At a meeting last week, a surgeon (and loyal Weekly Gist reader) shared his thoughts on our recent coverage of research evaluating physician earnings, and analysis comparing the incomes of American doctors with those in other Western countries.
(The gist: unsurprisingly, American doctors make more money—and one of the primary reasons is that there are simply fewer physicians per capita here than in most other Western nations.)
His retort: “It sounds like you’re rooting for doctors to get paid less!” Given the number of emails we received on the piece, it’s clear that the topic touched a nerve.
A few doctors pointed out the limitations of simple supply and demand in driving physician salaries. Of course there are important structural differences between our delivery and payment system and those in other nations: fee-for-service versus global payment; length of training and degree of student debt; and relative salaries of specialists versus primary care physicians, just to name a few.
But if anything, the effects of supply and demand are amplified in a more market-driven system like the US. Plus, there are factors, like regulation of the number of residency training slots, that keep supply artificially low—and physician incomes in competitive specialties high.
At a high level, the data do show that prices—both physician and hospital—are higher in the US than other countries, whereas utilization is roughly similar.
Over time, we’d expect that there will be continued price pressure driving down doctors’ incomes, but large swings in physician salaries will take a generation or more to emerge.
And should physicians experience more salary pressure, expect more of them to seek additional sources of entrepreneurial and investment income—further increasing the spread between the lowest- and highest-paid doctors.
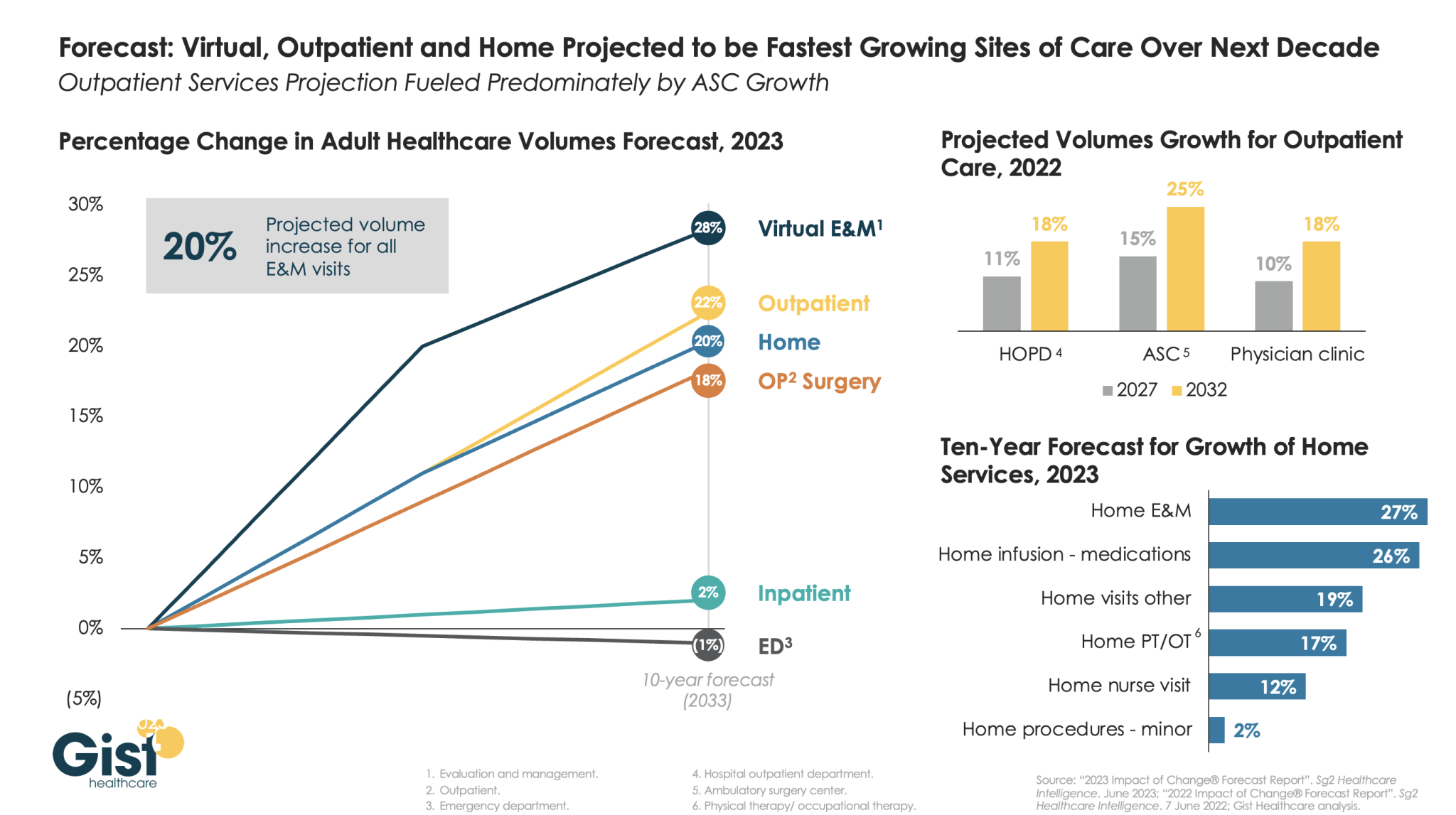
The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
An investigative piece published this month by ProPublica documents how it came to be that nearly 60 percent of healthcare providers report being charged fees to receive electronic payments from insurers.
The fees, which can be as high as five percent of total reimbursement, were briefly forbidden by the Centers for Medicare and Medicaid Services (CMS), before the agency reversed its policy in 2018. The article follows one dogged physician’s efforts to uncover why CMS allows these fees. His voluminous stream of public records requests revealed a highly coordinated pressure campaign, mounted by the insurance industry through one particularly influential regulator-turned-lobbyist.
While the American Medical Association has urged the Biden administration to protect physicians from these fees, and the Veterans Health Administration is refusing to pay them, CMS is so far maintaining the position that electronic-payment claims-processing fees are permissible.
The Gist: Through partnerships with payment companies, who charge double the average fees of electronic bank transfers and share the spoils of their “virtual credit cards”, insurers are essentially using the same business model as credit card companies, skimming revenue from physician payments just as Visa and MasterCard do to merchants.
With the increasing consolidation of both insurers and claims processors, physicians are left with little recourse but to pay these fees, as nonelectronic payments come with infrastructure costs and payment delays.
While the shift to electronic payments spurred on by the Affordable Care Act was supposed to improve efficiency, this article offers yet another example of how efficiency gains can be captured by industry middlemen before they can be translated into provider and consumer benefits.
Blue Shield of California announced a plan to diversify its pharmacy benefit management (PBM) contracts in a bid to improve transparency and reduce costs.
Instead of relying on Woonsocket, RI-based CVS Health’s Caremark as its sole PBM, the health plan and its 4.8M members will be served by five companies, including Amazon Pharmacy for at-home deliveries, Mark Cuban Cost Plus Drugs Company (MCCPDC) for a transparent pricing model, and Prime Therapeutics for negotiations with pharmaceutical companies.
Caremark will remain responsible for Blue Shield’s specialty pharmacy needs, which CVS noted in an investor filing represents over 50 percent of nationwide pharmacy benefit spending.
Blue Shield intends to implement this new system by 2025, and is targeting savings of $500M annually, which translates to 10 to 15 percent of its current spending.
The Gist: Whether Blue Shield saves money with this initiative depends on the whether the benefit of competition in its PBM contracts outweighs the costs of more complex coordination between vendors.
Keeping half of its business tied up with CVS through specialty pharmacy will further limit the potential impact. Nonetheless, it’s noteworthy that pharmacy disruptors like Amazon and MCCPDC have found a major health plan willing to work with them.
Consumers, employers, payers without PBMs, and members of Congress are increasingly dissatisfied with the current pharmacy benefit market structure, and Blue Shield’s move could serve as a catalyst for future shakeups.
As 41% of American adults face medical debt, residents of this southern Colorado city contend their local nonprofit hospitals aren’t providing enough charity care to justify the millions in tax breaks they receive.
The two hospitals in Pueblo, Parkview Medical Center and Centura St. Mary-Corwin, do not pay most federal or state taxes. In exchange for the tax break, they are required to spend money to improve the health of their communities, including providing free care to those who can’t afford their medical bills. Although the hospitals report tens of millions in annual community benefit spending, the vast majority of that is not spent on the types of things advocates and researchers contend actually create community benefits, such as charity care.
And this month, four U.S. senators called on the Treasury’s inspector general for tax administration and the Internal Revenue Service to evaluate nonprofit hospitals’ compliance with tax-exempt requirements and provide information on oversight efforts.
The average hospital in the U.S. spends 1.9% of its operating expenses on charity care, according to an analysis of 2021 data by Johns Hopkins University health policy professor Ge Bai. Last year, Parkview provided 0.75% of its operating expenses, about $4.2 million, in free care.
Centura Health, a chain of 20 tax-exempt hospitals, reports its community benefit spending to the federal government in aggregate and does not break out specific numbers for individual hospitals. But St. Mary-Corwin reported $2.3 million in charity care in fiscal year 2022, according to its state filing. The filing does not specify the hospital’s operating expenses.
The low levels of charity care have translated into more debt for low-income residents.
About 15% of people in Pueblo County have medical debt in collections, compared with 11% statewide and 13% nationwide, according to 2022 data from the Urban Institute. Those Puebloans have median medical debt of $975, about 40% higher than in Colorado and the U.S. as a whole. And all of those numbers are worse for people of color.
“How far into debt do people have to go to get any kind of relief?” said Theresa Trujillo, co-executive director at the Center for Health Progress’ Pueblo office. “Once you understand that there are tens of millions of dollars every single year that hospitals are extracting from our communities that are meant to be reinvested in our communities, you can’t go back from that without saying, ‘Oh my gosh, that is a thread we need to pull on.’”
Trujillo is organizing a group of fed-up residents to engage both hospitals on their community benefit spending. The group of at least a dozen residents believe the hospitals are ignoring the needs identified by the community — things like housing, addiction treatment, behavioral health care, and youth activities — and instead spending those dollars on things that mainly benefit the hospitals and their staffs.
For the fiscal year ending June 2022, with total revenue of $593 million, Parkview reported $100 million in community benefit spending. But most of that — more than $77 million — represented the difference between the hospital’s cost of providing care and what Medicaid paid for it.
IRS guidelines allow hospitals to claim Medicaid shortfall as a community benefit, but many academics and health policy experts argue such balance sheet shifts aren’t the same as providing charity care to patients.
Parkview also reported $4.7 million for educating its medical staff and $143,000 in incentives to recruit health professionals as community benefit. The hospital spent only $44,000 on community health improvement projects, which appear to have consisted mainly of launching a new mobile app to streamline appointments and referrals.
Meanwhile, the hospital recently spent $58 million on a new orthopedic facility and $43 million on a new cancer center. Parkview also wrote off $39 million in bad debt in fiscal 2022, although that is different from charity care. The bad debt is money the hospitals tried to collect from patients and ultimately decided they’d never get. But by that time, those patients would likely have been sent to collections and potentially had their credit damaged. And outstanding debt often keeps patients from seeking other needed care.
There is a disconnect between what the community said its biggest health needs were and where Parkview directed its spending. The hospital’s community needs assessment pegged access to care as the top concern, and the hospital said it launched the phone app in response.
The second-largest perceived health need was addressing alcohol and drug use. Yet, the only initiative Parkview cited in response was posting preventive health videos online, including some on alcohol and drug use. Meanwhile, the hospital shut down its inpatient psychiatric unit.
Parkview declined to answer questions about its charity care spending, but hospital spokesperson Todd Seip emailed a statement saying the hospital system “has been committed to providing extensive charity care to our community.”
Seip noted that 80% of Parkview’s patients are covered by Medicare or Medicaid, which pay lower rates than commercial insurance. The hospital posted a net loss of $6.7 million in the 2022 fiscal year, although its charity care wasn’t appreciably higher in previous years in which it posted a net gain.
Centura St. Mary-Corwin reported $16 million in Medicaid shortfall and $2 million in medical staff education in 2022, according to its state filing. The hospital spent about $38,000 for its community health improvement projects, primarily on emergency medical services outreach programs in rural areas. The hospital provided another $96,000 in services, mainly to promote covid-19 vaccination.
Centura also declined to answer questions about its charity care spending. Hospital spokesperson Lindsay Radford emailed a statement saying St. Mary-Corwin was aligning its community health needs assessment process with the Pueblo Department of Public Health and Environment “to develop shared implementation strategies for our community benefit funds, ensuring the resources are targeting the highest needs.”
Trujillo questioned how the hospital has conducted its community health assessments, relying on a social media poll to identify needs. After community members identified 12 concerns, she said, hospital leaders chose their priorities from the list.
“They talk about a community garden like they’re feeding the whole south side of the community,” Trujillo said. The hospital established a community garden in 2021, with 20 beds that could be adopted by residents to grow vegetables. Trujillo did praise the hospital for converting part of its building into dorms for a community college nursing program.
Trujillo’s group has spent much of the summer researching hospital charity spending and showing up at public meetings to have their views heard. They are working to gain seats on hospital and other state boards that influence how community benefit dollars are spent, and are urging hospitals to reconfigure their boards to better represent the demographics of their communities.
“We’ve made folks now aware that we want to be a part of those processes,” Trujillo said. “We’re willing to help them reach deeper into the community.”
Tax-exempt hospitals have been under increased state scrutiny for their charitable spending, especially after the Affordable Care Act and Medicaid expansion drove down the uninsured rate. That in turn cut the amount of care hospitals had to provide without being paid, potentially freeing up money to help more people without insurance or with high-deductible plans.
In Colorado, hospitals’ charity care spending and bad debt write-offs dropped from an average of $680 million a year in the five years prior to the ACA being fully implemented in 2014 to an average of $337 million in the years after, according to the Colorado Healthcare Affordability and Sustainability Enterprise Board, a state advisory group.
In states like Colorado, which used federal funding to expand the number of people covered by Medicaid, hospitals shifted more of their community benefit spending to cover Medicaid reimbursement shortfalls.
A January report from Colorado’s Department of Health Care Policy & Financing concluded that payments from public and private health plans help the state’s hospitals make more than enough money to offset lower Medicaid rates and still turn a profit while providing more true charity care.
Colorado has enacted two bills in the past five years to increase the transparency of hospitals’ charitable efforts with new reporting requirements.
“I think overall, we’re pleased with the amount of money that hospitals are reporting they spent,” said Kim Bimestefer, the executive director of the Department of Health Care Policy & Financing. “Is that money being expended in meaningful ways, ways that improve health and well-being of the community? Our reports right now can’t determine that.”
Payers have historically been the financial support for patients receiving medical care. Through scale, predictive analytics and actuarial insights, large insurers have been able to smoothly calibrate pricing and earnings so that members have health coverage no matter the economic environment. Over time different insurance products such as Medicare Advantage, managed Medicaid, Commercial insurance, and self-funded benefits were created to provide optionality for consumers. The demand for more services under one umbrella has resulted in six large public insurers, known collectively as the “Nationals.” As for-profit public entities, these organizations have utilized M&A to drive growth by acquiring smaller health plans. This horizontal consolidation has grown membership and diversified their membership geographically, as well as by line of business. The diversification enables these Nationals to reduce volatility in earnings, which eases concerns of public investors, while sustaining top line growth each year. However, with the changing tide in healthcare business models, payers have begun to look elsewhere for new growth opportunities.
The emergence of value-based care has garnered significant interest within the healthcare ecosystem. Consumers of healthcare value their personalized interactions with their providers / doctors and are typically somewhat agnostic about their payer. The payers have come to the realization that to further drive profits, they must create stickiness with their members by aligning with the providers that are delivering the care. Collaboration between the payers and providers will help increase the efficiencies in care management and drive unnecessary costs out the care delivery process, when fully integrated. By being “closer” to the patients, payers can use the data from providers to create valuable insights that proactively address a patient’s needs before catastrophic, high-cost treatments are required. This trend of vertical integration, turning payers to pay-(pro)viders, has started to play out and should be beneficial to patients, payers, providers, investors, and U.S. healthcare as a whole.
UnitedHealthcare recently closed its $5.4 billion acquisition of LHC Group in February 2023. LHC Group provides home health solutions and community-based care to over 12 million patients annually in their homes. This acquisition is UnitedHealthcare’s opportunity to increase patient engagement for the high acuity populations that LHC Group traditionally services. UnitedHealthcare also announced the acquisition of Amedisys, another home health and hospice provider, for $3.3 billion in 2023. UnitedHealthcare will be able to leverage the expertise from these two organizations, while utilizing its data analytical capabilities to synchronize care efficiently and effectively. As the U.S. population continues to age, optimizing care for seniors will be a key focal point for the healthcare services industry.
CVS Health acquired Oak Street Health, a primary care provider that specializes in value-based care, for $10.6 billion in 2023. This acquisition will help CVS Health address costs and patient health in underserved communities that Oak Street Health currently services. CVS Health also acquired Signify Health, a technology and services company that focuses on care at home, in 2023 for $8 billion. The acquisitions of Oak Street Health and Signify Health will expand CVS Health’s healthcare delivery arm as it looks to become a one-stop shop for all patient’s needs.
As other payers see the value, both in better health outcomes and economics, created through the vertical integration of services by their competitors, they too will follow the trend. The definition of the payer will continue to evolve, and healthcare consumers will increasingly receive lower cost of care, greater accessibility to care and preferential outcomes into the future. It will be exciting to see which pay-vider acts next and capitalizes on this opportunity.
Shorter contracts, noncompete agreements and increased emphasis on value-based components are among the shifts occurring in physician contracts as hospitals and medical groups build recruitment pipelines and offer incentives to retain physicians.
Changes in how physician contracts are layered echoes a trend that has been occurring in the labor market itself. Physicians are increasingly opting for employed opportunities and contracts within those models are changing accordingly.
From 2019 to 2021, more than 108,700 physicians left private practice for employment opportunities, with 58,200 physicians joining hospitals. About three in four physicians are now employed by hospitals, health systems, private-equity-owned groups, payers or other corporate entities.
The rising costs of private practice, increasing administrative burdens and reimbursement hurdles are also making solo practice a challenging model for many physicians today.
Fewer large medical groups are offering salaries with production bonuses, according to an AMN Healthcare report on physician and advanced practitioner recruiting incentives. The company’s 2017 report found that 75 percent of contracts featured a salary with production bonus, while only 17 percent had a straight salary.
Some medical groups have stopped offering production bonuses because they found that the straight salary model has less ambiguity and is less likely to cause friction with physicians, according to the report.
AMN also found that a relatively high percentage of academic medical centers do not offer the salary with production bonus model, which may account for the decline in the use of this compensation structure in its report.
Income guarantees, which are essentially loans that must be repaid generally (but can be forgiven over time) are used to establish physicians in solo or small independent practices. Income guarantees were once the standard contract model, but as the number of private practices has declined, so has the use of income guarantees, according to the report..
Health systems continue to rethink physician contracts as healthcare continues its shift away from fee for service, but challenges remain when it comes to compensation in these models. Systems at the forefront of this shift are developing ways to incentivize physicians in value-based care as the trend towards team-based compensation gains traction and fosters collaboration among providers.
Epic was named the top EHR for acute care hospitals with 251 beds or more by Black Book Research.
The research group based its results on surveys of 18 performance indicators conducted between the second quarter of 2022 and the third quarter of 2023.
Here are the top six EHRs for large hospitals, according to the report:
“I know that I have less to live than I have lived.
I feel like a child who was given a box of chocolates. He enjoys eating it, and when he sees that there is not much left, he starts to eat them with a special taste.
I have no time for endless lectures on public laws – nothing will change. And there is no desire to argue with fools who do not act according to their age. And there’s no time to battle the gray. I don’t attend meetings where egos are inflated and I can’t stand manipulators.
I am disturbed by envious people who try to vilify the most capable to grab their positions, talents and achievements.
I have too little time to discuss headlines – my soul is in a hurry.
Too few candies left in the box.
I’m interested in human people. People who laugh at their mistakes are those who are successful, who understand their calling and don’t hide from responsibility. Who defends human dignity and wants to be on the side of truth, justice, righteousness. This is what living is for.
I want to surround myself with people who know how to touch the hearts of others. Who, through the blows of fate, was able to rise and maintain the softness of the soul.
Yes, I hustle, I hustle to live with the intensity that only maturity can give. I’ll eat all the candy I have left – they’ll taste better than the ones I already ate.
My goal is to reach the end in harmony with myself, my loved ones and my conscience.
I thought I had two lives, but it turned out to be only one, and it needs to be lived with dignity.”
Brilliant Anthony Hopkins
and free interpretation of Mario de Andrade’s poem