
https://www.commonwealthfund.org/chart/2019/aca-fewer-adults-are-uninsured-more-are-underinsured

Senator Elizabeth Warren spoke at length this week about her vision for improving the American health care system, like strengthening the Affordable Care Act and making prescription drugs more affordable. Twice, though, she ignored a question posed to her: Would she support eliminating private health insurance in favor of a single-payer system?
“Affordable health care for every American” is her goal, Ms. Warren said on Bloomberg Television, and there are “different ways we can get there.”
To put it another way: I am not walking into that political trap.
Ms. Warren of Massachusetts and three other liberal presidential candidates support a Medicare for All bill, which would create a single-payer health plan run by the government and increase federal spending by at least $2.5 trillion a year, according to several estimates. But Ms. Warren’s determination to sidestep an essential but deeply controversial issue at the heart of the single-payer model — would people lose the choices offered by private insurance? — illustrated one of the thorniest dilemmas for several Democrats as the 2020 primary gets underway.
Their activist base, inspired by Senator Bernie Sanders of Vermont, believes that the party should unabashedly pursue universal health care, ending private insurance entirely. But polls indicate that the broader electorate, particularly the moderate- and high-income voters who propelled the party’s sweeping suburban gains in the midterms, is uneasy about this “Medicare for all” approach in which many would lose their current insurance options and pay higher taxes.
Senator Kamala Harris of California drew immediate attacks from Republicans this week by taking on the issue that Ms. Warren dodged. Ms. Harris breezily acknowledged in a CNN town hall forum that she would “eliminate all of that,” referring to ending private insurance in a country where almost 60 percent of the population receives coverage through an employer.
Her remark triggered an intraparty debate about an issue that until now had been largely theoretical: A decade after Democrats pushed through the most significant expansion of health care since the Great Society, should they build incrementally on the Affordable Care Act or scrap the insurance sector entirely and create a European-style public program?
Four Democratic presidential candidates — Ms. Harris, Ms. Warren, Senator Kirsten Gillibrand of New York and Senator Cory Booker of New Jersey — are among the co-sponsors of Mr. Sanders’s Medicare for All bill, which would replace the Affordable Care Act with a single government health plan for all Americans. Medicare is the federal program providing health coverage to people 65 and older.
The concept of Medicare for all has become popular with Democrats: 81 percent support it, according to a recent Kaiser poll. Yet voter opposition to surrendering the insurance they are used to led to a backlash over President Barack Obama’s repeated promise that “if you like your plan, you can keep your plan” after it proved false for several million people under his health law. Many Democrats are keenly aware of that backlash, and the 2020 presidential race will be the first where many of the party’s leading candidates will have to explain and defend the meaning of Medicare for all.
For now, as Ms. Warren demonstrated, many candidates do not want to wrestle publicly with the details. After Ms. Harris’s comment, her aides hastened to add that she would also support less sweeping changes to health care; like most other candidates, Ms. Harris declined an interview request. And by Friday, Mr. Booker, hours after announcing his presidential bid, sought to curtail the matter by offering a brisk “no” when asked if he supported eliminating private coverage.
Yet there is one likely 2020 contender who is thrilled to discuss Medicare for all.
Mr. Sanders, in an interview, did not mince words: The only role for private insurance in the system he envisioned would be “cosmetic surgery, you want to get your nose fixed.”
“Every candidate will make his or her own decisions,” Mr. Sanders said, but “if I look at polling and 70 percent of the people support Medicare for All, if a very significant percentage of people think the rich, the very rich, should start paying their fair share of taxes, I think I’d be pretty dumb not to develop policies that capture what the American people want.”
But Michael R. Bloomberg, the former New York City mayor who is considering a 2020 bid on a centrist Democratic platform, said it would be folly to even consider a single-payer system. “To replace the entire private system where companies provide health care for their employees would bankrupt us for a very long time,” Mr. Bloomberg told reporters in New Hampshire on Tuesday.
The Congressional Budget Office has not scored Mr. Sanders’s Medicare for All bill, but a study last year by the Mercatus Center of George Mason University predicted it would increase federal spending by at least $32.6 trillion over the first decade. The cost could be even greater, the study says, if the bill overestimated the projected savings on administrative and drug costs, as well as payments to health care providers.
The divide between Mr. Sanders, a democratic socialist, and Mr. Bloomberg, a Republican-turned-independent-turned-Democrat, reflects the large chasm in a party that has been reshaped by President Trump.
The president’s hard-line nationalism has simultaneously nudged Democrats to the left, emboldening them to pursue unambiguously liberal policies, and drawn independents and moderate Republicans to the party because they cannot abide his incendiary conduct and demagogy on race. These dueling forces have created a growing but ungainly coalition that shares contempt for Mr. Trump but is less unified on policy matters like health care.
And these divisions extend to what is wisest politically.
Liberals argue that the only way to drive up turnout among unlikely voters or win back some of the voters uneasy with Hillary Clinton’s ties to corporate interests is to pursue a bold agenda and elevate issues like Medicare for all.
“Those who run on incremental changes are not the ones who are going to get people excited and get people to turn out,” said Representative Pramila Jayapal of Washington, the co-chair of the Congressional Progressive Caucus.
And by preserving their options, Democrats risk alienating liberal primary voters, some of whom consider support for Medicare for all a litmus test.
“The center is not a good place to be on these policies anymore,” said Mary O’Connor, 61, a substitute teacher and horse farmer in Middleburg, Va., who wants a single-payer system. “I’ll be watching extremely closely, and I will most likely jump on board and volunteer for whoever it is that’s going to be the most forceful for this.”
But moderates believe that most Democratic primary voters are more fixated on defeating Mr. Trump than applying litmus tests — and that terminating employer-sponsored insurance would only frighten the sort of general election voters who are eager to cast out Mr. Trump but do not want to wholly remake the country’s health care system.
“Most of the freshmen who helped take back the House got elected on: ‘We’re going to protect your health insurance even if you have a pre-existing condition,’ not ‘We’re going to take this whole system and throw it out the window,’” said Kenneth Baer, a Democratic strategist.
While polling does show that Medicare for all — a buzz phrase that has lately been applied to everything from single-payer health care to programs that would allow some or all Americans to buy into Medicare or Medicaid — has broad public support, attitudes swing significantly depending on not just the details, but respondents’ age and income.
On the House side, a bill similar in scope to Mr. Sanders’s is under revision and will soon be reintroduced with Ms. Jayapal as the main sponsor. Other Democrats have introduced less expansive “Medicare buy-in” bills, which would preserve the current system but would give certain Americans under 65 the option of paying for Medicare or a new “public option” plan. Another bill would give every state the option of letting residents buy into Medicaid, the government health program for poor Americans.
The buy-in programs would generally cover between 60 and 80 percent of people’s medical costs and would require much less federal spending because enrollees would still pay premiums and not everyone would be eligible. Some proponents, like Senator Jeff Merkley, Democrat of Oregon, have described them as a steppingstone on the way to a full single-payer system; some of the Democrats running for president are co-sponsoring these “Medicare for more” bills as well as Mr. Sanders’s.
Mr. Sanders has suggested options to raise the money needed for his plan, such as a new 7.5 percent payroll tax and a wealth tax on the top 0.1 percent of earners. He has also predicted several trillion dollars in savings over 10 years from eliminating the tax exclusion that employers get on what they pay toward their workers’ insurance premiums, and other tax breaks.
But Robert Blendon, a health policy professor at Harvard who studies public opinion, said it would be wise not to delve into financing details for now.
“The reason it failed in Vermont and Colorado was taxes,” Professor Blendon said, referring to recent efforts to move to a near-universal health care system in those states, which flopped resoundingly because they would have required major tax increases. “But Democratic primary voters will not go deep into asking how these plans will work. What they will say is, ‘Show me you have a principle that health care is a human right.’”
The general election will be a different story, Professor Blendon added. If Ms. Harris were to become the Democratic nominee and keep embracing the idea of ending private coverage, he argued, “she’s going to have terrible problems.”
The difficulty for Democrats, added Ezekiel Emanuel, a former Obama health care adviser, is that many voters look at the health care system the same way they view politics. “They say Congress is terrible but I like my congressman,” as Mr. Emanuel put it.
According to the Gallup poll, 70 percent of Americans with private insurance rate their coverage as “excellent” or “good;” 85 percent say the same about the medical care they receive. The Kaiser poll found that the percentage of Americans who support a national health plan drops by 19 percentage points when people hear that it would eliminate insurance companies or that it would require Americans to pay more in taxes.
Among those who make over $90,000 a year — the sort of voters in the House districts that several Democrats captured in the midterms — those surveyed in the Kaiser poll were particularly wary of an all-government system: 64 percent in this income group said they would oppose a Medicare for all plan that terminated private insurance.
“My constituents are tired of bumper sticker debates about complex issues,” said Representative Lizzie Pannill Fletcher of Texas, a freshman from an affluent Houston district. “We don’t want ideologues in charge.”
In Vermont, where former Gov. Peter Shumlin shelved his ambitious plan for a single-payer system in 2014 after conceding it would require “enormous” new taxes, advocates for universal health care are now resigned to a more incremental approach.
Dr. Deb Richter, a primary care doctor who helped lead the state’s single-payer movement, said that while the Democratic field is “going to have to face the T word,” being upfront about the required tax increases, she now thinks phasing in a government-run system is a better approach.
“There’s ways of doing this that don’t have to happen all at once,” she said, pointing to a push in Vermont to start with universal government coverage for primary care only. “But you need to talk about the end goal: We are aiming for Medicare for all, and this is a way of getting it done.”

In reference pricing — a component of health insurance design — a health care purchaser establishes a maximum payment it will contribute toward covering the price of a drug. It is used when there is a wide variation in the prices for therapeutically similar products. The payment limit is set at the minimum, median, or other point along the range of drug prices within a therapeutic class. If a patient’s physician prescribes a drug with a price at or below the reference limit, the patient pays only a modest copayment. If a more expensive option is selected, he or she pays the copayment plus the full difference between the reference limit and the price of the chosen product.
Reference pricing offers several advantages over the most commonly used insurance designs in the United States, such as annual deductibles and coinsurance, which expose consumers to financial obligations without providing an affordable option or guidance on how to select products offering the best value. To date, however, reference pricing has been applied only by a limited number of purchasers and only to drug classes that feature multiple generic or therapeutically equivalent alternatives. For these therapeutic classes, it can reasonably be assumed that all products work similarly. Purchasers can limit their payments to the level charged for the cheaper products in each class and patients desiring a higher-priced option reasonably can be required to pay the difference themselves. Patients with physician-identified clinical needs for higher-priced options can be granted an exception.
In its efforts to improve the effectiveness and efficiency of pharmaceutical purchasing, the U.S. can learn from Germany, which manages traditional drugs using reference pricing and novel drugs using comparative-effectiveness pricing. Germany has developed evidence-based methods to assess the clinical benefit of new products, establish reference-based payments for drugs that do not offer incremental benefits over existing products, and negotiate new prices for drugs that do offer incremental benefits.1 This approach enjoys considerable social legitimacy as a mechanism for ensuring patient access while moderating payer expenditures.
The health care system in Germany resembles that of the U.S. in several important respects yet differs in others. (See box.) Both feature multiple nongovernmental insurers rather than a single governmental payer, favor negotiation over regulation for determining prices, enjoy declining expenditures for many traditional, nonspecialty drugs but face rising expenditures for novel specialty products, and are embedded in a culture that values patient access to even the most expensive treatments. However, in Germany, the clinical assessment of each new drug is centralized and the negotiation of drug prices is done collectively by the umbrella organization of health insurers, rather than by each insurer individually. This issue brief describes the structure of drug assessment and pricing in Germany and its potential applicability to the U.S. market.2
THE INSTITUTIONAL FRAMEWORK OF PHARMACEUTICAL PRICING IN GERMANY
In Germany, reference pricing falls within an institutional system that features publicly regulated and accountable associations of insurers, physicians, and other stakeholders. Statutory and case law establish the rules governing interactions among these entities, and the Ministry of Health continuously monitors and supports their processes. But the government does not directly assess the comparative clinical benefit of new drugs or negotiate their prices. In this regard, it resembles the U.S. framework more than other European systems where the heavy lifting in pharmaceutical cost control is done directly by governmental payers.
The German institutional framework does differ from its U.S. counterpart in important respects. The organization that assesses the comparative clinical performance of new drugs, the Federal Joint Committee (GBA), consists of representatives of the national insurance, physician, and hospital organizations. Patient advocacy organizations have nonvoting seats on the board. The GBA, in turn, delegates the clinical evaluation of new drugs to a privately governed but publically accountable entity, the Institute for Quality and Efficiency in Health Care (IQWiG). IQWiG bases its evaluations on: dossiers submitted by manufacturers, which include a systematic review of the incremental benefit of the drug; the clinical trials for initial market authorization by the European Medicines Agency, as well as other clinical trials; reports by technology assessment agencies in other nations; and other available evidence. GBA then makes its official assessment of each drug’s contribution based on the IQWiG study, further input from the manufacturers, and follow-on testimony at public meetings.
The GBA assessments are used by the umbrella organization of Sickness Funds, the GKV-SV. The GKV-SV works within a statutory and regulatory framework that assigns it special rights and responsibilities, and interprets its role as negotiating the best prices from the point of view of the health system, and not merely that of its constituent insurers.
In the German pharmaceutical system, new drugs are assessed and priced relative to existing treatments for the same conditions. Drugs that offer additional clinical benefits are paid higher prices; reference pricing is applied to new drugs with clinical performance similar to products already on the market. Comparative-effectiveness pricing applies to new products that perform better than their comparators.
All drugs authorized for market access by the European Medicines Agency (EMA) are immediately available after launch for physicians to prescribe and patients to use. The manufacturer unilaterally sets the new drug’s price at time of launch and is reimbursed in full at that price for the drug’s first year. During this first year, an assessment is conducted of the drug’s comparative clinical safety and efficacy by the Federal Joint Committee (GBA), a self-governing but publicly accountable entity representing associations of nongovernmental insurers (also known as “Sickness Funds”), physicians, and hospitals.
The GBA makes several important decisions regarding the assessment of each drug’s incremental benefit, with input from the Institute for Quality and Efficiency in Healthcare (IQWiG), the pharmaceutical manufacturer, relevant medical associations, patient advocacy organizations, and other interested entities. First and often most importantly, GBA decides which drug will be used as the comparator against which the new product is to be assessed; a drug treating multiple indications may have multiple comparators. If the new drug is found to offer incremental benefits, its price will be negotiated upwards from the comparator’s price, and so the manufacturer has an interest in having the GBA select a high-priced comparator. However, if GBA picks as the comparator a drug with high price but also high efficacy, the new drug faces a more difficult challenge in demonstrating incremental benefit. A finding of no incremental benefit leads to the drug being assigned to a therapeutic class subject to reference pricing. All products are reimbursed at a level based on the lowest prices charged within the class, if it falls within a therapeutic class for which reference prices have been established. If the new drug is found not to offer an incremental benefit but also does not fall into a reference-priced therapeutic class, its price is subject to negotiation with the proviso that the negotiated price not exceed that of its comparator drug.
Second, the GBA chooses the metrics that will assess the new drug’s benefit. These metrics may differ from those used by the EMA, the European equivalent of the U.S. Food and Drug Administration (FDA), in its review of the drug for initial market authorization and for which the manufacturer has conducted clinical trials. In some cases, GBA has rejected metrics acceptable to EMA, such as “progression free survival” for cancer drugs, as it deems them not relevant to the patient’s quality of life. Progression free survival indicates how many months the patient survives posttreatment without an increase in the size of his or her tumors. This metric is correlated with the more important overall survival metric, which indicates the number of months the patient remains alive posttreatment, but is often not correlated with patient quality of life. In other cases, GBA has required that pharmaceutical firms provide metrics that EMA does not require, principally quality-of-life indicators such as change in pain and nausea.
The GBA delegates the clinical evaluation of the new drug to IQWiG,3 which considers the portfolio of evidence used for market authorization by EMA plus other studies conducted by the manufacturer. The final assessment of the drug’s benefit then is decided by the GBA. Drugs can be judged by the GBA to offer a major, substantial, minor, positive but nonquantifiable, or no incremental benefit, relative to the comparator treatment. The nonquantifiable benefit is used when the drug is considered likely to offer incremental benefit but lacks sufficient evidence for a confident judgment of the scale. Orphan drugs, which often have no direct comparator and for which the clinical evidence may be based on very small patient samples, usually are awarded a nonquantifiable benefit. The GBA also evaluates the strength of the available evidence (weak, moderate, or strong). The clinical benefit of a drug can be reassessed by GBA in response to changes in the available evidence, sometimes triggering a renegotiation of the price.
If the GBA considers a drug not to offer an incremental benefit over existing treatments, it usually assigns it to one of the therapeutic classes covered by reference pricing. Manufacturers are permitted to set whichever price they feel is appropriate for drugs falling into these classes, but the umbrella organization of health insurers (GKV–SV) establishes a limit to what individual insurers will contribute toward payment. The GKV–SV sets its payment limit near the 30th percentile in the distribution of prices within each therapeutic class, high enough to ensure that patients have more than one choice but low enough to ensure that the payer is not responsible for paying the highest prices within the class. Most generic drugs fall into the reference pricing system. Approximately 34 percent of drugs, 80 percent of prescriptions, and 33 percent of drug spending in Germany is for drugs subject to reference pricing.4
Patients must pay out of pocket the difference between the price set by the manufacturer and the reference-based reimbursement limit set by the purchaser organization. Many patients are unwilling to contribute out of pocket and prefer drugs priced below the reference limit and their physicians will prescribe drugs at or below the limit. Of products subject to reference pricing, approximately 84 percent are priced by their manufacturers at or below the reference price limit and therefore not subject to additional cost-sharing.5 These products make up 92 percent of all prescriptions made for reference-priced drugs. Manufacturers can submit new prices up to twice a month for drugs in the reference pricing system. The umbrella organization of insurance firms is required to update the therapeutic classes every quarter and the payment limits at least annually. Manufacturers are permitted to lower their prices to the reference limit to avoid the otherwise inevitable reduction in sales volume; many do.
For drugs included in the reference pricing system, patients may be required to pay additional copayments, depending on which drug they select in consultation with their physicians. Patients selecting a drug priced above the reference maximum for their class contribute a copayment plus the difference between their drug’s price and the reference maximum. These extra copayments do not count toward the patients’ annual out-of-pocket cost-sharing maximum. However, the extra copayments are modest, since most of the drugs included in the reference pricing system are older, generic medications with typically low prices. For drugs not included in the reference pricing system, German health insurers require patients to pay the cost-sharing amount only.
Aside from the requirement that patients pay the difference between the reference limit and the full price of a product, which applies only in contexts where the patient can choose a low-priced option, Germany places tight limits on patients’ out-of-pocket financial responsibilities. The statutory copayment ranges from a minimum of EUR 5 to a maximum of EUR 10 per prescription, up to an annual out-of-pocket maximum (for all health care services) of 1 percent of gross income for people with chronic diseases and 2 percent for others. Approximately one-quarter of enrollees also have complementary private insurance, which covers these cost-sharing requirements.6
If a new drug is judged by the GBA to offer an incremental benefit over existing treatments, it is referred to the GKV–SV for price negotiations with the manufacturer. The insurer umbrella association uses the GBA’s assessment of clinical benefit, as well as the prices of the comparator drug, therapeutically similar medications, and prices charged in other European nations to negotiate a discount off the new drug’s launch price.
Some drugs are judged by the GBA not to offer an incremental benefit yet do not fall into an existing reference-priced therapeutic class, as there must be at least three therapeutically equivalent drugs to constitute a class for reference pricing. These drugs also have their prices negotiated between the manufacturer and the insurer association, but with the proviso that the price of the new drug cannot exceed that of the comparator product chosen by the GBA.
If negotiations between the insurer umbrella association and the drug manufacturer do not conclude with a price agreeable to both sides, the drug is referred to arbitration. In this process, a three-person panel selected by the manufacturer, the insurance organization, and the GBA assesses the evidence and renders a decision. Through the end of 2017 one of five (35 of 186) new drugs assessed by the GBA received a final price through arbitration rather than negotiation; for another 24, the negotiating parties reached an agreement after an arbitration process had been initiated.7
If a manufacturer cannot obtain an acceptable price either through negotiation or arbitration, it can withdraw its product from the market. Between 2011 and 2017, 148 drugs were subjected to comparative-effectiveness assessment and had their prices negotiated by the insurers and manufacturers. Of these, 29 were removed by the manufacturer from the German market by 2018.8 For 12 of these, the manufacturer chose to withdraw the product immediately following the results of the GBA evaluation — this is known as “opting out” of the pricing process. In 16 cases, drugs were withdrawn in reaction to the determined price, mainly through arbitration, and one was withdrawn because its manufacturer went bankrupt.9
The German system uses modest levels of cost-sharing as an instrument to influence consumer choices for drugs with therapeutically equivalent alternatives. However, it does not apply cost-sharing to new drugs that lack alternatives. Comparative-effectiveness pricing is used for new specialty medications that offer clinical benefits over existing treatments. Manufacturers are free to set the prices of their products, but insurers will not pay more for a new drug than for its comparators unless it offers an additional clinical benefit. For drugs covered by reference pricing, the insurers’ payment maximum is set at a level that ensures sufficient choices of low-priced options. These models offer an alternative to the U.S. system of tiered formularies.
In the United States, the level of cost-sharing and the resulting financial burden on patients is high, especially for patients with complex medical conditions. U.S. payers often impose modest copayments on low-cost drugs with many direct substitutes but onerous coinsurance on high-cost drugs with few substitutes. Coinsurance does not point the patient toward the most cost-effective drug choices. In contrast, insurance designs built on reference pricing identify drugs that are priced below the insurer’s payment maximum and require only minimal cost-sharing.
Can the State of California Afford to Provide Universal Health Care Coverage?
Perhaps no issue looms larger on both the state and national political stage than the question of universal health care coverage.
U.S. Presidential hopeful Kamala Harris (D) sent a shockwave through the national health care debate on Monday Jan. 28th by nonchalantly stating that she would eliminate private insurers as a necessary part of implementing “Medicare-for-all,” according to a CNN report.
Due to a firestorm of attention, most of it negative, the next day the Harris campaign walked back the previous day’s remarks in large part by stating that the candidate would also be open to more moderate health reform plans, which would preserve the private industry, according to the CNN report.
Newly elected California Governor Gavin Newsom (D) campaigned on the issue of single-payer health care and on his very first day in office unveiled a comprehensive package of reform proposals aimed at expanding state health care coverage subsidies and lowering its costs, which includes extending Medi-Cal to undocumented immigrants, according to a report by the LA Times.
In an interview, Gov. Newsom told the LA Times “These are not just symbolic gestures…We’re hoping to ignite a new conversation. It’s a moral imperative, not just economic,” states the LA Time report.
But as many experts, including Gov. Newsom, have pointed out, big systemic reform to the system, such as a move to a single-payer health system, would require the unlikely support of the Trump Administration.
Newsom has done a good job of tempering expectations for single-payer health care and his proposed coverage expansions and prescription cost controls demonstrate to the his supporters and the public that he is serious about expanding coverage as well containing costs.
But the 800-pound guerilla in the universal health care conversation is where will all the money come from to provide guaranteed government financed coverage to every Californian and everyone who likely to come to California once universal health care is guaranteed by the state?
“Where do you get the extra money? This is the whole question…I don’t even get it…how do you do that?,” said former California Governor Jerry Brown (D) following a universal healthcare discussion in Washington, D.C. in a 2017 interview with the LA Times.
At the time, Gov. Brown pointed out that the overall cost of medical care in California is equal to 18% of the state’s gross domestic product, which would be about $450 billion.
“You take a problem and say I’m going to solve it by something that’s an even bigger problem, which makes no sense,” then Governor Brown said at the time, according to the LA Times report.
Gov. Newsom developed some questionable rhetoric during the 2018 campaign, where he said that the State of California cannot afford not to move to a single-payer system because health care has become such a big expense in the state.
It appears that one of the major points of disagreement between former Gov. Brown and now Governor Gavin Newsom is the question of whether the State of California can afford to move to a universal health care system, specifically a single-payer system?
More recently, other high-profile liberal Democrats have come out against single-payer health care with former Mayor of New York City and billionaire Michael Bloomberg stating that Medicare-for-all “would bankrupt us for a very long time,” according to a CNN report.
“I think we could never afford that,” Bloomberg said, addressing pin factory employees in New Hampshire. “We are talking about trillions of dollars.”
“I think you could have Medicare-for-all people who are uncovered, but that’s a smaller group,” Bloomberg said.
“But to replace the entire private system where companies provide health care for their employees would bankrupt us for a very long time,” said Bloomberg according to the CNN report, which noted that Bloomberg made the comments in response to Sen. Kamala Harris calling for an end to the private health care market.
So what does all this mean for the current universal health care debate in California?
It means that California Democrats might want to heed the advice of two of the county’s most prominent liberal Democrats—former Gov. Jerry Brown and Michael Bloomberg—and proceed with great caution regarding the feasibility of California going it alone on universal health care.
There is no question that the state could choose to enact a single-payer or Obamacare-type universal health care system, but the million dollar question, or trillion dollar question rather in this case, is would such a system work and be fiscally sustainable over the long-term?
As a long-time analyst of fiscal issues in California, I believe that former Gov. Jerry Brown and Michael Bloomberg are correct to point out the major challenges and risks of moving to a universal health care system—both at the state level and the federal level.

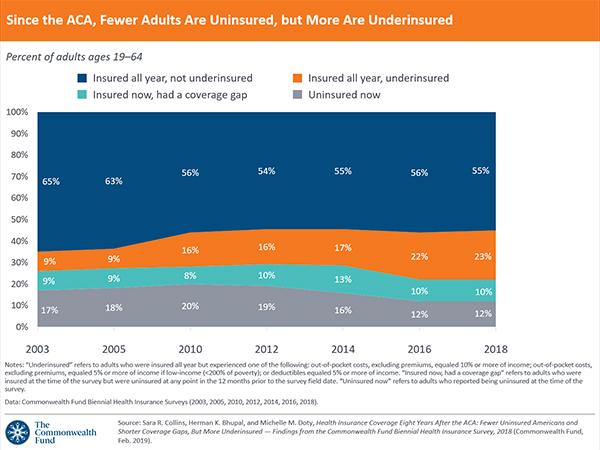
The Affordable Care Act’s insurance exchanges have been the law’s headline feature over the past eight years, but the law’s Medicaid expansion has covered just as many people, and its rolls are more likely to grow under the Trump administration.
Driving the news: Roughly 8.8% of Americans were uninsured last year, according to new Census figures released yesterday — essentially unchanged from 2016. That means the Trump administration has not kept the ACA’s coverage gains going, nor has it successfully rolled them back — at least, not yet.

People Googling for ACA coverage often found results that were actually trying to sell them skimpier short-term health plans, according to a report from Robert Wood Johnson Foundation and the Urban Institute.
Why it matters: Consumer confusion is one of the things regulators worried about most when the Trump administration expanded access to “short-term” coverage.
Details: Researchers Googled terms including “cheap health insurance” and “Obamacare plans” and looked at the first 4 results — which are usually ads.

Democratic presidential contender Sen. Kamala Harris wants to “move on” from the current healthcare system in favor of a plan that would roll everyone in the U.S. onto a government plan known as “Medicare for all,” doing away with private health insurance.
As the California Democrat and others in her party make their case, however, they will face considerable opposition not only in the insurance industry, but across the healthcare sector, which would see massive upheaval from the plan. And polling suggests that the public, roughly half of which relies on private insurance, isn’t quite on board.
Drug companies, insurers, doctors, and hospitals have united in recent months to fight national government healthcare. One healthcare industry group, called the Partnership for America’s Health Care Future, has launched a five-figure digital ad campaign arguing that “Medicare for all” would cause massive disruption, higher taxes, lower quality care, and less choice for patients. It plans to spend six figures bashing “Medicare for all” over the course of 2019.
“Whether it’s called Medicare for all, single payer, or a public option, one-size-fits-all healthcare will mean all Americans have less choice and control over the doctors, treatments, and coverage,” said Lauren Crawford Shaver, the group’s executive director.
Other candidates for the Democratic nomination, such as Sens. Elizabeth Warren of Massachusetts and Kirsten Gillibrand of New York, are, like Harris, co-sponsors of the Medicare for All Act, legislation led by Sen. Bernie Sanders, I-Vt. Although it has “Medicare” in the name, the bill would go much further than current Medicare, which covers adults 65 and older and people with disabilities. It would pay for emergency surgery, prescription drugs, mental healthcare, and eye care without a copay.
Children would be enrolled in the government plan soon after the the bill’s passage, and the rest would be gradually phased in after four years. This would mean that roughly half of the U.S. population, the 177 million people in the U.S. covered by private health insurance mostly through work, would be moved onto a government plan. Employers would pay higher taxes rather than pay for private plans.
In defending the need for a government system, Sanders has blasted insurance companies, saying upon unveiling the bill that they “make billions of dollars in profits and make industry CEOs extremely wealthy.”
But healthcare providers, not just insurers, benefit from the current fragmented system, in which insurance is purchased by employers, the government, and individuals. They charge private insurers more to make up for the gap left by patients who are uninsured or are on government programs, which pay less for their services.
If all privately insured individuals were to have Medicare instead, and if it were to pay the same rates it does now, then doctors and hospitals would see big losses caring for patients who moved from private coverage to the government plan. Healthcare providers have said that if taxes don’t go up to pay for the difference, then doctors and hospitals will face pay cuts and layoffs, leading to facility closures and long lines for care.
Hospitals serve as the main employer in many communities. For patients, that would mean losing not only a healthcare plan they might be satisfied with, but also doctors they worked with for years or hospitals they relied on in their communities.
The Medicare for All Act has not been scored by the Congressional Budget Office, but analyses from the Mercatus Center at George Mason University and the left-leaning Urban Institute found it would raise government spending over a decade by $32.6 trillion.
Overall healthcare spending, though, would actually fall by $2 trillion, as private spending on healthcare would collapse. The cut would be achieved, however, through paying 40 percent less to providers than what they were getting from private insurance.
Another obstacle to “Medicare for all” is the fact that the public isn’t fully convinced by the idea of nixing private insurance, a recent poll from the Kaiser Family Foundation shows. Initially, 56 percent of those polled favored the Medicare for All Act, but then when they learned it would do away with private health insurance, the support fell to 37 percent.
Candidates are going to face pushback within their party. House Speaker Nancy Pelosi and other Democratic leaders have not embraced government healthcare, instead pushing for adding funding to Obamacare.
But proponents of allowing the government to have a more extensive role in healthcare point out that waste is prevalent in the current system. Patients receive unnecessary medical care, such as repeated tests or surgeries that either don’t make them healthier or even make them worse.
These proponents agree with Harris that health insurance companies are unnecessary. Wendell Potter, an advocate of a government-financed healthcare system and president of the Business Initiative for Health Policy, said in a statement that polling results show the healthcare industry’s misinformation campaign to spread “fear, uncertainty, and doubt” was effective. He said that commercial health insurance companies don’t have an incentive to lower healthcare costs and make sure patients can access care.
Potter, a former health insurance executive, described how the information campaign worked, saying the goal was to “make people believe that private health insurance companies were a necessary part of the healthcare system, and to scare them into thinking that a ‘Medicare for all’ system was expensive and impractical, and that it would cause a significant drop off in the quality of care.”
Dems hit GOP on pre-existing conditions at panel’s first policy hearing

The powerful House Ways and Means Committee used its first policy hearing of the new Congress to hammer Republicans on pre-existing conditions, an issue that helped propel Democrats into the majority during the 2018 midterm elections.
Democratic panel members highlighted actions by the Trump administration that they argue have hurt people with pre-existing conditions, like the expansion of non-ObamaCare plans that could draw healthy people from the markets, raising premiums for those left behind.
The administration has expanded access to association and short-term health plans, which cost less than ObamaCare plans but cover fewer services. Republicans say they provide an off-ramp for consumers who can’t afford ObamaCare plans.
The witness invited by Republicans, Rob Robertson with the Nebraska Farm Bureau, said its newly developed association health plan “meets the needs of our members,” who can’t afford ObamaCare plans.
“We’re in this for the long term,” he told lawmakers. “We want to reduce costs, and the costs in the individual market are very, very high.”
ObamaCare’s popular consumer protections became the centerpiece of the November midterms after 20 Republican-led states sued to overturn the 2010 health care law, known as the Affordable Care Act (ACA).
Democrats tied congressional Republicans to the lawsuit after the Trump administration declined to defend ObamaCare and argued that those protections are unconstitutional.
Republicans say there are different ways to cover people with pre-existing conditions, like high-risk pools, which were banned after ObamaCare was implemented. Some pools had caps on coverage and long-waiting lists.
GOP committee members called Tuesday’s hearing political theatre, arguing they also support pre-existing protections but want to lower ObamaCare’s costs.
“Everyone up here wants protections for people with pre-existing conditions. Always have, always will,” said Rep. Devin Nunes (R-Calif.), ranking member of the health subcommittee. “We should be careful that we’re not stoking fear that someone is going to lose their health insurance. We have a responsibility to come up with a better health care system because ObamaCare is not the solution.”
Democrats on Tuesday said the GOP proposals aren’t serious.
Republicans have “political amnesia” and have “forgotten what it was like before the ACA,” said Rep. Lloyd Doggett (D-Texas), chairman of the health subcommittee. “Those with a diagnosis of a serious disease would also get a diagnosis of financial ruin. There were no protections for them before the ACA.”
Some Democratic panel members appealed to the emotional side of the health care debate, with one lawmaker announcing her cancer diagnosis at the hearing.
“This is a cancer I will live with for the rest of my life, but, because of my high-quality healthcare and insurance coverage, it is not a cancer I will die from,” said Rep. Gwen Moore (D-Wis.), 67.
Tensions ran high at times during Tuesday’s hearing, with members re-litigating the 2010 passage of ObamaCare and repeated GOP efforts to repeal it.
“Not one Republican up here supports pre-existing protections for the American people,” said Rep. Brian Higgins (D-N.Y.), who at times pounded his fist on the dais.
That drew a testy response from Rep. Tom Reed (R-Pa.), who said Republicans “heard the voices and the fear” from voters in the 2018 midterms when “this issue became the centerpiece.”
“We listened to this American people, as Republicans,” he said.

The pace of change in healthcare is not slowing down; in fact, it is accelerating. Healthcare organizations that are most successful in 2019 will know what challenges and changes are coming down the pipeline, and they will prepare accordingly.
To help ensure you don’t get left behind, we’ve assembled the top six challenges the industry will face in 2019.
1. Shifting the focus from payment reform to delivery reform. For the past few years, C-suite leaders at healthcare organizations have been focused on navigating healthcare payment reform—attempting to preserve, improve, and maintain revenue. Amidst those efforts, delivery reform has sometimes taken a back seat.
That will need to change in 2019. Organizations that are the most successful will focus more on patient care than revenue, and they will see improved outcomes and reduced costs as a result.
Many organizations are already exploring delivery reform with initiatives that focus on:
In 2019, however, they will need to bring all of these initiatives together to implement sustainable improvements in how healthcare is delivered.
An added bonus? Organizations that accomplish this will see enhanced revenue streams as value-based reimbursement accelerates.
2. Wrestling with the evolving healthcare consumer. Healthcare consumers are demanding more convenient and more affordable care options. They expect the same level of customer service they receive from other retailers—from cost-estimation tools and online appointment booking to personalized interactions and fast and easy communication options such as text messaging and live chats.
Organizations that don’t deliver on these expectations will have a difficult time retaining patients and attracting new ones.
That’s not the only consumer-related challenge healthcare organizations will face. In 2019, millennials (between the ages of 23 and 38), will make up nearly a quarter of the U.S. population.
This generation doesn’t value physician-patient relationships as highly as previous generations. In fact, nearly half of them do not have a personal relationship with their physician, according to a 2015 report by Salesforce.
Finding ways to maintain or increase the level of humanity and interaction with millennials will be a key challenge in 2019. Patient navigator solutions and other engagement tools will be critical to an organization’s success.
3. Clinician shortages. Physician and nurse shortages will continue to intensify in 2019, creating significant operational and financial challenges for healthcare organizations.
The most recent numbers from the Association of American Medical Colleges predict a shortage of up to 120,000 physicians by 2030. On the nursing side, the Bureau of Labor Statistics projects a need for 649,100 replacement nurses by 2024.
The implications of the shortages, combined with the fact that healthcare organizations face a number of new challenges in the coming years, are many. Fewer clinicians can lead to burnout, medical errors, poorer quality, and lower patient satisfaction.
Healthcare organizations that thrive amidst the shortages will find new ways to scale and leverage technology to streamline work flows and improve efficiencies.
4. Living with EHR choices. Despite the hype and hopes surrounding EHRs, many organizations have found that they are failing to deliver on their expectations.
A recent Sage Growth Partners survey found that 64 percent of healthcare executives say EHRs have failed to deliver better population health management tools, and a large majority of providers are seeking third-party solutions outside their EHR for value-based care.
The survey of 100 executives also found that less than 25% believe their EHRs can deliver on core KLAS criteria for value.
As we recently told Managed Healthcare Executive, that statistic is striking, considering how important value-based care is and will continue to be to the industry.
Despite the dissatisfaction surrounding EHRs, switching EHRs may be a big mistake for healthcare organizations. A recent Black Book survey found 47% of all health systems who replaced their EHRs are in the red over their replacements. A whopping 95% said they regret the decision to change systems.
Hospitals and physician may not be entirely happy with their EHR choices, but the best course may be to stick with their system. Highly successful hospitals and health systems will find ways to optimize workflow and patient care which may involve additional IT investments and best of breed investment approaches, rather than keeping all of the proverbial eggs in the EHR basket.
5. Dealing with nontraditional entrants and disruptors. In 2018, several new entrants entered and/or broadened their reach into healthcare.
Amazon acquired online pharmacy retailer PillPack, and partnered with JPMorgan Chase and Berkshire Hathaway to create a new healthcare partnership for their employees. Early in 2018, Apple announced it was integrating EHRs onto the iPhone and Apple watch, and recently, Google hired Geisinger Health CEO David Feinberg for a newly created role, head of the company’s many healthcare initiatives.
New partnerships have also arisen between traditional healthcare entities that could result in significant healthcare delivery changes. Cigna and Express Scripts received the go-ahead from the DOJ for their merger in September, and CVS and Aetna formally announced the completion of their $70 billion merger November 28.
Read more about the top two ways the CVS-Aetna merger could change healthcare.
All of these new industry disruptors and mergers will impact healthcare organizations, likely creating new competition, disrupting traditional healthcare delivery mechanisms, creating price transparency and pressures, and fostering higher expectations from consumers in 2019. Keeping an eye on these potential disrupters will be important to ensuring sustained success in the long term.
6. Turning innovation into an opportunity. From new diagnostic tests and machines to new devices and drug therapies—the past few years in healthcare have seen exciting and lifesaving developments for many patients. But these new devices and treatment approaches come with a cost.
One of biggest 2018 developments that best exemplifies the challenge between innovation and cost is CAR T-cell therapy. This new cancer treatment is already saving lives, but it racks up to between $373,000 and $475,000 per treatment. When potential side effects and adverse events are accounted for, costs can reach more than $1 million per patient.
Finding the best way to incorporate new treatments like this one, while balancing outcomes, cost, and healthcare consumer demands, will be a top challenge for healthcare organizations in 2019.
