
Thought of the Day: We are all one

Faced with tighter margins and continued rising costs, many health system C-suites are restructuring. At least 17 health systems have reorganized executive teams and some eliminated C-suite roles.
The chief operating officer role in particular has been on the chopping block for health systems but not everyone is slimming down.
Some are bulking up amid organizational transformation with an eye on the future.
In June, Sutter Health in Sacramento, Calif., named Todd Smith, MD, its inaugural senior vice president and chief physician executive, responsible for supporting the health system through clinical transformation. Dr. Smith will focus on service line standards, reducing variation and strengthening the system’s relationship with medical group and community physicians.
Sutter isn’t the only system adding clinical leaders to the C-suite. Mass General Brigham in Somerville, Mass., named Erica Shenoy, MD, PhD, its first chief of infection control in June. Her expanded role is accountable for leading the integration of infection control at the system and developing and implementing infection control standards, policies and measurements. She was also appointed to the National Infection Control Advisory Committee to guide HHS earlier this year.
Meritus Health in Hagerstown, Md., added physician leadership to its executive team. Adrian Park, MD, became the system’s first chief surgical officer with responsibility for building a surgical program with advanced technology and minimally invasive procedures to the system. He is known for surgical innovation in laparoscopic techniques, and holds more than 20 patents.
MaineHealth in Portland recently added Chris Thompson, MD, to the C-suite as the system’s first chief medical transformation officer. He is responsible for chief medical officer duties as well as innovating in care delivery.
Richmond, Va.-based VCU Health and OU Health in Oklahoma City named their first chief nursing executives as well earlier this year.
Health systems are also adding strategic experts with expertise in patient experience, transformation and data analytics.
Atlanta-based Emory Healthcare created a new role for Amaka Eneanya, MD, to serve as chief transformation officer, accountable for enhancing patient and clinician experiences. She took on the role in July and is tasked with developing systemwide strategies to boost patient experience, improve access to care, increase community engagement and enrich clinician experience. Dr. Eneanya works with the system’s diversity, equity and inclusion office to prioritize strategies for health equity, diversity and inclusion in care delivery as well.
“Amaka is a forward-thinking leader who is well versed in transformational strategy and operational structure and will help us move Emory Healthcare to the next level,” said Joon S. Lee, MD, CEO of Emory Healthcare. “We look forward to working with her in our continued pursuit to transform and strengthen patient access and the patient experience.”
Last year, Centura Health in Centennial, Colo., also added a chief transformation officer, Scott Lichtenberger, MD, as a new position to balance short-term improvements and long-term value. He is responsible for ensuring the system delivers results quickly.
Finally, Cleveland Clinic has elevated another IT leader into the C-suite in recent weeks. Albert Marinez was named the system’s first chief analytics officer, set to begin his new role Aug. 28. He previously served as chief analytics officer of Intermountain Health in Salt Lake City, and will be responsible for overseeing data strategies for better patient care and lower costs at Cleveland Clinic. He will also have accountability for boosting the system’s growth alongside chief digital officer Rohit Chandra, PhD.
https://mailchi.mp/altarum/health-sector-economic-indicators-briefs-august-2023?e=b4c24e7e20

The latest Altarum Health Sector Economic Indicators show that health spending as a percent of GDP has stabilized near 17.5%, health care price growth and economywide inflation recently converged, and the health sector added over 60,000 jobs in July. See the highlights below.
Health spending as a percent of GDP has stabilized at 17.5%
Health care price growth and economywide inflation finally converge
Health care adds 63,000 jobs in July, the largest increase since July 2022

Rating agencies have done a great job in increasing transparency around how ratings are determined. Detailed methodologies, scorecards, and medians are a big part of that effort.
Central to the rating process is the rating committee. All rating decisions are made by a rating committee, not an individual. The rating committee provides a robust discussion of various viewpoints as it deliberates, votes, and assigns ratings to the debt instrument.
Here are five things to know about what happens in a rating committee.
1. Rating committees are presided over by a Rating Committee Chair.
The Chair’s primary responsibility is to check that the committee follows numerous processes that meet company and SEC-mandated guidelines. For example, the Chair must verify that the correct methodology is being used to determine the rating, or if a rating requires additional methodologies (such as short-term rating methodologies on variable rate debt). The Chair must confirm that the rating decision will be based on verifiable facts or assessments (such as an audit) and that voting members are free of conflicts. Committees can be subject to internal and external reviews after the fact to ensure that decisions were made impartially and documented correctly.
The Chair ensures that the committee is populated with voting members who possess in-depth knowledge about the sector or related-credit knowledge (such as a higher education analyst in the case of an academic medical center) and are skilled in credit assessment. Each voting member has one vote and an equal vote. Serving as a voting member of a rating committee or as a Chair is a privilege and must be earned.
2. The rating committee discussion centers around the ability of a borrower to repay its obligations, or said another way, the likelihood of payment default.
As such, debt structure is integral to the rating committee. Detailed information provided in the committee package will include information on outstanding and proposed debt (if a bond financing is imminent), debt structure risks (fixed versus variable, for example), debt service schedule (level payments or with bullets), maturities and call dates, taxable and tax-exempt debt, bank lines and revolvers, counterparty risk and termination events, derivative products such as interest rate swaps and collateral thresholds, senior-subordinate debt structures, bond and bank covenants, obligated group, and security pledge, to name a few. Leases and pension obligations are also considered, particularly when liabilities outsize the direct debt.
Rating committees review hundreds of financial metrics to assess recent financial performance and an organization’s ability to pay debt in the future. Audited financial statements, year-to-date results, and annual budgets and projections are the basis for computing the financial ratios. Non-quantitative factors include success with past strategies and capital projects, market position and essentiality, management, governance and corporate structure, workforce needs, and local economic data. Confidential information provided by the organization is also shared. The job of the lead analyst is to distill all the information and present an organized credit story to the rating committee.
3. Rating consistency is paramount.
An “A” should be an “A” should be an “A.” Comparables (or “comps”) are an important part of the rating committee. Comps may include the other hospitals and health systems operating in the same state given shared Medicaid and state regulations (such as Certificate of Need or state-mandated minimum wage), workforce environment (such as the presence of active unions), and similar economic factors. Like-sized peers in the same rating category also populate comps. The type of hospital being evaluated is also important. For example, health systems that own health plans would be compared to other integrated delivery systems; likewise for children’s hospitals, academic medical centers, or subacute care providers. Medians are also a part of the comps and provide relativity to like-rated borrowers by highlighting outliers.
4. Rating committee spends time reviewing the draft report to make sure the committee’s views are accurately expressed and check that confidential information was not inadvertently revealed. If you want to know what was discussed in the rating committee, read the last rating report.
Over the years, many executives have asked to speak directly to the rating committee. While that is not possible, you can bring your voice to the discussion with an informative, well-crafted rating presentation. That brings me to my final “inside rating committee” point.
5. Rating presentations matter.
Effective, informative presentations that encapsulate your organization’s strengths will be shared with the rating committee. Every slide in your presentation should send a clear message that the organization’s ability to repay the debt and exceed covenants is strong. Emphasize the positives, acknowledge the challenges, and share what your action plan is to address them. Do your homework and review what you shared with the analysts last year; they will be doing the same to prepare. Provide updates on how the strategic plans are going. If you exceeded your financial goals, explain how. If you fell short, explain why.
How you tell the story is as important as the story itself. That’s how you can inform the discussion and ensure your voice is heard around the rating committee table.
Hospital and insurer contract negotiations are often framed as an industry gauntlet, a defined period of time with an objective outcome where big talk does not translate to money. But reimbursement rates secured in new contracts are only one piece of hospitals’ payer-induced headaches.
Traditionally, a health system and commercial insurer would occasionally run into a wall in the contract negotiation process. This could play out into a dispute palpable enough to consumers that it warranted headlines. These impasses generally lasted a matter of weeks with no significant disruptions before outside pressure drove the parties to compromise.
Over the past five years or so, the nature of provider-payer conflicts intensified and may be on the cusp of unprecedented severity given health systems’ financial pressures. At the same time, agreed-upon reimbursement rates are only the tip of the iceberg when it comes to payment health systems can expect from commercial insurers, who have many more defensive plays in their playbook.
They boil down to a classic line from a 1968 movie: deny, deny, deny.
Russ Johnson is CEO of LMH Health, a 102-year-old, independent, nonprofit health system based in Lawrence, Kan. The $350 million organization is anchored by a 174-bed hospital. As he puts it: “We’re not tiny, but we’re not very big.”
Mr. Johnson has spent 37 years working in healthcare, holding senior leadership positions in hospitals and health systems in rural communities and large cities. It’s difficult to identify many things going well when it comes to provider-payer relationships, but Mr. Johnson told Becker’s that it’s the payer movements beneath the reimbursement rates that are worsening and causing greater pain today.
“The part that’s getting worse is the practices behind and underneath the contracts — the sophistication and implementation of pay practices, information systems, artificial intelligence and computer algorithms that are just denying claims by the thousands every month,” he said.
The reimbursement rates secured in contracts are what you can see above water. Beneath, health insurers are moving faster and kicking harder. Throughout the first three months of 2023, about one-third of inpatient and outpatient claims submitted by providers to commercial payers went unpaid for more than 90 days, according to an analysis from Crowe.
“So many more claims are now surfacing with some kind of a fallout on a denial, a downcoding or a pre-authorization — you know, the proverbial dotting the i’s and crossing the t’s, sometimes. But what is abundantly clear is it is not fundamentally about a clinical difference,” Mr. Johnson said.
Denials were once reserved for a sliver of expensive treatments and have now become common occurrence for mundane, ordinary medical care and treatments such as inhalers or familiar medications for chronic conditions a patient has managed for years. The administrative burden is something close to a requirement to prove residency every month to receive electricity or verifying eligibility to work in the U.S. every week for a paycheck — redundant, time-wasting activity for ordinary, essential things.
“For our business office to keep up with what I frankly think is mischief by the payers in terms of denials, pre-authorization, DRG downcoding and a completely unengaged experience trying to negotiate — or to have our physicians call in and do a peer-to-peer conferences about clinical necessity — it’s demoralizing, frankly,” Mr. Johnson said. “Dealing with denial from our payers is one of the biggest dissatisfiers our physicians face.”
Authors of the 2010 Affordable Care Act worried that provisions to expand health insurance access — such as barring health insurers’ refusal to cover patients with preexisting conditions — could cause them to ratchet up other tactics to make up for the change. With this in mind, the law charged HHS with monitoring health plan denial rates, but oversight has been unfulfilled, leaving denials widespread.
Data and numbers on denial rates are not easy to find, but some examination paints a picture rich with variation. An analysis of 2021 plans on Healthcare.gov conducted by KFF found nearly 17 percent of in-network claims were denied, with rates varying from 2 percent to 49 percent. The reasons for the bulk of denials are unclear. About 14 percent were attributed to an excluded service, 8 percent to lack of pre-authorization or referral and 2 percent to questions of medical necessity. A whopping 77 percent were classified as “all other reasons.”
Adding to the inconsistency is the fact that health plan denial rates fluctuate year over year. In 2020, a gold-level health plan offered by Oscar Insurance in Florida denied 66 percent of payment requests; in 2021 it denied 7 percent.
There is much to learn about the ways AI will shape healthcare, and its potential to further expedite and increase denials is concerning. Cigna faces a class-action lawsuit alleging it bypassed requirements for claim review before denial by having an algorithm — dubbed “PXDX” — complete review before having physicians sign off on batches of denied claims. The lawsuit followed a ProPublica report on the practice, which said Cigna physicians denied more than 300,000 claims over two months in 2022 through the system, which equated to 1.2 seconds of review per claim on average.
AI is often touted as a potential, looming replacement to hardworking healthcare professionals, but in the day to day it exacerbates the administrative burdens that already bring them down.
“Nobody becomes a physician because they hope to feel like a cog in a factory,” Michael Ivy, MD, deputy chief medical officer of Yale New Haven (Conn.) Health, told Becker’s. “However, between meeting the demands of payers for referrals, denials of payment and increased documentation requirements in order to assure proper reimbursement and risk adjustment, as well as an increasing number of production metrics, it can be difficult not to feel like a cog.”

A number of hospitals and health systems are trimming their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations that were announced within the past year and/or take effect later in 2023.
Editor’s Note: This webpage was updated Aug. 10 and will continue to be updated. Stories are listed under the month they were reported on by Becker’s.
August
The University of Arkansas for Medical Sciences is laying off 51 workers in support services, administration and service lines. Some previously open positions will also be left vacant, the Little Rock-based institution told the Becker’s in a prepared statement. Some job duties will be reassigned.
Springfield, Ill.-based Memorial Health is laying off hundreds of employees, including 20 percent of leadership positions. Affected employees represent 5 percent of Memorial’s total salary and benefits, according to a statement provided to Becker’s. The cuts focused on system leadership, administrative and support sectors.
Boone Health, a county-owned system based in Columbia, Mo., will cut 62 jobs, most of which are unfilled. Fifteen of the 62 positions are held by existing employees.
The in-home care arm of Syracuse, N.Y.-based St. Joseph’s Health, part of Livonia, Mich.-based Trinity Health, is closing in October, pending the discharge of all patients. The closure includes the termination of 71 employees. Mark McPherson, president and CEO of Trinity Health At Home, said 63 full and part-time positions are being eliminated, while the remaining eight were contingent positions.
July
Chapel Hill, N.C.-based UNC Health will lay off 246 employees. The reduction will occur after the organization ends services at a behavioral health facility in Raleigh on Sept. 30, according to a WARN notice filed July 21 with the North Carolina Department of Commerce.
Philadelphia-based Jefferson Health is reducing its workforce by about 400 positions. The reduction represents approximately 1 percent of the workforce.
Tupelo-based North Mississippi Health Services is moving forward with layoffs and job reassignments as part of its “redesign” plan to improve the organization’s financial picture, according to a message sent to NMHS employees and affiliated providers July 19. NMHS did not provide the number of affected positions or types of positions affected.
Allina Health began layoffs affecting about 350 team members throughout the Minneapolis-based organization. The health system said the layoffs began July 17 and that most of the affected jobs are leadership and non-direct caregiving roles.
Middletown, N.Y.-based Garnet Health laid off 49 employees, including 25 leaders. The reductions represent 1.13 percent of the organization’s total workforce.
June
Coral Gables-based Baptist Health South Florida is offering its executives at the director level and above a “one-time opportunity” to apply for voluntary separation, according to a June 29 Miami Herald report. Decisions on buyout applications will be made during the summer.
MultiCare Health System, a 12-hospital organization based in Tacoma, Wash., will lay off 229 employees, or about 1 percent of its 23,000 staff members, including about two dozen leaders, as part of cost-cutting efforts, the health system said June 29. The layoffs primarily affect support departments, such as marketing, IT and finance.
Greensburg, Pa.-based Independence Health System laid off 53 employees and has cut 226 positions — including resignations, retirements and elimination of vacant positions — since January, The Butler Eagle reported June 28. The 226 reductions began at the executive level, with 13 manager positions terminated in March.
Billings (Mont.) Clinic will lay off workers as part of a restructuring plan to address financial and operational headwinds in today’s healthcare environment, the organization confirmed. The layoffs are expected to affect approximately 27 or fewer positions.
Melbourne, Fla.-based Health First is eliminating some positions and leaving open ones vacant, Florida Today reported June 21. Seventeen jobs will be cut and 36 will be left unfilled, according to Paula Just, the health system’s chief experience officer.
Pittsburgh-based Highmark Health laid off 118 employees on June 21, including two from Allegheny Health Network, a spokesperson for the health system told Becker’s. The layoffs follow the health system’s cutbacks in March and April, according to the Pittsburgh Business Times. Highmark laid off 141 workers earlier this year.
Vibra Hospital of Western Massachusetts, a long-term-acute care hospital in Springfield, will lay off 87 employees by Aug. 15 ahead of the facility’s planned closure. About 30 patients will be relocated to Baystate Health’s Valley Springs Behavioral Health Hospital in Holyoke, Mass., which will open in August.
Cortez, Colo.-based Southwest Memorial Hospital laid off nine people to help ensure the hospital is staffed appropriately, and create financial stability for the future, a spokesperson confirmed to Becker’s. The spokesperson, Chuck Krupa, said the layoffs occurred June 14 and included administrative workers. No bedside care positions were affected.
Henry Mayo Newhall Hospital in Valencia, Calif., is making “a little over 100” layoffs amid financial challenges, spokesperson Patrick Moody confirmed to Becker’s. Mr. Moody said the layoffs affect workers “in a wide range of hospital departments.” This includes some management-level employees. The hospital, which has about 1,800 employees total, is not providing specific numbers for specific job titles or departments.
Dartmouth Health is laying off 75 workers and eliminating 100 job vacancies. The layoffs came after the Lebanon, N.H.-based health system implemented a performance improvement plan in November.
Seattle Children’s is eliminating 135 leader roles, citing financial challenges. The management restructuring and reduction affects 1.5 percent of employees across the organization.
White Rock (Texas) Medical Center laid off 30 workers across 28 departments. The layoffs include clinical and administrative roles.
Jackson, Miss.-based St. Dominic Health Services is laying off 157 workers and ending behavioral health services. The reduction represents 5.5 percent of the hospital’s workforce.
Danville, Pa.-based Geisinger laid off 47 employees from its IT department. The reduction is part of a restructuring plan to offset high labor and supply costs.
Cascade Behavioral Health Hospital in Tukwila, Wash., is winding down operations and laying off 288 employees. The 137-bed psychiatric facility is slated to close by July 31.
Cambridge (Mass.) Health Alliance is laying off 69 employees, reducing the hours of 15 others and eliminating 170 open positions, according to The Boston Globe. The reductions are primarily in management, administrative and support areas, a health system spokesperson told Becker’s.
May
Wenatchee, Wash.-based Confluence Health has eliminated its chief operating officer amid restructuring efforts and financial pressures, the health system confirmed to Becker’s May 16.
Conemaugh Memorial Medical Center, a Duke LifePoint hospital in Johnstown, Pa., has laid off less than 1 percent of its workforce, the hospital confirmed to Becker’s May 15.
Community Health Network, a nonprofit health system based in Indianapolis, plans to cut an unspecified number of jobs as it restructures its workforce and makes organizational changes. The health system confirmed the job cuts in a statement shared with Becker’s on May 11. It did not say how many jobs would be cut or which positions would be affected.
New Orleans-based Ochsner Health eliminated 770 positions, or about 2 percent of its workforce, on May 11. This is the largest layoff to date for the health system.
Cedars-Sinai Medical Center eliminated the positions of 131 employees and cut about two dozen other jobs at related Cedars-Sinai facilities, a spokesperson confirmed via a statement shared with Becker’s May 7. The Los Angeles-based organization said reductions represent less than 1 percent of the workforce and apply to management and non-management roles primarily in non-patient care jobs.
Rochester (N.Y.) Regional Health is eliminating about 60 positions. A statement from RRH said the changes affect less than one-half percent of the system population, mostly in nonclinical and management positions.
Memorial Health System laid off fewer than 90 people, or less than 2 percent of its workforce.The Gulfport, Miss.-based health system said May 2 that most of the affected positions are nonclinical or management roles, and the majority do not involve direct patient care.
Monument Health laid off at least 80 employees, or about 2 percent of its workforce. The Rapid City, S.D.-based system said positions are primarily corporate service roles and will not affect patient services. Unfilled corporate service positions were also eliminated.
April
Habersham Medical Center in Demorest, Ga., laid off four executives. The layoffs are part of cost-cutting measures before the hospital joins Gainesville-based Northeast Georgia Health System in July, nowhaberbasham.com reported April 27.
Scripps Health is eliminating 70 administrative roles, according to WARN documents filed by the San Diego-based health system in March. The layoffs take effect May 8 and affect corporate positions in San Diego and La Jolla, Calif.
Trinity Health Mid-Atlantic, part of Livonia, Mich.-based Trinity Health, eliminated fewer than 40 positions, a spokesperson confirmed to Becker’s April 24. The layoffs represent 0.5 percent of the health system’s approximately 7,000-person workforce.
PeaceHealth eliminated 251 caregiver roles across multiple locations. The Vancouver, Wash.-based health system said affected roles include 121 from Shared Services, which supports its 16,000 caregivers in Washington, Oregon and Alaska.
Toledo, Ohio-based ProMedica plans to lay off 26 skilled nursing support staff. The layoffs, effective in June, affect 20 employees who work remotely across the U.S, and six who work at the ProMedica Summit Center in Toledo, according to a Worker Adjustment and Retraining Notification filed April 18. Most affected positions support sales, marketing and administrative functions for the skilled nursing facilities, Promecia told Becker’s.
Northern Inyo Healthcare District, which operates a 25-bed critical access hospital in Bishop, Calif., anticipates eliminating about 15 positions, or less than 4 percent of its 460-member workforce, by April 21, a spokesperson confirmed to Becker’s. The layoffs include nonclinical roles within support and administration, according to a news release. No further details were provided about specific positions affected.
West Reading, Pa.-based Tower Health is eliminating 100 full-time equivalent positions. The move will affect 45 individuals, according to an April 13 news release the health system shared with Becker’s. The other 55 positions are either recently vacated or involve individuals who plan to retire in the coming weeks and months.
Grand Forks, N.D.-based Altru Health is trimming its executive team as its new hospital project moves forward. The health system is trimming its executive team from nine to six and incentivizing 34 other employees to take early retirement.
Tacoma, Wash.-based Virginia Mason Franciscan Health laid off nearly 400 employees, most of whom are in non-patient-facing roles. The job cuts affected less than 2 percent of the health system’s 19,000-plus workforce.
Katherine Shaw Bethea Hospital in Dixon, Ill., will lay off 20 employees, citing financial headwinds affecting health organizations across the U.S. It will also leave other positions unfilled to reduce expenses amid rising labor and supply costs and reductions in payments by insurance plans. Affected employees largely work in administrative support areas and not direct patient care.
Danbury, Conn.-based Nuvance Health will close a 100-bed rehabilitation facility in Rhinebeck, N.Y., resulting in 102 layoffs. The layoffs are effective April 12, according to the Daily Freeman.
March
Charleston, S.C.-based MUSC Health University Medical Center laid off an unspecified number of employees from its Midlands hospitals in the Columbia, S.C. area. Division President Terry Gunn also resigned after the facilities missed budget expectations by $40 million in the first six months of the fiscal year, The Post and Courier reported March 30.
Winston-Salem, N.C.-based Novant Health laid off about 50 workers, including C-level executives, the health system confirmed to Becker’s March 29. The layoffs affected Jesse Cureton, the health system’s executive vice president and chief consumer officer since 2013; Angela Yochem, its executive vice president and chief transformation and digital officer since 2020; and Paula Dean Kranz, vice president of innovation enablement and executive director of the Novant Health Innovation Labs.
Penn Medicine Lancaster (Pa.) General Health eliminated fewer than 65 jobs, or less than 1 percent of its workforce of about 9,700, the health system confirmed to Becker’s March 30. The layoffs include support, administrative and executive roles, and COVID-19-related support staff, spokesperson John Lines said, according to lancasteronline.com. Mr. Lines did not provide a specific number of affected workers.
McLaren St. Luke’s Hospital in Maumee, Ohio, will lay off 743 workers, including 239 registered nurses, when it permanently closes this spring. Other affected roles include physical therapists, radiology technicians, respiratory therapists, pharmacists and pharmacy support staff, and nursing assistants. The hospital’s COO is also affected, and a spokesperson for McLaren Health Care told Becker’s other senior leadership roles are also affected.
Bellevue, Wash.-based Overlake Medical Center and Clinics laid off administrative staff, the health system confirmed to the Puget Sound Business Journal. The layoffs, which occurred earlier this year, included 30 workers across Overlake’s human resources, information technology and finance departments, a spokesperson said, according to the publication. This represents about 6 percent of the organization’s administrative workforce. Overlake’s website says it employs more than 3,000 people total.
Columbia-based University of Missouri Health Care is eliminating five hospital leadership positions across the organization, spokesperson Eric Maze confirmed to Becker’s March 20. Mr. Maze did not specify which roles are being eliminated saying that the organization won’t address individual personnel actions. According to MU Health Care, the move is a result of restructuring “to better support patients and the future healthcare needs of Missourians.”
Greensboro, N.C.-based Cone Health eliminated 68 senior-level jobs. The job eliminations occurred Feb. 21, Cone Health COO Mandy Eaton told The Alamance News. Of the 68 positions eliminated, 21 were filled. Affected employees were offered severance packages.
The newly merged Greensburg, Pa.-based organization made up of Excela Health and Butler Health System eliminated 13 filled managerial jobs. The affected employees and positions are from across both sides of the new organization, Tom Chakurda, spokesperson for the Excela-Butler enterprise, confirmed to Becker’s. The positions were in various support functions unrelated to direct patient care.
Crozer Health, a four-hospital system based in Upland, Pa., is laying off roughly 215 employees amid financial challenges. The system announced the layoffs March 15 as part of its “operational restructuring plan” that “focuses on removing duplication in administrative oversight and discontinuing underutilized services.” Affected employees represent about 4 percent of the organization’s workforce.
Philadelphia-based Penn Medicine is eliminating administrative positions. The change is part of a reorganization plan to save the health system $40 million annually, the Philadelphia Business Journal reported March 13. Kevin Mahoney, CEO of the University of Pennsylvania Health System, told Penn Medicine’s 49,000 employees last week that changes include the elimination of a “small number of administrative positions which no longer align with our key objectives,” according to the publication. The memo did not indicate the exact number of positions that were eliminated.
Sovah Health, part of Brentwood, Tenn.-based Lifepoint Health, eliminated the COO positions at its Danville and Martinsville, Va., campuses. The responsibilities of both COO roles will now be spread across members of the existing administrative team.
Valley Health, a six-hospital health system based in Winchester, Va., eliminated 31 administrative positions. The job cuts are part of the consolidation of the organization’s leadership team and administrative roles.
Marshfield (Wis.) Clinic Health System said it would lay off 346 employees, representing less than 3 percent of its employee base.
February
St. Mark’s Medical Center in La Grange, Texas, is cutting nearly 50 percent of its staff and various services amid financial challenges.
Roseville, Calif.-based Adventist Health plans to go from seven networks of care to five systemwide to reduce costs and strengthen operations. The reorganization will result in job cuts, including reducing administration by more than $100 million.
Arcata, Calif.-based Mad River Community Hospital is cutting 27 jobs as it suspends home health services.
Hutchinson (Kan.) Regional Medical Center laid off 85 employees, a move tied to challenges in today’s healthcare environment.
January
Oklahoma City-based OU Health eliminated about 100 positions as part of an organizational redesign to complete the integration from its 2021 merger.
Memorial Sloan Kettering Cancer Center announced it would lay off to reduce costs amid widespread hospital financial challenges. The layoffs are spread across 14 sites in New York City, and equate to about 1.8 percent of Memorial Sloan’s 22,500 workforce.
St. Louis-based Ascension completed layoffs in Texas, the health system confirmed in January. A statement shared with Becker’s says the layoffs primarily affected nonclinical support roles. The health system declined to specify to Becker’s the number of employees or positions affected.
Lebanon, N.H.-based Dartmouth Health is freezing hiring and reviewing all vacant jobs at its flagship hospital and clinics in an effort to close a $120 million budget gap.
Chillicothe, Ohio-based Adena Health System announced it would eliminate 69 positions — 1.6 percent of its workforce — and send 340 revenue cycle department employees to Ensemble Health Partners’ payroll in a move aimed to help the health system’s financial stability.
Ascension St. Vincent’s Riverside in Jacksonville, Fla., will end maternity care at the hospital, affecting 68 jobs, according to a Workforce Adjustment and Retraining Notification filed with the state Jan. 17. The move will affect 62 registered nurses as well as six other positions.
Visalia, Calif.-based Kaweah Health said it aimed to eliminate 94 positions as part of a new strategy to reduce labor costs. The job cuts come in addition to previously announced workforce reductions; the health system already eliminated 90 unfilled positions and lowered its workforce by 106 employees.
Oklahoma City-based Integris Health said it would eliminate 200 jobs to curb expenses. The eliminations include 140 caregiver roles and 60 vacant jobs.
Toledo, Ohio-based ProMedica announced plans to lay off 262 employees, a move tied to its exit from a skilled-nursing facility joint venture late last year. The layoffs will take effect between March 10 and April 1.
Employees at Las Vegas-based Desert Springs Hospital Medical Center were notified of layoffs coming to the facility, which will transition to a freestanding emergency department. There are 970 employees affected. Desert Springs is part of the Valley Health System, a system owned and operated by King of Prussia, Pa.-based Universal Health Services.
Philadelphia-based Jefferson Health plans to go from five divisions to three in an effort to flatten management and become more efficient. The reorganization will result in an unspecified number of job cuts, primarily among executives.
December
Pikeville (Ky.) Medical Center said it would lay off 112 employees as it outsources its environmental services department. The 112 layoffs were effective Jan. 1, 2023.
Southern Illinois Healthcare, a four-hospital system based in Carbondale, announced it would eliminate or restructure 76 jobs in management and leadership. The 76 positions fall under senior leadership, management and corporate services. Included in that figure are 33 vacant positions, which will not be filled. No positions in patient care are affected.
Citing a need to further reduce overhead expenses and support additional investments in patient care and wages, Traverse City, Mich.-based Munson Health said it would eliminate 31 positions and leave another 20 jobs unfilled. All affected positions are in corporate services or management. The layoffs represent less than 1 percent of the health system’s workforce of nearly 8,000.
November
West Reading, Pa.-based Tower Health on Nov. 16 laid off 52 corporate employees as the health system shrinks from six hospitals to four. The layoffs, which are expected to save $15 million a year, account for 13 percent of Tower Health’s corporate management staff.
St. Vincent Charity Medical Center in Cleveland closed its inpatient and emergency room care Nov. 11, four days before originally planned — and laid off 978 workers in doing so. After the transition, the Sisters of Charity Health System will offer outpatient behavioral health, urgent care and primary care.
October
Sioux Falls, S.D.-based Sanford Health announced layoffs affecting an undisclosed number of staff in October, a decision its CEO said was made “to streamline leadership structure and simplify operations” in certain areas. The layoffs primarily affect nonclinical areas.

https://mailchi.mp/27e58978fc54/the-weekly-gist-august-11-2023?e=d1e747d2d8

This week we had a conversation with a health system executive who has been wondering how to make the case to his board for expansion beyond the existing markets where the organization operates.
Like many, he’s confronting declining margin performance, and feeling pressure to combine with another system—joining the wave of cross-market consolidation that’s been dominating discussion among system CEOs recently.
His concern was that his locally governed board may be putting an artificial brake on growth, not seeing value of expansion beyond their market for the community they serve.
That’s a valid point—how does it help a Busytown resident if the local health system expands to operate in Pleasantville? Shouldn’t Busytown Health System just focus its resources and time on improving performance at home, and wouldn’t it represent a loss to Busytown if Pleasantville got investment dollars that could have been spent locally?
That’s a question raised by the “super-regional” or national strategies being pursued by many large systems today, and one worth thinking about.
Whenever a system grows outside its geography, there should be a solid argument that additional scale will reap returns for its existing operations, from better efficiency, better access to innovation and talent, better access to capital, or the like.
Those are legitimate reasons for out-of-market growth and consolidation, as long as the systems involved are diligent in pursuing them.
But local boards are right to hold executives accountable for making the case for growth, and ensuring that growth creates value for local patients and purchasers.
https://mailchi.mp/27e58978fc54/the-weekly-gist-august-11-2023?e=d1e747d2d8
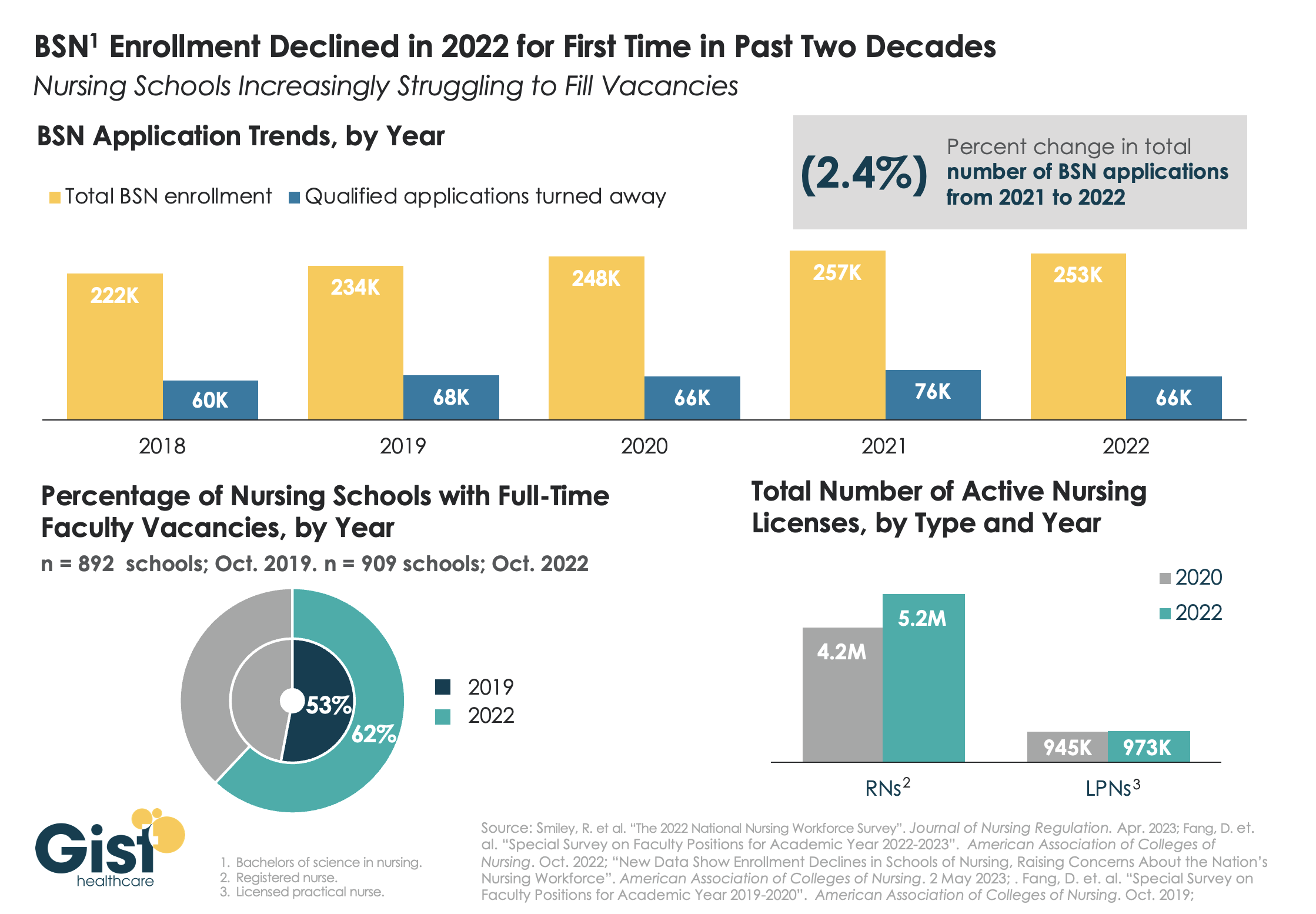
While last week’s graphic looked at how a wave of retirements has hit the nursing workforce, this week we take a look at the pipeline of nurses in training to fill that gap. In recent years, there has been a consistent stream of qualified applicants who want to become BSN nurses, but schools don’t have the capacity to admit them.
One reason: an ongoing shortage of nursing faculty, which recent retirements have exacerbated. The percentage of nursing schools with at least one full-time faculty vacancy grew from 53 percent in 2019 to 62 percent in 2022.
Looking at registered nurses (RNs), the number with active licenses has continued to grow at a much higher rate than the supply of licensed practice nurses (LPNs) with active licenses.
The relatively small LPN workforce is especially significant, given rising interest in team-based nursing care, which aims to utilize a higher number of LPNs, supervised by RNs and BSNs.
Expanding training programs with an eye toward the skills and mix needed to deliver team-based care will be critical to ensuring a stable, efficient nursing workforce for future decades.
