences for clinical quality. Persistent nursing shortages will force hospitals to increase patient loads and expand overtime hours, measures that have been repeatedly linked to longer hospital stays, more clinical errors, and worse patient outcomes. Additionally, the wave of experienced nurses exiting the workforce will accelerate an already growing divide between average nursing experience and the complexity of care they are asked to provide. This trend, referred to as the “Experience-Complexity Gap,” will only worsen in the coming years as a significant portion of the nursing workforce reaches retirement age. In addition to the clinical quality implications, the exodus of experienced nurses—many of whom serve in crucial nurse educator and mentorship roles—also has feedback effects on the training and supply of new nurses.
Staffing impacts on quality of care are not limited to clinical staff. During the initial months of the pandemic, hospitals laid off or furloughed hundreds of thousands of nonclinical staff, a common target for short-term payroll reductions. While these staff do not directly impact patient care (or billed charges), they can have a significant impact on patient experience and satisfaction. Additionally, downsizing support staff can negatively impact physician productivity and time spent with patients, which can have downstream effects on cost and quality of care.
Disproportionate Impacts On Underserved Communities
Reduced access to care will be felt most acutely in rural regions. A recent report found that more than 30 percent of rural hospitals were at risk of closure within the next six years, placing the affected communities—statistically older, sicker, and poorer than average—at higher risk for adverse health outcomes. When rural hospitals close, local residents are forced to travel more than 20 miles further to access inpatient or emergency care. For patients with life-threatening conditions, this increased travel has been linked to a 5–10 percent increase in risk of mortality.
Rural closures also have downstream effects that further deteriorate patient use and access to care. Rural hospitals often employ the majority of local physicians, many of whom leave the community when these facilities close. Access to complex specialty care and diagnostic testing is also diminished, as many of these services are provided by vendors or provider groups within hospital facilities. Thus, when rural hospitals close, the surrounding communities lose access to the entire care continuum. As a result, individuals within these communities are more likely to forgo treatment, testing, or routine preventive services, further exacerbating existing health disparities.
In areas not affected by hospital closures, access will be more selectively impacted. After the 2008 financial crisis, the most common cost-shifting response from hospitals was to reduce unprofitable service offerings. Historically, these measures have disproportionately impacted minority and low-income patients, as they tend to include services with high Medicaid populations (for example, psychiatric and addiction care) and crucial services such as obstetrics and trauma care, which are already underprovided in these communities. Since 2020, dozens of hospitals, both urban and rural, have closed or suspended maternity care. Similar to closure of rural hospitals, these closures have downstream effects on local access to physicians or other health services.
Potential For Productive Cost Reduction And The Need For A Measured Policy Response
Despite the doom-and-gloom scenario presented above, the focus on hospital costs is not entirely negative. Cost-cutting measures will inevitably yield efficiencies in a notoriously inefficient industry. Additionally, not all facility closures negatively impact care. While rural facility closures can have dire consequences in health emergencies, studies have found that outcomes for non-urgent conditions remained similar or actually improved.
Historically, attempts to rein in health care spending have focused on the demand side (that is, use) or on negotiated prices. These measures ignore the impact of hospital costs, which have historically outpaced inflation and contributed directly to rising prices. Thus, the current situation presents a brief window of opportunity in which hospital incentives are aligned with the broader policy goals of lowering costs. Capitalizing on this opportunity will require a careful balancing act from policy makers.
In response to the current challenges, the American Hospital Association has already appealed to Congress to extend federal aid programs created in the CARES Act. While this would help to mitigate losses in the short term, it would also undermine any positive gains in cost efficiency. Instead of a broad-spectrum bailout, policy makers should consider a more targeted approach that supports crucial community and rural services without continuing to fund broader health system inefficiencies.
The establishment of Rural Emergency Hospitals beginning in 2023 represents one such approach to eliminating excess costs while preventing negative patient consequences. This rule provides financial incentives for struggling critical access and rural hospitals to convert to standalone emergency departments instead of outright closing. If effective, this policy would ensure that affected communities maintain crucial access to emergency care while reducing overall costs attributed to low-volume, financially unviable services.
Policies can also help promote efficiencies by improving coverage for digital and telehealth services—long touted as potential solutions to rural health care deserts—or easing regulations to encourage more effective use of mid-level providers.
Conclusion
The financial challenges facing hospitals are substantial and likely to persist in the coming years. As a result, health systems will be forced to take drastic measures to reduce costs and stabilize profit margins. The existing challenges and the manner in which hospitals respond will have long-term implications for cost, quality, and access to care, especially within historically underserved communities. As with any crisis, though, they also present an opportunity to address industrywide inefficiencies. By relying on targeted, evidence-based policies, policy makers can mitigate the negative consequences and allow for a more efficient and effective system to emerge.
COVID-19 hospitalizations increased slightly this week after nearly two months of decline, while omicron subvariants BQ.1 and BQ.1.1 — dubbed ‘escape variants’ for their immune evasiveness — continued to gain prevalence nationwide, according to the CDC’s COVID-19 data tracker weekly review published Oct. 28.
Ten findings:
Hospitalizations
1. The seven-day hospitalization average for Oct. 19-25 was 3,249, a 1 percent increase from the previous week’s average. New hospital admissions had been falling since early August, CDC data shows.
Cases
2. As of Oct. 26, the nation’s seven-day case average was 37,683, a 25.1 percent decrease from the previous week’s average. This marks the 14th week of decline and the lowest daily case rate seen since late April, CDC data shows.
Variants
3. Based on projections for the week ending Oct. 29, the CDC estimates that BQ.1 accounts for 14 percent of cases, while BQ.1.1 accounts for 13.1 percent.
4. BA. 5 remains the nation’s dominant strain, accounting for 49.6 percent of infections. BF.7, another omicron subvariant experts are closely monitoring, makes up 7.5 percent of cases. Other omicron subvariants make up the rest.
Community levels
5. As of Oct. 27, 2.3 percent of counties, districts or territories had high COVID-19 community levels, 21.9 percent had medium community levels and 75.8 percent had low community levels.
Deaths
6. The current seven-day death average is 373, down 13.7 percent from the previous week’s average. Some historical deaths have been excluded from these counts, the CDC said.
Vaccinations
7. As of Oct. 26, about 266 million people — 80.1 percent of the U.S. population — have received at least one dose of the COVID-19 vaccine, and more than 226.9 million people, or 68.4 percent of the population, have received both doses.
8. About 111.8 million people have received a booster dose, and more than 22.9 million people have received an updated omicron booster. However, 49.3 percent of people eligible for a booster dose have not yet gotten one, the CDC said.
Wastewater surveillance
9. About 34 percent of the U.S. is reporting moderate to high virus levels in wastewater. Of these surveillance sites, 10 percent are seeing some of the highest levels since Dec. 1, 2021.
10. About 50 percent of sites are reporting an increase in virus levels, and 44 percent of sites are seeing a decrease.
Several hospitals and health systems are trimming their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations that were announced within the past month and/or take effect over the next month.
1. Fayetteville, N.C.-based Cape Fear Valley Health is eliminating 200 positions. The decision affects 42 employees in non-direct patient care positions. The other 158 positions were unfilled positions. Employees were informed of the changes Oct. 27.
2. Sioux Falls, S.D.-based Sanford Healthannounced layoffs affecting an undisclosed number of staff on Oct. 19, a decision its CEO said was made “to streamline leadership structure and simplify operations” in certain areas. The layoffs primarily affect nonclinical areas.
3. University Hospitalsannounced efforts to reduce system expenses by $100 million Oct. 12, including the elimination of 326 vacant jobs and layoffs affecting 117 administrative employees. None of the employees affected by job cuts or layoffs provide direct patient care. The workforce reduction comes as the 21-hospital system faces a net operating loss of $184.6 million from the first eight months of 2022.
4. Ascension is closingAscension St. Vincent Dunn, a critical access hospital in Bedford, Ind., and nine medical practices in December, a move that will affect 133 employees. Affected employees who do not secure another position within the health system will be offered severance and outplacement services.
5. Quincy, Ill.-based Blessing Health Systemclosed its hospital in Keokuk, Iowa, Sept. 30. The closure affected 151 workers. The layoffs take effect Nov. 4. The employees will do on-site work or be placed on administrative leave until the layoff date, Blessing Health said.
6. St. Vincent Charity Medical Center in Cleveland will lay off 978 workers when it ends many services in November. The hospital, part of Sisters of Charity Health System, is ending inpatient care and most other services in November. After the transition, the facility will offer outpatient behavioral health, urgent care and primary care.
7. Commonwealth Health, part of Franklin, Tenn.-based Community Health Systems, will lay off 245 employees when it closes facilities at the end of October. The health system is closing First Hospital, a psychiatric hospital in Kingston, Pa., and its various outpatient centers on Oct. 30. Affected workers are encouraged to apply for open positions they’re qualified for at other Commonwealth Health facilities, a system spokesperson told Becker’s.
8. Yale New Haven (Conn.) Healtheliminated 155 management positions from its nearly 30,000-person workforce. The health system laid off 72 employees and eliminated 83 vacant positions, a spokesperson told Becker’s Hospital Review in September. The cuts were attributed to financial pressures.
9. Citing financial pressures, BHSH System — now named Corewell Health — cut about 400 positions from its 64,000-member workforce in September. The 22-hospital organization was formed by the February merger of Grand Rapids, Mich.-based Spectrum Health with Southfield, Mich.-based Beaumont Health.
10. Bakersfield (Calif.) Heart Hospital is laying off 114 employees. Affected employees were told in September that they no longer had to report to work, but they will continue to receive full pay and benefits through Nov. 5. The layoffs are an effort to optimize operations and to free up resources for patient care and specialized surgery, the hospital said.
Early into flu season, nationwide flu activity is ten times higher than at the same point last year. Meanwhile, cases of respiratory syncytial virus (RSV), a virus most severe in young children and the elderly, have tripled in the past two months, with some children’s hospitals reporting “unprecedented” admissions for the virus. And most experts expect at least some winter COVID surge, possibly involving several different variants. The combined threat of these viruses circulating together has been labeled a potential “tripledemic.”
The Gist: Across the past two winters, the widespread adoption of COVID prevention measures, including masking and social distancing, kept the spread of other viruses at bay. But with return to normal life for most Americans, other viruses have returned to circulation—and with a vengeance, as population immunity toward flu and RSV has weakened.
While it’s hard to predict when and where local surges will occur, hospitals struggling with staffing shortages may be forced to hire more contract labor to care for an influx of patients—making this a potentially challenging winter for already stretched facilities.
The plaintiffs in Braidwood v. Becerra filed a motion on Monday asking a US District Court judge in Texas—the same judge who ruled the entire ACA unconstitutional in 2018—to block enforcement of the ACA’s no-cost requirement for preventive care services. This judge already sided with the plaintiffs in September, ruling the government cannot require a company to fully cover preventive HIV drugs, also known as PrEP therapy, for its employees, on the grounds that doing so violates owners’ religious freedom.
In that ruling, the judge also asserted that the government’s system for deciding what preventive care services should be covered under the ACA is unconstitutional. This latest motion now asks him to invalidate all parts of the ACA requiring preventive health services on the grounds that the Preventive Services Task Force was never appointed by Congress, and thus lacks the authority to say which services insurers must cover. The final ruling is expected early next year, after which the case will certainly be appealed, regardless of outcome.
The Gist: Given the judge’s initial ruling in Braidwood last month, this motion from the plaintiffs was expected. While the US Supreme Court reversed a 2018 ruling by this judge that struck down the entire ACA, it could potentially find the narrow targeting of this case more reasonable, making preventive care coverage optional for employers.
If that happens, millions of Americans would once again have to pay for some of the most common and highest-value healthcare services, including screening tests for a variety of cancers, sexually transmitted infections, and diabetes. That additional financial burden, along with likely tightening of health plan benefit designs, would create barriers to access and exacerbate health disparities.
Drawing on a report published by the North Carolina State Health Plan for Teachers and State Employees, a recent Kaiser Health News article shines a light on the lack of transparency in financial reporting of not-for-profit hospitals’ community benefit obligations.
The report claims many North Carolina hospitals—including the state’s largest system, Atrium Health—show profits on Medicare patients in their cost report filings, while at the same time claiming sizable unrecouped losses on Medicare patients as a part of their overall community benefit analyses.
The Gist: These kind of reporting discrepancies draw attention to the controversial issue of whether not-for-profit hospitals provide sufficient community benefit to compensate for their tax-exempt status, which was worth nearly $2 billion in 2020 for North Carolina hospitals alone.
Greater transparency around charity care, community benefit, and losses sustained from public payerscould go a long way toward shoring up stakeholder support for not-for-profit institutions at a time when their political goodwill has deteriorated. Hospitals should be proactive on this front, as political leaders increasingly train their sites on high hospital spending in the current tight economic environment.
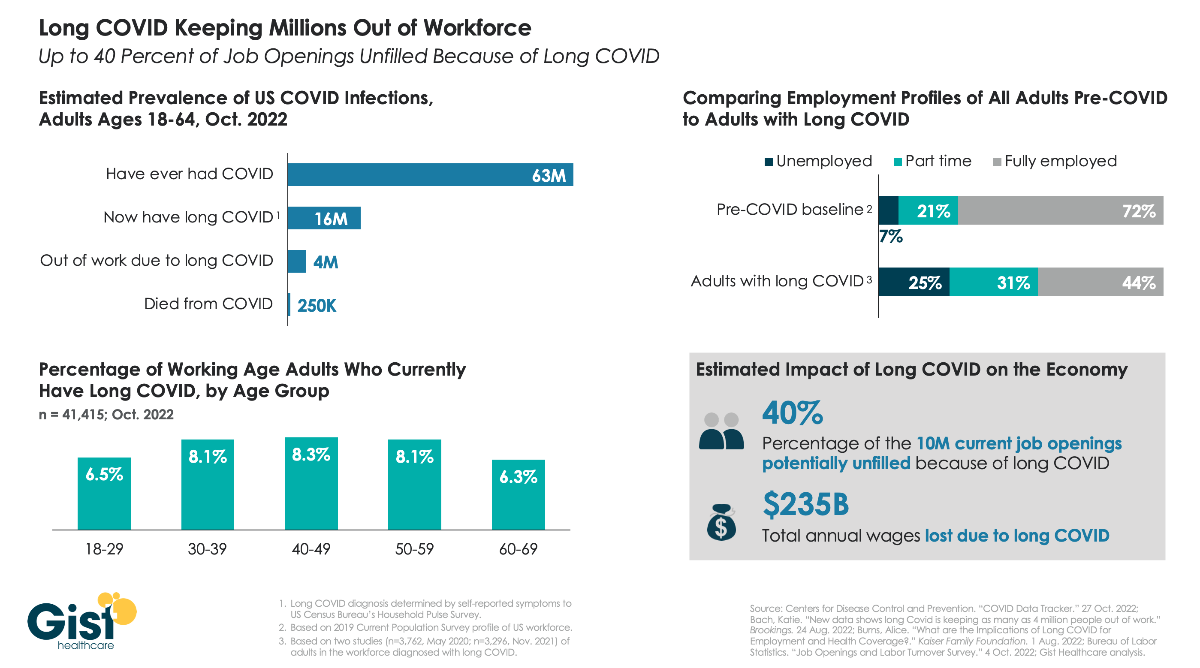
As the nation continues to grapple with the fallout from COVID, one of the greatest unknowns is “long COVID”, the broad range of health problems experienced by a significant number of individuals after contracting the virus. The Centers for Disease Control and Prevention defines long COVID as any post-COVID condition lasting three months or longer.
In the graphic above, we aim to quantify the prevalence of long COVID and its ongoing impact on the US workforce. While estimates for thesenumbers vary, data compiled by Brookings show that COVID infections in roughly one in four working age adults have resulted in long COVID, and up to one in four individuals with long COVID are unable to work due to their lingering health problems. Long COVID is also more prevalent in middle-aged adults, who are often at the peak of their working years. Dealing with symptoms like chronic fatigue and brain fog, long COVID patients are more likely to be unemployed or working reduced hours, compared to a pre-COVID baseline of the general adult population.
While it’s difficult to assess the precise impact on the nation’s current labor shortage, the estimate that 4M working age adults are no longer working because of long COVID equals about 40 percent of the 10M total job openings in August of this year, undoubtedly exacerbating ongoing economic challenges.










_(33114415716).jpg#/media/File:Human_Respiratory_Syncytial_Virus_(RSV)_(33114415716).jpg){kind=link}