The Federal Reserve just raised interest rates by three-quarters of a percentage point, the biggest single increase in interest rates since 1994. It’s another move in the Fed’s effort to tackle the fastest inflation in four decades.
I understand the Fed’s urgency, but it has entered dangerous territory. If the Fed continues down this path – as it has signaled it will – the economy will be plunged into a recession. Every time over the last half century the Fed has raised interest rates this much and this quickly, it has caused a recession.
Besides, interest rate increases will not remedy the major causes of the current inflation – huge pent-up worldwide demand from two years of pandemic, shortages of goods and services responding to that demand, Putin’s war in Ukraine, and big profitable corporations with enough pricing power to use inflation as a cover for pushing up prices even further.
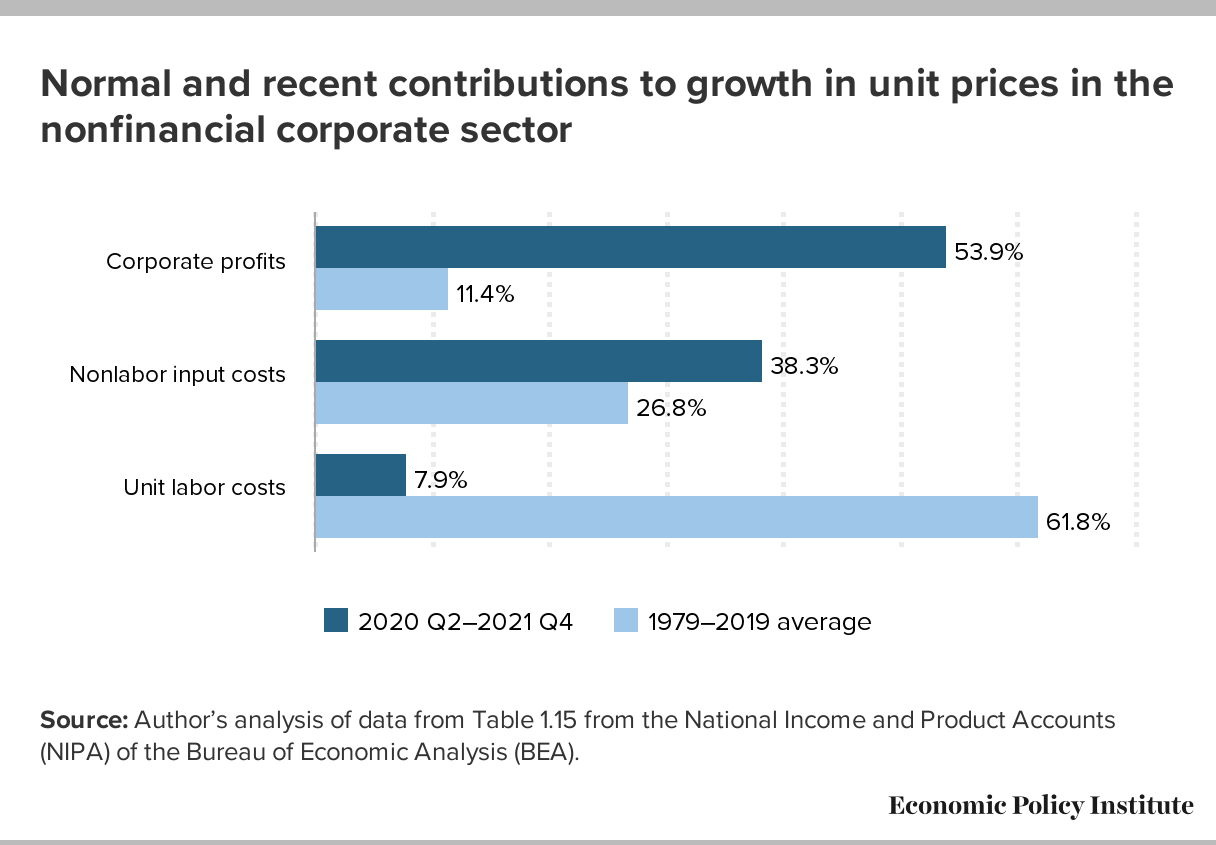
The Fed assumes that price increases are being driven by wage increases — so-called “wage-price inflation.” That’s incorrect. Wages are lagging behind inflation. A more accurate description of what we’re now seeing might be called “profit-price inflation” — prices driven upward by corporations seeking increased profits. (See chart below, from the Economic Policy Institute.)
A recession will be especially harmful to people who are most vulnerable to downturns in the economy — who are the first to be fired (and last to be hired again when the economy turns upward): lower-wage workers, disproportionately women and people of color.
Social factors impact a person’s health and their potential health outcomes. While this has long been discussed (especially by folks of color, individuals with lived experiences, and those in public health), it is finally now getting deserved mainstream attention, including by health insurers.
Medicare Advantage (MA) — a program that offers private plan alternatives to traditional Medicare — is one key player looking at social determinants of health. It’s a good thing, too; an estimated 42% of the Medicare population are enrolled in MA plans, and that share grows each year. MA plans have more flexibility in offering supplemental benefits and services, some of which can address social determinants of health.
In 2018, the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act passed with bipartisan support and marked a substantial shift in MA policy by including acknowledgment of the role of social determinants of health. It allows even greater flexibility for MA plans to help with the very conditions that impact how a person lives, such as providing financial assistance for nutritional needs, transportation to appointments, caregiver support, and even home construction projects. Interestingly, it does not mandate coverage, so it is still dependent on what plans an individual has access to and how health plans are choosing to move forward with this freedom.
The problem is, however, that most individuals aren’t eligible for Medicare until age 65 (there are some exceptions). If we wait until Medicare eligibility to act on social determinants of health, are we waiting too long?
The short answer is yes. Although addressing social determinants of health in the Medicare-eligible population is important, what we know suggests that more could be done earlier.
Why are social determinants important in Medicare Advantage?
Chronic disease is a significant issue among Medicare-eligible individuals, and one that’s exacerbated by social determinants of health. There are substantial implications for both beneficiaries and MA plans. For beneficiaries, chronic disease affects not only their quality of life, but also their wallet. From the plans’ perspectives, the presence of comorbid chronic diseases is a significant differentiator between so called “high cost” beneficiaries and those who are not.
Current MA enrollment trends also point to the need to sharpen the focus on social determinants of health. Although they make up a minority of MA enrollees, persons of color are enrolling in MA plans at a breakneck pace: especially among Black people, dual enrollees, and people living in disadvantaged neighborhoods.
Historically, these are folks most negatively impacted by social determinants of health, and the likelihood of poor health outcomes is only compounded when enrollees reside in disadvantaged neighborhoods. These are neighborhoods commonly characterized by high concentrations of poverty, crime, and harmful environmental exposures compounded by limited resources to support economic and social well-being, and research has consistently found strong associations between neighborhood disadvantage and health risks and outcomes.
Health systems must do more about social determinants earlier in life
Social determinants of health affect us all — regardless of age. Until recently, they have received relatively little attention from insurers.
It is difficult though to discern the extent that these actions are altruistic or opportunistic, especially when they can technically be both. While that might not be the worst thing, it does matter if it leaves out the very people it should be helping.
Let’s consider internet access, for example. If a patient isn’t connected to the web, they can’t participate in a telehealth visit, leaving in-person care as the only option. In a world where telehealth visits are reimbursed at a fraction of the in-person rate, there are substantial cost savings (read: profit) associated with facilitating and promoting virtual care. Critics have also pointed out that most of these steps can be attributed to insurers’ philanthropic apparatuses as opposed to any substantive change or innovation in member benefits.
What is also becoming readily apparent, is that while telehealth use is increasing, it does not make care accessible for everyone. It could even serve to increase disparities if it is not done properly.
However, administrative hurdles and societal stigma can challenge people’s willingness to participate in these programs no matter how beneficial they might be. We should all be asking what more the health system — providers, payers, and government — should be doing to improve social determinants of health earlier in life.
The CHRONIC Care Act has the potential to mitigate some of these harmful impacts of long-standing structural inequities by providing greater flexibility for plans to cover non-medical needs. The law illustrates that policymakers believe that health insurers should do more to address social determinants of health. Perhaps they should also focus on how plans can address these social factors earlier in the life cycle as well.
RWJBarnabas Health on Tuesday called off its attempt to acquire St. Peter’s Healthcare System in New Brunswick, N.J., days after the Federal Trade Commission sued to block the proposed transaction.
Currently there is a resolution HR 7995 in the U.S. House of Representatives, introduced late last week, that will decrease prior authorization delays for patients awaiting care.
The very manual, time-consuming processes, for prior authorization, burden physicians, physician practices, and hospitals while diverting valuable resources away from direct patient care. HR 7995 was referred to the Committee on Ways and Means in addition to the Committee on Energy and Commerce.
Now that the framework of this bill is still being worked, it is crucial to get in front of legislators and let them know that you support this legislation that will decrease prior authorization delays ensuring continuity of care to patients because it:
Exempts qualifying physicians from prior authorization requirements under Medicare Advantage (MA) (providing for a “Gold Card” status for physicians that consistently meet prior authorization requirements).
Allows physicians to appeal “Gold Card” revocation from insurers that are wrongly decided.
Requires Secretary of HHS to issue rules on MA plans.
Pandemic pressures and a high debt load are among the factors stalling Franklin, Tenn.-based Community Health Systems’ financial turnaround, Bloomberg Law report June 8.
CHS, an 83-hospital system, is facing many of the same challenges as other health systems across the U.S., including a surge in labor expenses in the first quarter of this year. The higher expenses and a COVID-19 surge that negatively impacted operating revenues dragged down the company’s earnings in the first quarter of this year. CHS ended the first three months of 2022 with a net loss of $1 million.
CHS leaders expect some of the pressures to continue through the second quarter.
“Moving through the second quarter and the remainder of the year, we anticipate contract labor rates to remain elevated, however, we expect our operational momentum to continue, as we anticipate capturing deferred healthcare demand, benefitting from recent strategic investments, and continuing the execution of the company’s margin improvement program,” Tim Hingtgen, CEO of CHS, said in an April 27 earnings release.
The company cut its earnings forecast in April when it released results for the first quarter, and it has seen its bonds and stock slide since March, according to Bloomberg Law.
Shares of CHS closed June 8 at $5.16, down from $5.25 the day before.
Numerous viruses that were seemingly dormant during the pandemic are returning in new and atypical ways, CNBC reported June 10.
Flu, respiratory syncytial virus, adenovirus, tuberculosis and monkeypox are among the viruses that have recently surged or exhibited unusual behaviors.
The U.S. saw extremely mild flu seasons in 2020-21 and 2021-22, likely due to high rates of mask-wearing, social distancing and other COVID-19 prevention measures. However, flu cases started to rise this February and continued to climb through the spring as more public health measures receded.
“We’ve never seen a flu season in the U.S. extend into June,” Scott Roberts, MD, associate medical director for infection prevention at Yale New Haven (Conn.) Hospital, told CNBC. “COVID has clearly had a very big impact on that. Now that people have unmasked [and] places are opening up, we’re seeing viruses behave in very odd ways that they weren’t before.”
Washington state is also reporting its most severe tuberculosis outbreak in 20 years, while the world is grappling with a monkeypox outbreak that’s affected more than 1,000 people.
These viruses, suppressed during the pandemic, now have more opportunities to spread as people resume daily life, become more social and travel more. Society, as a whole, also has less immunity against the viruses after two years of reduced exposure to them, according to the report.
The pandemic has also boosted surveillance efforts and public interest in other outbreaks, experts say.
“COVID has raised the profile of public health matters so that we are perhaps paying more attention to these events when they occur,” Jennifer Horney, PhD, professor of epidemiology at the University of Delaware in Newark, told CNBC.
The popularity of travel nursing is leaving healthcare facilities and the companies serving them susceptible to misclassification accusations and joint-employer disputes, Bloomberg Law reported June 14.
Providers should read contracts to understand who is liable if a travel nurse sues a healthcare facility and staffing company, according to the report. Even if agreements state that a hospital is not a temporary employee’s employer, courts may decide it’s a joint employer. If they are a joint employer, they may have to pay legal fees if a staffing agency is sued.
If classified as an employer, healthcare facilities may be bound by labor laws that didn’t apply to independent contractors. In California, for example, employers are required to pay part of a worker’s cell phone bill if a phone is needed for the job.
“Given the already serious issues with many of these healthcare workers feeling overwhelmed and underpaid, they’re going to turn these questions not just to the individual hospitals, but potentially also to the companies that are hosting these platforms,” Sonya Rosenberg, a labor and employment partner at Neal Gerber Eisenberg, told Bloomberg Law.
This week’s contributor is Paula Chatterjee, a physician and assistant professor at the Perelman School of Medicine at the University of Pennsylvania. Her research focuses on improving the health of low-income patients and evaluating policies related to safety-net health care delivery and financing.
Low-income patients face many barriers to care, one of which is the high cost of prescription medications. The 340B program lets certain hospitals and clinics (like federally qualified health centers) receive discounts on outpatient medications. They can then use those savings to provide medication and additional care for little to no charge to low-income patients. However, policymakers and other stakeholders have raised concerns that the 340B program might not be reaching the patients it was designed to support.
A recent paper in the American Journal of Managed Care by Sayeh Nikpay*, Gabriela Garcia, Hannah Geressu and Rena Conti sheds light on one of the latest examples of 340B mistargeting: so-called contract pharmacies. These are retail pharmacies that fill 340B prescriptions and split the savings with the hospital or clinic. These relationships have been on the rise, with hospitals and clinics arguing they make it more convenient for patients to get their prescriptions. Given their growth, the authors looked at whether contract pharmacies were more likely to open up in areas where low-income and uninsured people live.
They found the pattern was different for pharmacies contracting with 340B clinics vs. 340B hospitals:
The number of counties with a pharmacy contracted with a 340B clinic grew from 20.8% to 64.8% over the past decade. Counties with higher poverty rates were more likely to gain a clinic-contracted pharmacy.
The number of counties with hospital-contracted pharmacies grew much more (from 3.2% to 76.3%), but those counties had fewer uninsured residents and were less likely to be medically underserved.
The researchers acknowledge that counties may be an imperfect geographical area to represent a pharmacy’s market and that they were unable to collect information on how many (if any) 340B prescriptions a pharmacy actually filled.
Nonetheless, their results reveal a mismatch between where the 340B program is growing and where low-income patients live, especially for pharmacies contracting with 340B hospitals. The authors argue that any 340B policy changes should take these differences between hospitals and clinics into account.
Despite decades of policies designed to bolster the safety-net, it remains perennially reliant on a patchwork of subsidies that are often mistargeted.
This study adds to a growing body of work highlighting the opportunity to improve the 340B program so that it achieves its intended goal of improving access for low-income patients.
This week’s contributor is Aditi Sen, the Director of Research and Policy at the Health Care Cost Institute. Her work uses HCCI’s unique data resources to conduct analyses that inform policy to promote a sustainable, accessible and high-value health care system.
High health care prices in the U.S. make it hard for people to access care, difficult for employers to provide insurance, and challenging for policymakers to balance health care spending with other budgetary priorities. That’s why it’s important to understand what drives prices higher and identify policies to keep prices from getting so high.
In a new paper in Health Affairs, Vilsa Curto, Anna Sinaiko and Meredith Rosenthal examined whether hospital and health systems’ acquisition of and contracting with physician practices – two forms of what is often called vertical integration – has led to higher prices for physician services. The researchers combined four sets of data from Massachusetts from 2013-2017 for their analysis.
They found that:
The percent of physicians who joined health systems grew meaningfully: The percent of primary care physicians who remained independent dropped from 42% in 2013 to 31.5% in 2017, and the percent of independent specialists fell from 26% to 17%.
Over this same period, prices for physician services rose. Price increases were especially large – 12% for primary care physicians and 6% for specialists – when physicians joined health systems that had a high share of admissions in their area.
This study stands out for several reasons. First, it shows vertical integration drives up health care prices. Second, the authors highlight actions states can and are considering taking to monitor and curb vertical integration, including antitrust enforcement and enacting laws to promote competition.
Finally, the Massachusetts data allow the public to better appreciate what’s happening across the state. Many earlier studies on health care consolidation have been limited to a subset of insurers, physicians or patients. Massachusetts is a leader when it comes to creating and sharing its data thanks to its all-payer claims database, which pulls together all the health care bills from private insurers and public programs like Medicare and Medicaid in the state. This critical information helps to illuminate patterns of care and prices and connect them to issues like consolidation and competition.Neither the federal government nor most states track how vertical integration mergers influence health care prices.
As these findings demonstrate, acquisitions and other forms of vertical integration impact what people pay for health care services. Given that prices in this sector continue to climb, this paper underscores the need for more state and national data to understand the downstream effects on all of us who use and participate in the U.S. health care system.