An investigative piece in the Wall Street Journal, written by Mark Maremont, Danny Dougherty, and Anna Wilde Mathews, gives an eye-popping look at how UnitedHealth Group is turning diagnosis-driven billing into a high-stakes game in the conglomerate’s Medicare Advantage business.
As The Journal reported, UnitedHealth has taken a unique approach to Medicare Advantage:
directly employing thousands of doctors and arming them with software that generates diagnosis checklists before they even see patients. Former UnitedHealth physicians described how these suggested diagnoses — often obscure or irrelevant — weren’t optional. To move on to their next patient, doctors were forced to confirm, deny, or defer each proposed diagnosis.
One Oregon physician, Dr. Nicholas Jones, said UnitedHealth frequently pushed conditions so rare – like secondary hyperaldosteronism – he had to Google them. And this wasn’t limited to minor conditions.
Sickness scores for UnitedHealth’s Medicare Advantage patients jumped an average of 55% in their first year of enrollment in one of the company’s health plans compared to a mere 7% rise for patients who stayed in traditional Medicare. As the Journal noted, that’s the kind of jump you’d expect if everyone suddenly developed HIV and breast cancer.
The implications? More diagnoses mean higher “sickness scores,” which translate to billions in extra payments from Medicare. The Journal found that UnitedHealth’s practices generated an additional $4.6 billion from 2019 to 2022 compared to what it would have received if those scores had matched industry averages.
Citing fewer hospitalizations, UnitedHealth insists these practices improve patient outcomes and disease management, but the incentives to inflate diagnoses raise serious questions.
In the piece, you’ll meet Chris Henretta, a UnitedHealth Medicare Advantage “member” who lives in Florida. His doctor diagnosed him as morbidly obese, even though he’s a lifelong weightlifter and doesn’t meet the BMI threshold. “I began to suspect my doctor may have a financial incentive to portray people as higher risk,” Henretta said. The article pointed out that such a diagnosis can trigger an extra $2,400 in Medicare payments annually.
UnitedHealth’s system isn’t just about inflating diagnoses — it’s about turning them into profit centers.
The Journal reported that internal documents revealed that doctors could earn bonuses of up to $30,000 annually for engaging with the diagnosis system. Nurses tasked with “finding” new diagnoses were paid $250 per patient visit.
UnitedHealth has countered by saying these practices reflect its commitment to diagnosing and treating diseases early. But the Journal said many doctors felt pressure to play along.
Dr. Emilie Scott, a former UnitedHealth physician, called the system a money machine: “It’s not about taking care of the patient. It’s about how you get the money to flow.”
For patients and taxpayers, this system poses tough questions. Traditional Medicare patients treated by UnitedHealth doctors didn’t see the same inflation in sickness scores, which underscores how Medicare Advantage’s payment system incentivizes diagnose gaming.
What’s clear is that Medicare Advantage — and UnitedHealth’s dominant role in it — needs much closer scrutiny.
As The Journal reporters wrote, the Centers for Medicare and Medicaid Services is studying these relationships. But real change will require policymakers and the public to confront the deeper flaws in how Medicare Advantage is structured.
Be sure to dive into the original Wall Street Journal article for the full story. The fantastic graphs and photography alone are worth your time, and the detailed reporting provides invaluable insights into how one company’s profit strategies impact us all.
Regular readers know I’ve long been curious about the forces driving one essential question in healthcare today:
Why is it so hard to run a hospital now? One area worth exploring is the interplay between the healthcare system and our nation’s changing demographics.
Baby Boomers have been displaced as the largest generation of adults in America.Millennialsnow hold that position, and Gen Z will likely outnumber Baby Boomers in the workplace sometime this year. Our nation is rapidly diversifying, as more than two-fifths of Americans identify as people of color.
It’s not just a matter of who we are as a nation that’s changing; how we live is evolving, too. The number of 40-year-olds who’ve never been married reached record highs in 2022, according to the Pew Research Center, dovetailing with a steadily growing trend since 1970 toward single living.
The U.S. Census published a report earlier this year showing that nearly 29% of American households include only one person. Further, the U.S. fertility rate is at an all-time low — and, according to a Pew survey, may not recover, given that 47% of those under 50 said they were unlikely to have children. That’s an increase of 10 percentage points since 2018.
The effects of this are starting to shape our broader culture. Solo living has been cited as a contributing factor to the housing crisis, and we’re starting to hear more about how people are grappling with the practical implications of retiring while living alone. This column in The New York Times is just one example.
As for the potential health effects of living alone, in 2023, U.S. Surgeon General Vivek Murthy raised an alarm with a report documenting the negative effects of social isolation on individual and public health. Murthy outlined a host of risks, including cardiovascular disease, hypertension, diabetes and increased susceptibility to infectious disease. Mental health is a major concern. A 2024 study published in National Health Statistics Reports found that people who live alone were more likely to be depressed, particularly if they lacked social or emotional support.
All of this adds up to an increasing burden on the U.S. healthcare system.
As providers who care for the socially isolated already know, it’s impossible to operate as usual if a patient lacks family support. Hospitals and the traditional American family structure are fundamentally intertwined. When family support is not available for a medical emergency, then the entire hospital episode becomes more fragile. Patient discharge procedures assume someone is available at home to help with care, assist in transporting patients for follow-up visits, and engage with the business office around billing and insurance.
Without this family safety net, the potential for readmission rises, harming patient outcomes, increasing costs and putting quality ratings at risk. The rise in younger people living alone also raises further financial implications, given that about 45% of Americans access health insurance through employer-sponsored programs. If someone living alone becomes too sick to work, patients may be less able to pay for care when they need it most.
This is just another in a long list of challenging hospital operational dilemmas. How best to respond to such profound change in the American demographic landscape? The right strategy may be to re-think consumer segmentation.
Consumer segmentation has become very popular at the clinical product level, but perhaps the next level of service segmentation is not among disease types but based on demographic characteristics.
As an increasing portion of the American population has less family support to navigate a hospital stay or chronic illness, it will become more important to identify these patients and determine which new and enhanced services need to be provided to them by the hospital. Social work programs will need to be more robust, and health systems should invest in community partnerships to help bridge the resource gap. But the wide-ranging nature of patients’ practical needs will likely require healthcare leaders to think creatively.
Consider the scope:
Care coordinators: Particularly for patients with complex conditions, it may be beneficial to designate a care coordinator to oversee healthcare planning.
Home health care: Without family members to help with day-to-day care, more nurses and aides will be needed to provide healthcare at home as well as help with day-to-day living. For patients with less demanding healthcare needs, adult day care may be useful.
Medication management: Patients need to understand how to take their medications, watch for potential side effects and interactions, and develop a system to make sure they take them on time. Further, they may need help navigating the pharmacy, either in getting prescriptions filled or with financial assistance programs.
Meal delivery: Nutrition is vital to a patient’s recovery, and ensuring patients have access to healthy options can help to reduce the likelihood of readmission.
Personal emergency response systems: Patients may need devices to call for help during an emergency as well as medical bracelets or other methods for communicating important information to first responders.
Housekeeping assistance: Hospitals may need to help connect patients with resources to maintain clean, safe homes.
Volunteer companions: While volunteer companions usually help elderly patients with social interaction and basic needs, it may be necessary to develop programs that target a wider range of ages.
Transportation services: Patients need help getting to and from follow-up visits.
Telehealth: Remote care will become increasingly important. Clinical services should consider whether care plans could be adjusted to reduce the number of in-person visits.
Beyond targeting resources, consumer segmentation also offers an opportunity to communicate with patients in a more effective and personalized way. This sort of engagement fosters trust and increases loyalty that’s particularly important, given the intimate nature of healthcare.
It’s long been true that the stronger the family system, the better off hospitals are. But as the concept of the American family shifts, and in this case, unwinds, healthcare leaders need to be attuned to new demands—and nimble enough to meet them. This requires making the most of the information you have today to plan for tomorrow.
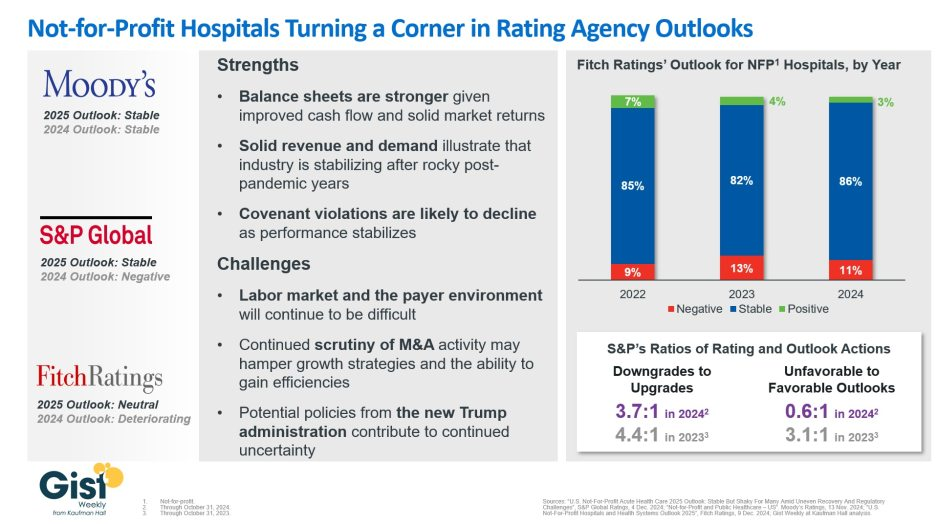
In late 2023, S&P Global and Fitch Ratings viewed the not-for-profit (NFP) hospital sector as negative or deteriorating, reflecting the difficult financial position many were in following the pandemic.
In recent weeks, S&P and Fitch upgraded their 2025 sector outlook for NFP hospitals to stable and neutral respectively, joining Moody’s Ratings, which held stable from last year.
This week’s graphic illustrates the rating agencies’ latest views on NFP hospitals, which point to a promising but uneven recovery for the industry.
Overall, the reports detail that stronger balance sheets, solid revenues, and improved demand have reduced the likelihood of covenant violations and strengthened NFP hospitals’ positions.
However, challenges persist that could impede further progress. The labor market, payer environment, antitrust enforcement, and a new administration all present complications for the continued recovery of NFP hospitals. Nonetheless, the reports indicate significant improvement for the industry since the post-pandemic ratings downturn.
Fitch’s report noted that the share of NFP hospitals with a stable outlook has reached a three-year high. Meanwhile, S&P reported that there are now almost twice as many NFP hospitals with favorable outlooks compared to unfavorable ones, a dramatic flip from 2023, which had a 3.1:1 ratio of unfavorable to favorable outlooks.
These ratings changes reflect the hard work put in by NFP hospitals across the country to improve their financial performance and find new ways to serve their communities sustainably.
However, the recovery remains “shaky” and incomplete, and hospitals still face a long road ahead as they reconfigure to a new normal.
With the onset of the pandemic in March 2020, states were required to provide continuous enrollment for Medicaid and Children’s Health Insurance Program (CHIP) beneficiaries in exchange for enhanced federal funding. This led to immense growth in Medicaid rolls that states could not begin to unwind until April 2023.
This week’s graphic illustrates the outcomes of Medicaid redeterminations—a process which most states completed by August 2024—and provides a comprehensive coverage update.
As this undertaking nears completion, most beneficiaries have had their Medicaid coverage renewed during redeterminations. Around 30% of recipients, or about 25M beneficiaries, lost Medicaid coverage. Nearly 70% of these cuts were made for procedural reasons, such as state agencies not processing beneficiaries’ documents before their cases closed or beneficiaries never receiving the renewal notices.
Despite significant nationwide reductions, 8M more people were enrolled in Medicaid and CHIP in August 2024 than just before continuous enrollment began in February 2020.
Throughout continuous enrollment, an elevated share in Medicaid and a lower uninsured rate were the most notable differences to a coverage landscape that has otherwise remained largely stable.
Somewhat surprisingly, initial evidence suggests that the net effect of continuous enrollment and subsequent Medicaid redeterminations equaled out, and many former recipients have gained coverage elsewhere.
While the national uninsured rate increased to 8.2% in Q1 2024 following a record low in 2023, the uninsured rate remains lower than it was in 2019.
You have three days left, if you got suckered in by those omnipresent ads for Medicare Advantage and left regular Medicare for the siren song of cheaper coverage, “free” vision, hearing, or dental, or even “free” money to buy groceries or rides to the doc.
The open enrollment period for real Medicare closes at the end of the day Saturday, December 7th; after that, you’re locked into the Medicare Advantage plan you may have bought until next year.
If you’ve had Medicare Advantage for a year or more, however, the open enrollment period is still “open” until December 7th, but you will want to make sure you can get a “Medigap” plan that fills in the 20% that real Medicare doesn’t cover.
Companies are required to write a Medigap policy for you at a reasonable price when you turn 65, no matter how sick you are or what preexisting conditions you may have, but if you’ve been “off Medicare” by being on Medicare Advantage for more than a year, they don’t have to write you a policy, so double-check that and sign up for a Medigap policy before making the switch back to real Medicare.
So, what’s this all about and why is it so complicated?
When George W. Bush and congressional Republicans (and a handful of bought-off Democrats) created Medicare Advantage in 2003, it was the fulfillment of half of Bush’s goal of privatizing Social Security and Medicare, dating all the way back to his unsuccessful run for Congress in 1978 and a main theme of his second term in office.
Medicare Advantage is not Medicare.
These plans are private health insurance provided by private corporations, who are then reimbursed at a fixed rate by the Medicare trust fund regardless of how much their customers use their insurance. Thus, the more they can screw their customers and us taxpayers by withholding healthcare payments, the more money they make.
With real Medicare,
if your doctor says you need a test, procedure, scan, or any other medical intervention you simply get it done and real Medicare pays the bill. No muss, no fuss, no permission needed. Real Medicare always pays, and if they think something’s not kosher, they follow up after the payment’s been made so as not to slow down the delivery of your healthcare.
With Medicare Advantage,
however, you’re subject to “pre-clearance,” meaning that the insurance company inserts itself between you and your doctor: You can’t get the medical help you need until or unless the insurance company pre-clears you for payment.
These companies thus make much of their billions in profit by routinely denying claims — 1.5 million, or 18 percent of all claims, were turned down in one year alone — leaving Advantage policy holders with the horrible choice of not getting the tests or procedures they need or paying for them out-of-pocket.
Given this, you’d think that most people would stay as far away from these private Medicare Advantage plans as they could. But Congress also authorized these plans to compete unfairly with real Medicare by offering things real Medicare can’t (yet). These include free or discounted dental, hearing, eyeglasses, gym memberships, groceries, rides to the doctor, and even cash rebates.
You and I pay for those freebies, but that’s only half of the horror story.
This year, as Matthew Cunningham-Cook pointed out in Wendell Potter’s brilliant Health Care un-covered Substack newsletter, we’re ponying up an additional $64 billion to give to these private insurance companies to “reimburse” them for the freebies they relentlessly advertise on television, online, and in print.
And here’s the most obscene part of the whole thing: the companies won’t tell the government (us!) how much of that $64 billion they’ve actually spent. They just take the money and say, “Thank you very much.” And then, presumably, throw a few extra million into the pockets of each of their already obscenely-well-paid senior executives.
For example, the former CEO of the nation’s largest Medicare Advantage provider, UnitedHealth, walked away with over a billion dollars in total compensation. With a “B.” One guy. His successor made off with over a half-billion dollars in pay and stock.
Good work if you can get it: all you need do is buy off a hundred or so members of Congress, courtesy of Clarence Thomas’ billionaire-funded tie-breaking vote on Citizens United, and threaten the rest of Congress with massive advertising campaigns for their opponents if they try to stop you.
And while the companies refuse to tell us how much of the $64 billion that we’re throwing at them this year to offer “free” dental, etc. is actually used, what we do know is that most of that money is not going to pay for the freebies they advertise. As Cunningham-Cook noted, in one study only 11 percent of Advantage policyholders who’d signed up with plans offering dental care used that benefit.
Another study showed over-the-counter-drug freebies were used only a third of the time, leaving $5 billion in the insurance companies money bins just for that “reimbursable” goodie. A later study found that at least a quarter of all Advantage policyholders failed to use any of the freebies they’d been offered when they signed up.
That’s an enormous amount of what the industry calls “breakage”; benefits offered and paid for by the government but not used. Billions of dollars left over every month. And, used or not, you and I sure paid for them.
And now it looks like things are about to get a whole lot worse.
When he was president last time, Donald Trump substantially expanded Medicare Advantage, calling real Medicare “socialism.” Project 2025 and candidate Trump both promised to end real Medicare “immediately” if Trump was re-elected; at the very least, they’ll make Medicare Advantage the “default” program people are steered into when they turn 65 and sign up for Medicare.
These giant insurance companies ripped off us taxpayers last year to the tune of an estimated $140 billion over and above what it would’ve cost us if people had simply been on real Medicare, according to a report from Physicians for a National Health Program (PNHP).
If there was no Medicare Advantage scam bleeding off all that cash to pay for executives’ private jets, real Medicare could be expanded to cover dental, vision, and hearing and even end the need for Medigap plans.
But for now, the privatization gravy train continues to roll along. The insurance giants use some of that money to buy legislators, and some of it for expensive advertising to dupe seniors into joining their programs. The company (Benefytt) that hired Joe Namath to pitch Medicare Advantage, for example, was recently hit with huge fines by the Federal Trade Commission for deceptive advertising.
“Benefytt pocketed millions selling sham insurance to seniors and other consumers looking for health coverage,” said Samuel Levine, Director of the FTC’s Bureau of Consumer Protection. “The company is being ordered to pay $100 million, and we’re holding its executives accountable for this fraud.”
And what was it that the Federal Trade Commission called “sham insurance”? Medicare Advantage. Nonetheless, the Centers for Medicare Services continues to let Benefytt and Namath market these products: welcome to the power of organized money.
And it’s huge organized money. Medicare Advantage plans are massive cash cows for the companies that run them. As Cigna prepares for a merger, for example, they’re being forced to sell off their Medicare Advantage division: it’s scheduled to go for $3.7 billion. Nobody pays that kind of money unless they expect enormous returns.
And how do they make those billions?
Most Medicare Advantage companies regularly do everything they can to intimidate you into paying yourself out-of-pocket. Often, they simply refuse payment and wait for you to file a complaint against them; for people seriously ill the cumbersome “appeals” process is often more than they can handle so they just write a check, pull out a credit card, or end up deeply in debt in their golden years.
As a result, hospitals and doctor groups across the nation are beginning to refuse to take Medicare Advantage patients. And in rural areas many hospitals are simply going out of business because Medicare advantage providers refuse to pay their bills.
California-based Scripps Health, for example, cares for around 30,000 people on Medicare Advantage and recently notified all of them that Scripps will no longer offer medical services to them unless they pay out-of-pocket or revert back to real Medicare.
They made this decision because over $75 million worth of services and procedures their physicians had recommended to their patients were turned down by Medicare Advantage insurance companies. In many cases, Scripps had already provided the care and is now stuck with the bills that the Advantage companies refuse to pay.
“We are a patient care organization and not a patient denial organization and, in many ways, the model of managed care has always been about denying or delaying care – at least economically. That is why denials, [prior] authorizations and administrative processes have become a very big issue for physicians and hospitals…”
Similarly, the Mayo Clinic has warned its customers in Florida and Arizona that they won’t accept Medicare Advantage any more, either. Increasing numbers of physician groups and hospitals are simply over being ripped off by Advantage insurance companies.
Traditional Medicare has been serving Americans well since 1965: it’s one of the most efficient single-payer systems to fund healthcare that’s ever been devised. But nobody was making a buck off it, so nobody could share those profits with greedy politicians. Enter Medicare Advantage, courtesy of George W. Bush and the GOP.
While several bills have been offered in Congress to do something about this — including Mark Pocan’s and Ro Khanna’s Save Medicare Act that would end these companies’ ability to use the word “Medicare” in their policy names and advertising — the amounts of money sloshing around DC in the healthcare space now are almost unfathomable.
So far this year, according to opensecrets.org, the insurance industry has spent $117,305,895 showering gifts and persuasion on our federal lawmakers to keep their obscene profits flowing.
It’s all one more example of how five corrupt Republicans on the US Supreme Court legalizing political bribery with Citizens Unitedhave screwed average Americans and made a handful of industry executives and investors fabulously rich.
They get away with it because when people choose to sign up for Medicare Advantage at 65 (or convert to these plans in their 60s or early 70s) they’re typically not sick — and thus cost the insurance companies little.
Tragically, the people signing up for these plans have no idea all the hassles, hoops, and troubles they might have to jump through when they do get sick, have an accident, or otherwise need medical assistance.
And since the last three years of life are typically the most expensive years for healthcare, the insurance denials are more likely to happen then — long after the person’s signed up with the Advantage company and it’s too late to go back to real Medicare.
This is why it typically takes a few years for people to figure out how badly they got screwed by not going with regular Medicare but instead putting themselves in the hands of private insurance companies.
“In spite of recommendations from Mr. Pauker’s doctors, his family said, Humana has repeatedly denied authorization for inpatient rehabilitation after hospitalization, saying at times he was too healthy and at times too ill to benefit.”
“Tens of millions of denials are issued each year for both authorization and reimbursements, and audits of the private insurers show evidence of ‘widespread and persistent problems related to inappropriate denials of services and payment,’ the investigators found.”
If you have “real” Medicare with a heavily regulated Medigap policy to cover the 20% Medicare doesn’t, you never have to worry.
Your bills get paid, you can use any doctor or hospital in the country who takes Medicare, and neither Medicare nor your Medigap provider will ever try to collect from you or force you to pay for what you thought was covered.
Neither you or your doctor will ever have to do the “pre-authorization” dance with real Medicare: those terrible experiences dealing with for-profit insurance companies are part of the past.
But if you have Medicare Advantage — which is not Medicare, but private health insurance — you’re on your own.
As the Times laid out:
“About 18 percent of [Advantage] payments were denied despite meeting Medicare coverage rules, an estimated 1.5 million payments for all of 2019. In some cases, plans ignored prior authorizations or other documentation necessary to support the payment. These denials may delay or even prevent a Medicare Advantage beneficiary from getting needed care…”
Buying a Medicare Advantage policy is a leap in the dark, and the federal government is not there to catch you. And it’s all perfectly legal, thanks to Bush’s 2003 law, so your state insurance commissioner usually can’t or won’t help.
Thus, here we are, handing billions of dollars a month to insurance industry executives so they can buy new Swiss chalets, private jets, and luxury yachts. And so they can compete — unfairly — with Medicare itself, driving LBJ’s most proud achievement into debt and crisis.
Enough is enough. Let your members of Congress know it’s beyond time to fix the Court and Medicare, so scams like Medicare Advantage can no longer rip off America’s seniors while making industry executives richer than Midas.
And if you got hooked into switching out of real Medicare and now find yourself in a Medicare Advantage plan, you have three days to back out and return to real Medicare. For more information, you can also contact the nonprofit and real-Medicare-supporting Medicare Rights Center at 800-333-4114.
There’s only one person in this photograph/video of a recent G7 meeting who represents a country where an illness can destroy an entire family, leaving them bankrupt and homeless, with the repercussions of that sudden fall into poverty echoing down through generations.
Most Americans have no idea that the United States is quite literally the only country in the developed world that doesn’t define healthcare as an absolute right for all of its citizens. That’s it. We’re the only one left.
The United States spends more on “healthcare” than any other country in the world: about 17% of GDP.
Switzerland, Germany, France, Sweden and Japan all average around 11%, and Canada, Denmark, Belgium, Austria, Norway, Netherlands, United Kingdom, New Zealand and Australia all come in between 9.3% and 10.5%.
We are literally the only developed country in the world with an entire multi-billion-dollar for-profit industry devoted to parasitically extracting money from us to then turn over to healthcare providers on our behalf. The for-profit health insurance industry has attached itself to us like a giant, bloodsucking tick.
They all failed, and when I did a deep dive into the topic two years ago for my book The Hidden History of American Healthcare I found two major barriers to our removing that tick from our backs.
The early opposition, more than 100 years ago, to a national healthcare system came from southern white congressmen (they were all men) and senators who didn’t want even the possibility that Black people could benefit, health-wise, from white people’s tax dollars. (This thinking apparently still motivates many white Southern politicians.)
The leader of that healthcare-opposition movement in the late 19th and early 20th centuries was a German immigrant named Frederick Hoffman, as I mentioned in a recent newsletter. Hoffman was a senior executive for the Prudential Insurance Company, and wrote several books about the racial inferiority of Black people, a topic he traveled the country lecturing about.
His most well-known book was titled Race Traits and Tendencies of the American Negro. It became a major best-seller across America when it was first published for the American Economic Association by the Macmillan Company in 1896, the same year the Supreme Court’s Plessy v. Ferguson decision legally turned the entire US into an apartheid state.
Hoffman taught that Black people, in the absence of slavery, were so physically and intellectually inferior to whites that if they were simply deprived of healthcare the entire race would die out in a few generations. Denying healthcare to Black people, he said, would solve the “race problem” in America.
Southern politicians quoted Hoffman at length, he was invited to speak before Congress, and was hailed as a pioneer in the field of “scientific racism.” Race Traits was one of the most influential books of its era.
By the 1920s, the insurance company he was a vice president of was moving from life insurance into the health insurance field, which brought an added incentive to lobby hard against any sort of a national healthcare plan.
Which brings us to the second reason America has no national healthcare system: profits.
And that’s just one of multiple giant insurance companies feeding at the trough of your healthcare needs.
Much of that money, and the pay for the multiple senior executives at that and other insurance companies who make over $1 million a year, came from saying “No!” to people who file claims for payment of their healthcare costs.
Companies offering such “primary” health insurance simply don’t exist (or are tiny) in almost every other developed country in the world. Mostly, where they do exist, they serve wealthier people looking for “extras” beyond the national system, like luxury hospital suites or air ambulances when overseas. (Switzerland is the outlier with exclusively private insurance, but it’s subsidized, mandatory, and non-profit.)
If Americans don’t know this, they intuit it.
In the 2020 election there were quite a few issues on statewide ballots around the country. Only three of them outpolled Joe Biden’s win, and expanding Medicaid to cover everybody was at the top of that list. (The other two were raising the minimum wage and legalizing pot.)
The last successful effort to provide government funded, single-payer healthcare insurance was when Lyndon Johnson passed Medicare and Medicaid (both single-payer systems) in the 1960s. It was a hell of an effort, but the health insurance industry was then a tiny fraction of its current size.
In 1978, when conservatives on the Supreme Court legalized corporations owning politicians with their Buckley v Belotti decision (written by Justice Louis Powell of “Powell Memo” fame), they made the entire process of replacing a profitable industry with government-funded programs like single-payer vastly more difficult, regardless of how much good they may do for the citizens of the nation.
The Court then doubled-down on that decision in 2010, when the all-conservative vote on Citizens Unitedcemented the power of billionaires and giant corporations to own politicians and even write and influence legislation and the legislative process.
Medicare For All, like Canada has, would save American families thousands every year immediately and do away with the 500,000+ annual bankruptcies in this country that happen only because somebody in the family got sick. But it would kill the billions every week in profits of the half-dozen corporate giants that dominate the health insurance industry.
This won’t be happening with a billionaire in the White House, but if we want to bring America into the 21st century with the next administration, we need to begin working, planning, and waking up voters now.
In late 2025, two events reset the U.S. health system’s future at least through 2026 and possibly beyond:
November 5, 2024: The Election: Its post-mortem by pollsters and pundits reflects a country divided and unsettled: 22 Red States, 7 Swing States and 21 Blue States. But a solid majority who thought the country was heading in the wrong direction and their financial insecurity driving voters to return the 45th President to the White House. With slim majorities in the House and Senate, and a short-leash before mid-term elections November 3, 2026, the Trump team has thrown out ‘convention’ in their setting policies and priorities for their second term. That includes healthcare.
December 4, 2024: The Murder of a Health Executive : The murder of Brian Thompson, United Healthcare CEO, sparked hostility toward health insurers and a widespread backlash against the corporatization of the U.S. health system. While UHG took the most direct hit for its aggressiveness in managing access and coverage disputes, social media and mainstream journalists exposed what pollsters affirmed—the majority of American’s distrust the health system, believing it puts its profits above their needs. And their polls indicate animosity is highest among young adults, in lower income households and among members of its own workforce.
These events provide the backdrop for what to expect this year and next. Four directional shifts seem to underly actions to date and announced plans:
From elitism to populism: Key personnel and policy changes will draw less from Ivy League credentials, DC connections and recycled federal health agency notables and more from private sector experience, known disruptors and unconventional thought leaders. Notably, the new Chairs of the 7 Congressional Committees that control healthcare regulation, funding and policy changes in the 119th Congress represent LA, AL, WV, ID, VA, MO & KY constituents—hardly Ivy League territory.
From workforce disparities to workforce modernization: The Departments of Health & Human Services, Labor, Commerce and Treasury will attempt to suspend/modify regulatory mandates and entities they deem derived from woke ideology. The Trump team will replace them with policies that enable workforce de-regulation and modernization in the private sector. Hiring quotas, non-compete contracts, DEI et al will get a fresh look in the context of technology-enabled workplaces and supply-demand constraints. The HR function in every organization will become ground zero for Trump Healthcare 2.0 system transformation.
From western medicine to whole person wellbeing: HHS Secretary Nominee Robert F. Kennedy Jr. (RFK) Jr.’s “Make America Healthy Again” pledges war on ultra-processed foods. CMS’ designee Mehmet Oz advocates for vitamins, supplements and managed care. FDA nominee Marty Makary, a Hopkins surgeon, is a RFKJ ally in the “Health Freedom” movement promoting suspicion about ‘mainstream medicine’ and raising doubts about vaccination efficacy for children and low-risk adults. NIH nominee Jay Bhattacharya, director of Stanford’s Center for Demography and Economics of Health and Aging, opposed Covid-19 lockdowns and is critical of vaccine policies. Collectively, this four-some will challenge conventional western (allopathic) medicine and add wide-range of non-traditional interventions that are a safe and cost-effective to the treatment arsenal for providers and consumers. The food supply will be a major focus: HHS will work closely with the USDA (nominee Brooke Rollins, currently CEO of the America First Policy Institute, to reduce the food chain’s dependence on ultra-processed foods in public health.
From DC dominated health policies to states: The 2022 Supreme Court’ Dobbs decision opened the door for states to play the lead role in setting policies for access to abortion for their female citizens. It follows federalism’s Constitutional preference that Washington DC’s powers over states be enumerated and limited. Thus, state provisions about healthcare services for its citizens will expand beyond their already formidable scope. Likely actions in some states will include revised terms and conditions that facilitate consolidation, allowance for physician owned hospitals and site-neutral payments, approval of “skinny” individual insurance policies that do not conform to the Affordable Care Act’s qualified health plan spec’s, expanded scope of practice for nurse practitioners, drug price controls and many others. At least for the immediate future, state legislatures will be the epicenters for major policy changes impacting healthcare organizations; federal changes outside appropriations activity are unlikely.
Transforming the U.S. health system is a bodacious ambition for the incoming Trump team. Early wins will be key—like expanding price transparency in every healthcare sector, softening restrictions on private equity investments, targeted cuts in Medicaid and Medicare funding and annulment of the Inflation Reduction Act. In tandem, it has promised to cut Federal government spending by $2 trillion and lower prices on everything including housing and healthcare—the two spending categories of highest concern to the working class. Healthcare will figure prominently in Team Trump’s agenda for 2025 and posturing for its 2026 mid-term campaign. And equally important, healthcare costs also figure prominently in quarterly earnings reports for companies that provide employee health benefits forecast to be 8% higher this year following a 7% spike the year prior. Last year’s 23% S&P growth is not expected to repeat this year raising shareholder anxiety and the economy’s long-term resilience and the large roles housing and healthcare play in its performance.
My take:
The 2024 election has been called a change election. That’s unwelcome news to most organizations in healthcare, especially the hospitals, physicians, post-acute providers and others who provide care to patients and operate at the bottom of the healthcare pyramid.
Equipping a healthcare organization to thoughtfully prepare for changes amidst growing uncertainty requires extraordinary time and attention by management teams and their Boards. There are no shortcuts. Before handicapping future state scenario possibilities, contingencies and resource requirements, a helpful starting point is this: On the four most pressing issues facing every U.S. healthcare company/organization today, Boards and Management should discuss…
Trust: On what basis can statements about our performance be verified? Is the data upon which our trust is based readily accessible? Does the organization’s workforce have more or less trust than outside stakeholders? What actions are necessary to strengthen/restore trust?
Purpose: Which stakeholder group is our organization’s highest priority? What values & behaviors define exceptional leadership in our organization? How are they reflected in their compensation?
Affordability: How do we measure and monitor the affordability of our services to the consumers and households we ultimately depend? How directly is our organization’s alignment of reducing cost reduction and pass-through savings to consumers? Is affordability a serious concern in our organization (or just a slogan)?
Scale: How large must we be to operate at the highest efficiency? How big must we become to achieve our long-term business goals?
This week, thousands of healthcare’s operators will be in San Francisco (JPM Healthcare Conference), Naples (TGI Leadership Conference) and in Las Vegas (Consumer Electronics Show) as healthcare begins a new year. No one knows for sure what’s ahead or who the winners and losers will be. What’s for sure is that healthcare will be in the spotlight and its future will not be a cut and paste of its past.
PS: The parallels between radical changes facing the health system and other industries is uncanny. College athletics is no exception. As you enjoy the College Football Final Four this weekend, consider its immediate past—since 2021, the impact of Name, Image and Likeness (NIL) monies on college athletics, and its immediate future–pending regulation that will codify permanent revenue sharing arrangements (to be implemented 2026-2030) between college athletes, their institutions and sponsors. What happened to the notion of student athlete and value of higher education? Has the notion of “not-for-profit” healthcare met a similar fate? Or is it all just business?
In late 2025, two events reset the U.S. health system’s future at least through 2026 and possibly beyond:
November 5, 2024: The Election: Its post-mortem by pollsters and pundits reflects a country divided and unsettled: 22 Red States, 7 Swing States and 21 Blue States. But a solid majority who thought the country was heading in the wrong direction and their financial insecurity driving voters to return the 45th President to the White House. With slim majorities in the House and Senate, and a short-leash before mid-term elections November 3, 2026, the Trump team has thrown out ‘convention’ in their setting policies and priorities for their second term. That includes healthcare.
December 4, 2024: The Murder of a Health Executive : The murder of Brian Thompson, United Healthcare CEO, sparked hostility toward health insurers and a widespread backlash against the corporatization of the U.S. health system. While UHG took the most direct hit for its aggressiveness in managing access and coverage disputes, social media and mainstream journalists exposed what pollsters affirmed—the majority of American’s distrust the health system, believing it puts its profits above their needs. And their polls indicate animosity is highest among young adults, in lower income households and among members of its own workforce.
These events provide the backdrop for what to expect this year and next. Four directional shifts seem to underly actions to date and announced plans:
From elitism to populism: Key personnel and policy changes will draw less from Ivy League credentials, DC connections and recycled federal health agency notables and more from private sector experience, known disruptors and unconventional thought leaders. Notably, the new Chairs of the 7 Congressional Committees that control healthcare regulation, funding and policy changes in the 119th Congress represent LA, AL, WV, ID, VA, MO & KY constituents—hardly Ivy League territory.
From workforce disparities to workforce modernization: The Departments of Health & Human Services, Labor, Commerce and Treasury will attempt to suspend/modify regulatory mandates and entities they deem derived from woke ideology. The Trump team will replace them with policies that enable workforce de-regulation and modernization in the private sector. Hiring quotas, non-compete contracts, DEI et al will get a fresh look in the context of technology-enabled workplaces and supply-demand constraints. The HR function in every organization will become ground zero for Trump Healthcare 2.0 system transformation.
From western medicine to whole person wellbeing: HHS Secretary Nominee Robert F. Kennedy Jr. (RFK) Jr.’s “Make America Healthy Again” pledges war on ultra-processed foods. CMS’ designee Mehmet Oz advocates for vitamins, supplements and managed care. FDA nominee Marty Makary, a Hopkins surgeon, is a RFKJ ally in the “Health Freedom” movement promoting suspicion about ‘mainstream medicine’ and raising doubts about vaccination efficacy for children and low-risk adults. NIH nominee Jay Bhattacharya, director of Stanford’s Center for Demography and Economics of Health and Aging, opposed Covid-19 lockdowns and is critical of vaccine policies. Collectively, this four-some will challenge conventional western (allopathic) medicine and add wide-range of non-traditional interventions that are a safe and cost-effective to the treatment arsenal for providers and consumers. The food supply will be a major focus: HHS will work closely with the USDA (nominee Brooke Rollins, currently CEO of the America First Policy Institute, to reduce the food chain’s dependence on ultra-processed foods in public health.
From DC dominated health policies to states: The 2022 Supreme Court’ Dobbs decision opened the door for states to play the lead role in setting policies for access to abortion for their female citizens. It follows federalism’s Constitutional preference that Washington DC’s powers over states be enumerated and limited. Thus, state provisions about healthcare services for its citizens will expand beyond their already formidable scope. Likely actions in some states will include revised terms and conditions that facilitate consolidation, allowance for physician owned hospitals and site-neutral payments, approval of “skinny” individual insurance policies that do not conform to the Affordable Care Act’s qualified health plan spec’s, expanded scope of practice for nurse practitioners, drug price controls and many others. At least for the immediate future, state legislatures will be the epicenters for major policy changes impacting healthcare organizations; federal changes outside appropriations activity are unlikely.
Transforming the U.S. health system is a bodacious ambition for the incoming Trump team. Early wins will be key—like expanding price transparency in every healthcare sector, softening restrictions on private equity investments, targeted cuts in Medicaid and Medicare funding and annulment of the Inflation Reduction Act. In tandem, it has promised to cut Federal government spending by $2 trillion and lower prices on everything including housing and healthcare—the two spending categories of highest concern to the working class. Healthcare will figure prominently in Team Trump’s agenda for 2025 and posturing for its 2026 mid-term campaign. And equally important, healthcare costs also figure prominently in quarterly earnings reports for companies that provide employee health benefits forecast to be 8% higher this year following a 7% spike the year prior. Last year’s 23% S&P growth is not expected to repeat this year raising shareholder anxiety and the economy’s long-term resilience and the large roles housing and healthcare play in its performance.
My take:
The 2024 election has been called a change election. That’s unwelcome news to most organizations in healthcare, especially the hospitals, physicians, post-acute providers and others who provide care to patients and operate at the bottom of the healthcare pyramid.
Equipping a healthcare organization to thoughtfully prepare for changes amidst growing uncertainty requires extraordinary time and attention by management teams and their Boards. There are no shortcuts. Before handicapping future state scenario possibilities, contingencies and resource requirements, a helpful starting point is this: On the four most pressing issues facing every U.S. healthcare company/organization today, Boards and Management should discuss…
Trust: On what basis can statements about our performance be verified? Is the data upon which our trust is based readily accessible? Does the organization’s workforce have more or less trust than outside stakeholders? What actions are necessary to strengthen/restore trust?
Purpose: Which stakeholder group is our organization’s highest priority? What values & behaviors define exceptional leadership in our organization? How are they reflected in their compensation?
Affordability: How do we measure and monitor the affordability of our services to the consumers and households we ultimately depend? How directly is our organization’s alignment of reducing cost reduction and pass-through savings to consumers? Is affordability a serious concern in our organization (or just a slogan)?
Scale: How large must we be to operate at the highest efficiency? How big must we become to achieve our long-term business goals?
This week, thousands of healthcare’s operators will be in San Francisco (JPM Healthcare Conference), Naples (TGI Leadership Conference) and in Las Vegas (Consumer Electronics Show) as healthcare begins a new year. No one knows for sure what’s ahead or who the winners and losers will be. What’s for sure is that healthcare will be in the spotlight and its future will not be a cut and paste of its past.
PS: The parallels between radical changes facing the health system and other industries is uncanny. College athletics is no exception. As you enjoy the College Football Final Four this weekend, consider its immediate past—since 2021, the impact of Name, Image and Likeness (NIL) monies on college athletics, and its immediate future–pending regulation that will codify permanent revenue sharing arrangements (to be implemented 2026-2030) between college athletes, their institutions and sponsors. What happened to the notion of student athlete and value of higher education? Has the notion of “not-for-profit” healthcare met a similar fate? Or is it all just business?