Trump administration officials deny there will be availability issues, but others say problems are possible in the second quarter.
Pfizer has told the Trump administration it cannot provide substantial additional doses of its coronavirus vaccine until late June or July because other countries have rushed to buy up most of its supply, according to multiple individuals familiar with the situation.
That means the U.S. government may not be able to ramp up as rapidly as it had expected from the 100 million doses of the Pfizer vaccine that it purchased earlier this year, raising questions about whether it can keep to its aggressive schedule to vaccinate most Americans by late spring or early summer.
Trump administration officials denied there would be availability issues in the second quarter, citing other vaccines in the pipeline — most immediately, Moderna’s, also expected to be approved in coming weeks. Both vaccines are two-dose regimens, so the 100 million doses purchased of each would cover 50 million people each.
“I’m not concerned about our ability to buy vaccines to offer to all of the American public,” Gen. Paul Ostrowski, who oversees logistics for Operation Warp Speed, the government’s initiative to expedite vaccine development, said in an interview Monday. “It’s clear that Pfizer made plans with other countries. Many have been announced. We understand those pieces.”
But several officials knowledgeable about the contracts said that supplies from other companies may be insufficient to fill the gap.
Last summer, Pfizer officials had urged Operation Warp Speed to purchase 200 million doses, or enough of the two-shot regimen for 100 million people, according to people knowledgeable about the issue who spoke on the condition of anonymity because they weren’t authorized to discuss the situation. But the Warp Speed officials declined, opting instead for 100 million doses, they said. The New York Times first reported that federal officials passed on the opportunity when Pfizer offered to sell more doses.
“Anyone who wanted to sell us … without an [FDA] approval, hundreds of millions of doses back in July and August, was just not going to get the government’s money,” said a senior administration official.
It was only last weekend, with a Food and Drug Administration clearance expected any day, that federal officials reached back out to the company asking to buy another 100 million doses. By then, Pfizer said it had committed the supply elsewhere and suggested elevating the conversation to “a high level discussion,” said a person familiar with the talks.
Pfizer said the company might be able to provide 50 million doses at the end of the second quarter, and another 50 million doses in the third quarter, the individuals said.
The government had a different type of contract with Pfizer than with other companies involved with Operation Warp Speed. Pfizer was the only company that did not take government money for research and development, which meant U.S. officials have had less insight into its decisions than it does with the other companies, said a senior administration official familiar with the matter who spoke on the condition of anonymity.
The contract between the government and Pfizer stipulated that if Pfizer’s vaccine was successful and received authorization from the FDA, the U.S. government would purchase 100 million doses at a set price.
Pfizer spokeswoman Amy Rose declined to confirm any information about the company’s discussions with the government, and said that beyond the first 100 million doses the U.S. has already secured, a separate agreement would have to be negotiated.
President Trump is expected to sign an executive order Tuesday that would prioritize vaccinating Americans before providing doses to other countries, according to a senior administration official who requested anonymity because he was not authorized to speak about the plans. Fox News first reported the executive order. It is not clear whether the order is related to the Pfizer supply issue, or whether the president can prevent an American company from fulfilling lawful contracts with other countries.
“The executive order reaffirms to the American people that we are going to put America first,” said a senior administration official, who spoke on the condition of anonymity because he was not authorized to discuss the issue publicly.
The order will be announced as part of a White House “vaccine summit” designed to highlight the administration’s accomplishments on vaccines.
The vaccine by Pfizer and German biotech firm BioNTech is expected to receive emergency authorization from the FDA in the next several days, and Moderna is lined up for likely clearance shortly after that. Shipments of the vaccines will begin within 24 hours of the approvals, federal officials have said.
Warp Speed officials hope that other companies with promising vaccine candidates will supplement the supply in the near future, but some are still conducting late-stage clinical trials, while others haven’t begun them.
That means it could be several weeks to months before they are ready to apply to the FDA for clearance. One of the companies, AztraZeneca recently reported encouraging vaccine data, but experts raised questions about it and what it meant about the efficacy of the vaccine.
Moncef Slaoui, chief science adviser to Warp Speed, said in an interview Monday that the U.S. government strategy was to spread its risk widely over many different types of vaccines from different manufacturers. He declined to comment on negotiations with any company, but said he did not believe there would be any kind of vaccine “cliff,” where the available doses would fall off sharply.
Slaoui said that Johnson & Johnson was likely to report trial results in early January and be ready to ship doses in February, if its vaccine is authorized. He predicted that AstraZeneca’s trial would report results in late January or early February and potentially begin providing doses later that month.
“We could have all of them,” Slaoui said. “And for this reason, we feel confident we could cover the needs without a specific cliff … We have planned things in such a way as we would indeed avoid a cliff.”
The contract that Pfizer signed with the government in July was to deliver 100 million vaccine doses, and contained an option to contract to buy an additional 500 million doses.
“Pfizer shall inform the Government of appropriate lead times based on purchase of raw materials, capacity reservation and other factors, and Pfizer and the Government shall mutually agree on an appropriate estimated delivery schedule,” the contract states.
“Recognizing the urgency of the need, our manufacturing teams have been working around-the-clock so we can bring the vaccine to the world as quickly, efficiently and equitably as possible,” Rose said.
Additional doses would be “subject to a separate and mutually acceptable agreement” she said.
No agreements with Moderna beyond its initial contract for 100 million have been announced, but the U.S. has the option to purchase 400 million additional doses. Moderna is expected to deliver 20 million doses by year’s end and another tranche in the first quarter of 2021.
They have been at this for almost a year. While politicians argued about masks, superspreader weddings made the news, a presidential election came and went, and at least 281,000 Americans died, nurses reported for work. The Post asked seven ICU nurses what it’s been like to care for the sickest covid patients. This is what they want you to know.
As of Dec. 7, Idaho has seen 110,510 total confirmed cases, 1,035 deaths, and 477 people are currently hospitalized with the virus.
Kori Albi, 31
Covid unit intensive care nurse and unit supervisor, Saint Alphonsus Regional Medical Center
Our staff are getting sick. Our physicians are getting sick. And they’re not getting it from the hospital. They’re getting it from the community. We are almost lucky to care for the covid patients because we know who they are. Anytime we go into these rooms, we know exactly what we need to do. We have all the PPE we need. And as long as we are diligent and follow all the processes that are in place, we can keep ourselves safe. That’s not what worries me at all. Going out into the community is scarier than coming into work every day. Because you don’t know who has it.
This virus has caused this feeling, this sense of isolation. The covid unit is an isolated desert. Every door is shut. Every room has negative airflow. By the time you put your N95 mask on and then your surgical mask over the top of that, then you put your isolation gown on and your face shield on top of that, you can’t tell who is who. So much of health care is about that personal touch — now, our patients can’t even see our name badges because they are on under our gowns. All they see are our eyes through our face mask.
A lot of families are hesitant to have Zoom calls with patients because it can be uncomfortable and awkward. Especially if these patients are sedated and intubated. There’s always that awkwardness of: Can they hear you? Can they not hear you? Even as nurses, we feel like we’re talking to the wall. But we talk to them just as if they were awake. Allowing families to play their music that they like or pray with them or just talk to them can absolutely help. You see vital signs change.
One patient, all she wanted to do was have her son sing her a song. I think I spent over an hour in the room listening to him play the guitar and sing her a song. He sang her mostly hymns.
Death is a very intimate event that normally involves a lot of family members that help bring closure and that helps everyone process. In normal circumstances, health care providers form these relationships with the family at the bedside. All of that has been removed. And we now have to try to form those relationships over the telephone. It’s a traumatic experience. And it’s a long drawn-out process. A lot of people don’t make it out of here. It’s a slow, lonely death.
The amount of death with covid is profound. As nurses, we have learned to process death, but the amount of death has happened in such a short span of time — that’s what’s been overwhelming. I had a patient that we did a Zoom call with. His four-year-old granddaughter lived with him. And she brought tears to the room. The naivete of a four-year-old. Her grandfather was intubated so he couldn’t talk. But he could kind of look around the room. But the innocence of her, saying, “Come home, Pa. I miss you, Pa. I love you Pa,” all through a video screen. The 14-year-old that also lived with them couldn’t formulate words to say anything, and he didn’t know what to do or say in that video. But the four-year-old was telling Pa to come home.
JACKSON, MISS.
As of Dec. 7, Mississippi has seen 166,194 total confirmed cases, 3,961 deaths, and 1,157 people are currently hospitalized with the virus.
Catie Carrigan, 28
ICU, University of Mississippi Medical Center
There are some patients who have been in their younger 20s and their younger 30s, and I think maybe those are the hardest cases. They have families and they have kids just like I do, and it’s hard coming into work and taking care of them. Knowing they’re supposed to be going to college, they’re supposed to be getting married, they’re supposed to be having kids and, instead, they’re laying in a hospital bed on a ventilator fighting for their life.
They have their whole entire lives ahead of them, and then they get hit with this disease that everybody thinks is a hoax and then they die.
I worked in the ER a month ago, so I know exactly what’s going on down there, and now I work in the ICU, so I know exactly what’s going on on both sides of it. There are no ICU beds in the hospital. None. When there are no ICU beds, we hold them in the ER, or we hold them in the PACU (post-anesthesia care unit). The ER still has to treat our trauma patients, our car accidents, our gunshot victims. So when we have those ICU holds in the ER, it obviously makes the jobs of nurses and doctors in the ER way more difficult than it needs to be. We are treating patients in the hallway. They’re just trying to do the best they can with the resources that we have.
There is no room left, essentially, and I think that’s really what people don’t seem to understand. And I get it, when you’re not in health care you don’t really see our side of it, but we’re seeing the worst of it. It’s hard for us to convey that to the public because they don’t seem to want to take our word for it — but take our word for it. Take our word for it.
IOWA CITY
As of Dec. 7, Iowa has seen 244,844 total confirmed cases, 2,717 deaths, and 898 people are currently hospitalized with the virus.
Allison Wynes, 39
Medical intensive care unit, University of Iowa Hospitals and Clinics
I cry every day when I walk in to work, and I cry every day when I walk to my car after work.
You get it out of your system before you show up and you do your job and you’re fine. Then, you go home and you cry before you get home. And then you go home and be mom.
My 9-year-old daughter asks frequently, “Mommy, how many patients were there today? Mommy, how many sick ones were there today? Were you safe? Was everything okay? Do you have to go to work again? How many patients?” She gets it.
I think one thing that people do not appreciate is it’s not only the number or volume of patients that comes through — it’s the level of care that they require, which is so much greater than a standard patient in the ICU or a standard patient in the floor, because they can get very, very sick very quickly.
We were walking a patient who was on ECMO, which is extracorporeal membrane oxygenation, and it took five people to walk her. That’s not normal.
I work in the MICU, so it’s never like a party up in here, but it used to at least be, nine times out of ten, calm and controlled and tidy and clean. Occasionally stuff would go bad and we would all run and help, and then we would all go about our days. Now it just feels like, especially of late, there is equipment everywhere. There are gowns everywhere. There are gloves everywhere, there are people everywhere, and there are fires everywhere.
I’m actually scared, and I’ve never been scared at work before. I am scared that we will lose control.
It’s the human resources we are running low on. We can make a bed, we can find a ventilator, we have PPE. But it’s the human cost of caring for these patients that has been keeping me up at night the past couple of weeks and really making me nauseous every day.
I didn’t think it would be over by now, but I didn’t think we’d be getting hit this hard this late. I thought we’d still just be smoldering. I didn’t know that we would just be a raging fire at this point in time. We’re not prepared for that, but here we are.
After this, I’m going to take my kids to a beach or somewhere.
GLENVIEW, ILL.
As of Dec. 7, Illinois has seen 796,264 total confirmed cases, 14,216 deaths, and 5,190 people are currently hospitalized with the virus.
Luisa Alog Penepacker, 51
ICU, Glenbrook Hospital
I’ve taken care of a lot of husband-wife patients, unfortunately. One of the cases was one in which the husband had tested positive for covid first, but he was a mild case. She was a little bit more serious. She ended up on our unit.
The husband ended up in the hospital the next day, but he was on the step-down unit. When I admitted her, she was terrified, especially knowing that her husband was upstairs in another unit. She was having a hard time breathing, and she grabbed onto my hand and looked at me. She goes, “Am I gonna die?” I mean, I didn’t know what to say. And I just told her, “Not on my watch.” So we just kept on going. But unfortunately, she got intubated the next day.
Then I was sent to work upstairs on the step-down unit. I had her husband that next day, and he was actually quite happy that I saw her. He goes, “You took care of my wife, how is she? I heard that she’s not doing well.” I didn’t know what to say to him, either. I just said, “You know, she’s in the best of care. We’ll take really good care of her.” And he looked really relieved. He goes, “I’m just so glad that someone who had seen her is here now to talk to me.” And my heart broke with that.
She ended up passing. A few days after, he went home, and I didn’t see him, so I don’t know how he took it. He wasn’t able to see her before she passed.
We wear personal air purification respirators on our heads — these big white domes over our heads with a respirator hose going to a machine strapped around our waist, and we look like astronauts walking through the unit, going in and out of patients’ rooms with our plastic gowns and gloves.
It can be frightening to family members if they’re allowed to come to visit and definitely for patients because we’re kind of scary-looking. It can be frantic at times. You walk through the hall, and you see a lot of patients on ventilators. You hear a lot of beeping. People are rounding constantly to check on patients. It’s a busy place.
You don’t know what to tell family members when you see them. What can you say? You just say, “I’m sorry.” You can’t even hug them. I used to be able to hug family members, but you can’t with all the gear.
When patients are scared, I will hold their hand even though I’m wearing gloves. I look them in the eyes as much as I can because really, that’s all you can see. You can’t see our faces. You can barely even hear past the mask. So I’ll make sure to look at them. I try to make an effort to smile with my eyes and to just hold their hand if they need it.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Tammy Kocherhans, 41
Respiratory ICU, Intermountain Healthcare
These patients are different than the typical patient. They’re very complex. They can change in the blink of an eye. And it’s very hard as a nurse when you wrap your heart and soul into taking care of these patients. I started noticing that I was emotionally tired. I was physically completely exhausted. And I was beginning to question whether or not I could continue forward being a nurse at all. I was past my physical capacity.
I happened to be working a day where another health care worker who was a veteran said that this was like a combat zone, and for some reason in my head, that validated the way that I was feeling. So I reached out to one of my best friends who is a veteran, a flight medic, and he said, “I meditate and do yoga.”
Once I started doing that, I was able to handle the emotional crises, the physical pain of working so, so many long, hard hours. We do something called proning, where you take patients and flip them over onto their bellies. And that sounds really easy, but it takes a team of a minimum of five people. It is extremely taxing on your body. It hurts. And I lift weights! The meditation and yoga really has saved my life, my mental capacity, my spiritual capacity, my physical capacity, everything that is required to give to these patients.
Hopefully by 8 p.m., I’m out in the parking lot and spend a minute in my car to unload from my day. It’s all about taking a moment to breathe for myself and then going through whatever came up that day that I need to let go of. It depends on how complicated my patient was that day, whether I can let my whole day go or if I have to spend time to go through each piece and work it down to: What did I do right? Did I miss something? Sometimes I just can’t let some details go quickly, and I have to work them down to allow myself to say I did everything that I possibly could for this individual this day, in this time, in this situation. And whatever the outcome was or is, I followed protocol. I did everything that I knew how to do. And it’s going to be OK.
I find it very frustrating when I go out and about on my days off and I see people very blatantly not wearing masks or trying to tell me how come they don’t work or telling me that this pandemic isn’t real. I find it completely disrespectful to the work we do to save people’s lives, to have people think that this pandemic isn’t real, to show utter disregard for people around them, not trying to do their part.
And I really wish that I could take people on a day with me so that they can see what I see. So that they can feel your feet ache so bad that you wish they’d just fall off, because you’re on that concrete for so many hours. Your back aches because you’re wearing equipment to save your life — so that you can save somebody else’s life. And your head hurts. I’ve never had so many headaches in my life because part of the equipment sits on your head, and after 12 hours, it starts to exert so much pressure that you start to have a headache, and you’re dehydrated.
Early in the pandemic, I remember walking into this room, and this young patient was crying and asked me if they were going to die. And I’m a mom of teenagers. For me, that was awful because this patient was all alone, and we as staff were minimizing contact because we didn’t want to get the virus.
This patient started physically trembling in the bed. I couldn’t take it anymore, and I went over and just held this patient because that’s what I’d want somebody to do for my children. That was my first patient that I held like that. And there have been many since.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Nate Smithson, 28
Respiratory ICU, IntermountainHealthcare
A few weeks ago, my wife and I were on a date at a restaurant. And in the middle of nowhere, I had this panic attack and went and hid in the bathroom stall for half an hour. I have no idea what brought it on. I just couldn’t handle being there right then, which was weird for me. That’s the first time anything like that has happened. But since then, it’s happened multiple times, where the anxiety and stress is overwhelming, and I can’t handle it. So I have to go and excuse myself for a little bit.
Balancing work and life is something that used to seem possible. Now it doesn’t seem like there is any difference between the two. I fall asleep and I dream about my patients.
When we got our first covid patient in February in the hospital, in the ICU, we all kind of thought it was a little bit of a joke, to be honest. I had this patient, and he was sitting there with minimal amounts of oxygen in the room just watching TV. He’s like, “I’m fine. I don’t know why everyone’s freaking out about this.” And I thought the same thing. And then a few hours later, he stands to go pee, and I’m looking at his monitor. And it drops down to the low 90s. Ninety-two is about as low as you want to go. And then it starts dropping down lower, to about the 70s. Then it gets down into the 60s and 50s. And that’s dangerous territory. That’s where brain cells start dying and you start having some serious problems.
I run into the room. We get him back into bed and throw all the oxygen that we have in the room on him, crank everything up, and he’s not recovering from it. We had to intubate right then and there. And about an hour later, he finally starts recovering a little bit. But at this point, he’s sedated, he’s on the ventilator. Everything is worse. And that’s the first time where it’s like: Oh, crap, this is serious. This is something else. I’ve never seen anything like that before.
If a patient’s heart stops or if they stop breathing, we call a code blue, and that’s when the doctor, respiratory therapist, nurses, everybody comes into the room. We start chest compressions or CPR or that kind of stuff. This one patient’s heart is not working. So I call the code blue. We all get in there. We start doing the chest compressions. Five minutes later, we get the patient back. We all go back about our work. Twenty minutes later, same thing happens again. We start doing the chest compressions. We start pushing medications as fast as we can to get the patient back again.
The spouse comes into the hospital. I explain: “Just so you know, this is what happened before. It could possibly happen again. If it does, I’m going to need you to step outside of the room.” And as I’m explaining this, sure enough, it happens again. We lose the pulse. We lose the heartbeat. So I ask her to leave the room. Everyone gets in there, and we start going for it. We went for almost two hours: chest compressions, pushing medications, shocking the patient’s heart.
The doctor is ultimately the one who makes the decision about when we stop, and they call time of death. But typically in situations like that, where it’s unexpected and sudden, they want to make sure that everybody can go home that night feeling OK about what they did, knowing that they did everything. And after an hour, he stops, turns to the room and asks: Does anyone have a problem with us stopping?
I didn’t have a problem, but then as he’s saying that, I look out the window, and the patient’s wife is just watching us. She’s been sitting out there watching us for an hour, and no one’s saying anything.
And I ask them to keep going.
So we did. We went almost for another hour after that, and we didn’t get the patient back. He ended up dying.
But I think for me, that was important — to keep going. Not because we thought we would get them back, but so that his wife would know that we did everything we could.
I still go to bed with her face kind of burned into my mind, of just seeing her sitting out there watching us, and that’s what kills me.
COLUMBUS, OHIO
As of Dec. 7, Ohio has seen 475,024 total confirmed cases and 6,959 deaths.
Kahlia Anderson, 32
ICU, Ohio State University Wexner Medical Center
I graduated from nursing school in May 2019. I started here at the Wexner in August. Our orientation is a 20-week program, and so I came out on my own Jan. 12, 2020. The pandemic hit us at the end of February.
In nursing school, I think your biggest fears are making med errors, or harming your patient in some way, or just not knowing how to do everything. Did I check my patient’s blood pressure before I gave this blood pressure medication, or did I give the correct dose of a specific medication? I had heard stories about that on the unit, like make sure you’re careful with the needle stick, or make sure you’re careful with this medication. And I don’t even think about those kinds of things anymore.
Now it’s the fear of the unknown. It’s the fear that anything could happen because of this virus and my patient could die regardless of what I do.
When I got my first covid-positive patient, I remember thinking: Somebody did the assignment wrong because there’s no way that they believe that I should be taking care of this patient. I can remember the feeling. I can remember the day. It was a weekend. I was on a day shift. And I was thinking to myself: Who trusted me, the new nurse to take care of a covid-positive patient? How am I going to do this? How am I going to keep this patient safe? How am I going to keep myself safe? Am I safe? Wait, who cares about me? Let’s get back to the patient. What do they need?
At the time, I didn’t even understand some of the ventilator settings because I was still that new, and it was still that fresh to me. And I thought: This machine is doing that much work for them, and I don’t know enough about it, but I’m going to make sure that I get it done and I’m going to figure it out today to make sure that this patient gets everything that they need. And I’m going to call their family and double check with them and check in with them and call them.
That patient is alive. That patient is no longer in the hospital. As far as I know, that patient is home and safe with family.
I would feel like: There’s someone more experienced. There’s someone more adequate to deal with this. And I was like — oh, it’s me. This is me, I’m doing this, and I’ve been doing it ever since.
I saw new nurses come out of orientation, and I saw the type of assignments that they would get. So my mind fixated on like: I’m going to get patients that are ready to transfer out. They can talk, they can eat. They’re just waiting for a bed on another unit. Or maybe it’s a patient who needs long-term care. So they’re waiting to go to a facility to be discharged. And so I was thinking to myself: I’m going to get my feet wet. It’s going to be great. I’m going to build up this experience, and then I’m going to start getting sicker patients, and I’m going to be ready.
Once covid hit, there was no room for those types of patients anymore. Everyone had covid, everyone was sick, everyone was intubated or approaching intubation.
And for me, I just wanted my first experience. I wanted to have the simple experience of building and getting better. But that’s not what was in store. And I can’t say that I’m upset about it today. I’m grateful for this experience. I don’t wish this pandemic on anyone. I wish it was not here. I wish that it was different. But as a nurse, as a new nurse, these experiences are unique to me. It’s making me a better nurse. It’s made me a better person, and I can only continue to just be.
We did cry in the beginning, and now not so much. I think we all struggled when we had a young death. Someone in their 20s was very difficult for us. Because you think: That was a young life. What a young life that was, and they’re not here anymore. Because of a virus. That’s hard. It’s very hard.
Hospitals across the country are reaching their breaking point on ICU and bed capacity as COVID surges, forcing many health systems to begin diverting patients from emergency rooms and ration care, Axios’ Orion Rummler reports.
What’s happening:
Pennsylvania: “Most hospitals in Montgomery County are at or near capacity,” county commissioners’ chair Valerie Arkoosh said in Norristown, Pennsylvania, last Wednesday.
Georgia: Major hospitals, including Grady Memorial and Emory University, have had to turn away patients brought in ambulances, the Atlanta-Journal Constitution reports.
South Dakota: The Monument Health Rapid City Hospital and Sanford USD Medical Center — some of the biggest in the state — say they have no more ICU beds, the Mitchell Republic reports.
Colorado: More than a third of hospitals across the state said in a survey they expect staffing shortages this week, Colorado Public Radio reports.
Context:White House coronavirus task force coordinator Deborah Birx noted on Sunday’s “Meet the Press” that U.S. hospitals are usually anywhere from 80 to 90% full in the fall and winter — and “when you add 10, 15, 20% COVID-19 patients on top of that, that’s what puts them at the breaking point.”
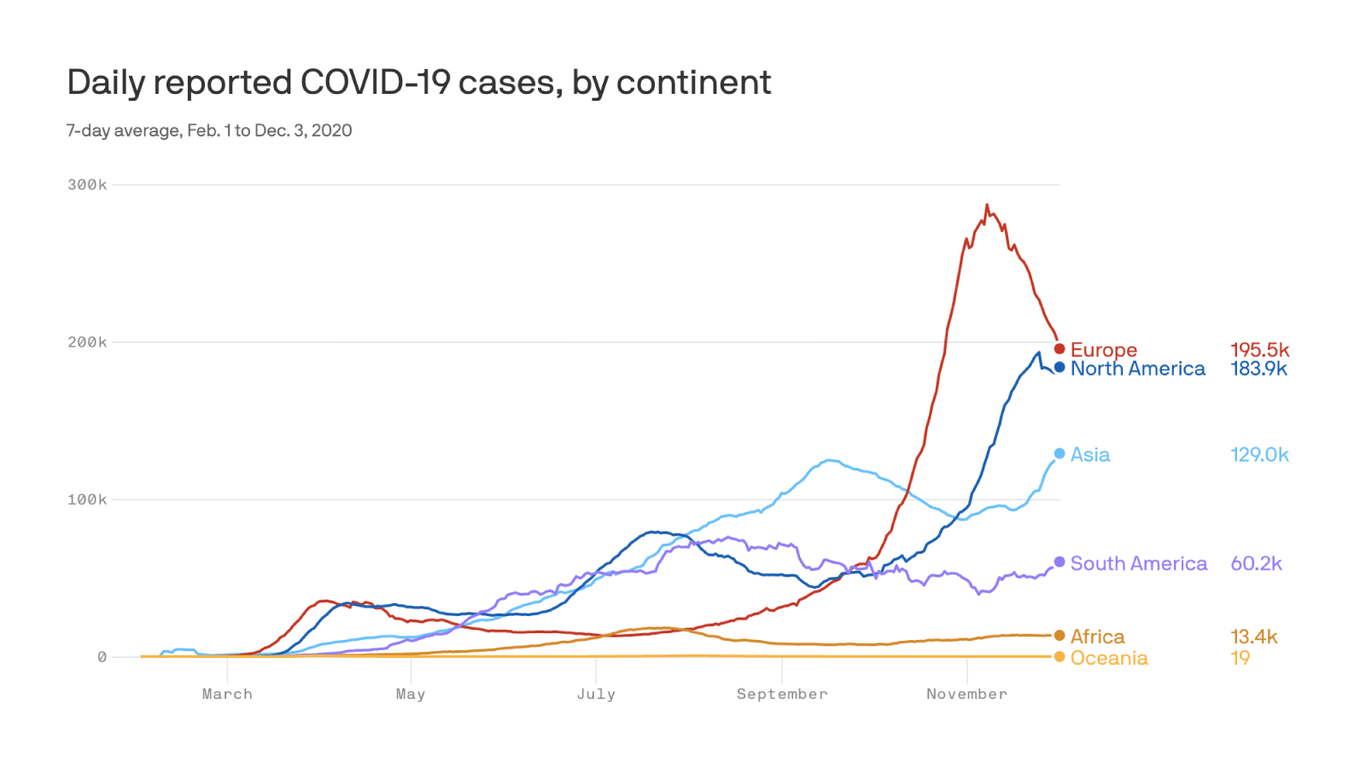
While the U.S. continues to set records for new coronavirus cases, European countries have managed to turn their own terrifying spikes around.
The big picture:As some states in the U.S. crack down to head off the worst, the debate in countries like the U.K. and France has shifted to whether and how to lighten their own restrictions before the holidays.
America’s surge lagged two to three weeks behind Europe’s, with a similarly worrying trajectory. However, responses in U.S. states have been uneven and generally less severe than in most European countries.
Daily case counts are already rising significantly in most U.S. states, and they’re likely to tick up further following Thanksgiving gatherings around the country.
Much of Europe returned to some form of lockdown in the fall, but the restrictions tended to be less restrictive than in the spring. They certainly haven’t been in place as long.
Many countries closed bars and restaurants, and nearly all at least limited their opening hours. Social gatherings were also limited — in Germany’s case, to groups of up to five from a maximum of two households (children are exempted).
But schools have remained open across nearly all of the continent, and the disruption to economic activity, while highly significant, hasn’t been quite as severe (though many governments have faced anti-lockdown protests).
The fact that countries like Italy were able to bend the curve so quickly with partial lockdowns is encouraging, says Stephen Kissler, a researcher at Harvard who models the spread of diseases, including COVID-19.
“The evidence shows that these full lockdowns we underwent in the spring aren’t necessary now,” he says.
“We have so much more information now that we can respond a lot more quickly and in a more targeted manner — really just shutting down the types of activities that contribute most to the spread.”
Test positivity rates are falling significantly in many EU countries — another sign that the current wave is subsiding.
In Belgium, for example, the positivity rate fell from 21% to 8% over the past three weeks, with similar trends in France and the Netherlands.
The outlook is a bit darker in Central Europe. The Czech Republic still has a positivity rate of 21%, while Poland’s 49% rate is higher than every U.S. state but Idaho.
Reality check:Europe is far from out of the woods. Deaths and hospitalizations lag behind spikes in cases, and those numbers are falling much later and less sharply.
Italy recorded a record-high death toll on Thursday, three weeks after case numbers peaked.
And while the trajectory on cases is positive, public health experts fear a swift reversal if countries open up too quickly.
Governments in the U.K., France and elsewhere had promised the measures would be temporary and Christmas celebrations would still be possible. They’re now attempting a difficult balancing act with the virus still spreading rampantly.
The U.K. is introducing the “Christmas bubble,” which will allow up to three households to gather together over the Christmas period.
Spain is increasing the maximum gathering size from 6 to 10.
Germany plans to tighten restrictions through Dec. 20 and then allow groups of up to 10 to gather.
The bottom line:In Europe, those decisions are being made with cases on the decline and the outlook improving. That’s not the case in the U.S.
Despite taking a huge volume hit in Q2, most hospitals have managed to maintain positive operating margins—largely thanks to a $100B cash infusion from the federal government via the Coronavirus Aid, Relief and Economic Security (CARES) Act.
According to Kaufman Hall’s most recent National Hospital Flash Report, based on data from over 900 hospitals of all sizes nationwide, hospitals would have been operating at a significant loss without federal aid. As the graphic above shows, the average hospital operating margin without CARES Act relief funds would have been negative eight percent in April—and would still be in the red as of October, despite much of the cancelled elective business returning across the summer and early fall.
However, with the aid, hospitals operating margins only turned negative in April and May. When compared to the same time period last year, year-to-date (YTD) gross revenue is down almost five percent, though net patient service revenue per discharge is up—the result of longer lengths of stay, the 20 percent Medicare reimbursement bump for COVID-19 patients, and suspension of the two percent sequestration adjustment on Medicare fee-for-service payments. Yet hospital expenses per discharge are also up 13.5 percent, dampening profitability.
Though the CARES Act has been a stopgap solution for the vast majority of hospitals, a handful, most notably HCA Healthcare, have proactively returned the money. While motivations for doing so are varied, we’ve been hearing that the ever-changing reporting and spending requirements associated with CARES Act funding have many hospital leaders concerned about possible future claw-backs.
With COVID-19 hospitalizations now reaching record-breaking highs, potentially forcing another round of shut-downs, and with little movement on another round of federal relief, hospitals may be on their own for the time being—and the greatest hit to health system finances may still be yet to come.
We are now in uncharted and dangerous new territory in the coronavirus pandemic, with the US recording a record-high 2,800 deaths on Thursday, along with 200,000 new cases—the second highest daily total of the pandemic so far.
More than 100,000 Americans are now hospitalized with COVID-19, occupying more than 10 percent of the nation’s hospital beds, and creating capacity constraints at hospitals around the country. With the impact of Thanksgiving travel—which was the heaviest since March—yet to be seen in the numbers, and with hospitalizations and deaths lagging new case counts by several weeks (as an epidemiological rule of thumb, 1.7 percent of new cases will result in reported deaths from COVID after 22 days), we are almost certainly headed for a grim winter holiday season.
But the light at the end of the tunnel grew brighter this week, with the United Kingdom becoming the first Western country to approve a COVID vaccine. (China and Russia both rolled out vaccines prior to Phase 3 trials being completed.)
Doctors and hospital staff in the UK will begin to administer Pfizer’s vaccine next week, and the US Food and Drug Administration (FDA) is expected to approve the same vaccine for emergency use on or shortly after an outside panel of experts convenes on December 10th.
Moderna, whose vaccine is similar to Pfizer’s, submitted an application for emergency use this week, and it will be evaluated on December 17th.
In the meantime, a group advising the Centers for Disease Control and Prevention (CDC) held a public meeting this week to craft recommendations for which populations should be prioritized to receive the new vaccines, settling on healthcare workers and residents of long-term care facilities as first in line. While state public health officials will make the final decisions about who gets vaccinated, most are expected to follow the CDC’s guidelines. The two priority groups represent about 24M people, most of whom could be immunized by the end of this month if all goes according to plan. The end of the pandemic will not come quickly, or easily, but it will come—we are near the beginning of the end.
Roommates Madilyn Dennington, Bailey Mills and Olivia Noe, all 23, were issued misdemeanor citations in connection with an Oct. 31 football watch party at their East Nashville home on the 1200 block of Boscobel Street south of Fatherland Street.
Police spokesman Don Aaron said the women were served with court summonses on Monday and are slated to appear on the charges Dec. 16.
According to an arrest affidavit, officers responded about 6:30 p.m. to a complaint about a loud party at the home, heard music blaring and saw several people in the yard. In all, police said they found more than 100 people inside and outside the home.
When officers spoke to Dennington, Mills and Noe outside, they told police they had organized a watch party at their home for a football game, the affidavit states. The officers told the women that at that time, no more than 25 people were permitted to gather in Davidson County unless the gathering was approved by the city.
The women then went inside and told everyone to leave, police reported.
Police then alerted Metro Health officials about the party. Hugh Atkins, Metro Health’s environmental health services director, confirmed the Health Department did not receive an event application for the gathering.
On Tuesday, Davidson County reportedan increase of 851 cases in 24 hours — the second-highest ever daily increase. So far 369 people in Nashville have died from the virus.
Dennington is a registered nurse at TriStar Skyline Medical Center, authorities said.
It was not immediately known whether the hospital had taken any disciplinary action against Dennington. She did not return an immediate request for comment and blocked her Facebook page from a Tennessean reporter shortly after being contacted.
“Properly following pandemic regulations is extremely important to help reduce the spread of COVID-19,” Anna-Lee Cockrill, a spokeswoman for TriStar, said regarding the party. “We are looking into this further.”
According to their social media pages, all three roommates formerly attended the University of Mississippi before moving to Nashville, and Dennington and Noe both graduated from the University of Mississippi Medical Center.
Noe and Mills also could not immediately be reached for comment.
More than 50 arrests, 315 citations
Police data shows at least 50 people have been arrested and more than 315 have been cited under local emergency health orders that went into effect earlier this year.
As of Tuesday, only one of the arrested defendants had pleaded guilty: Jeffrey Mathews, a 36-year-old Goodlettsville dentist arrested for throwing an Aug. 1 house party on Fern Avenue in East Nashville. He was one of two men criminally charged for the party that drew hundreds.
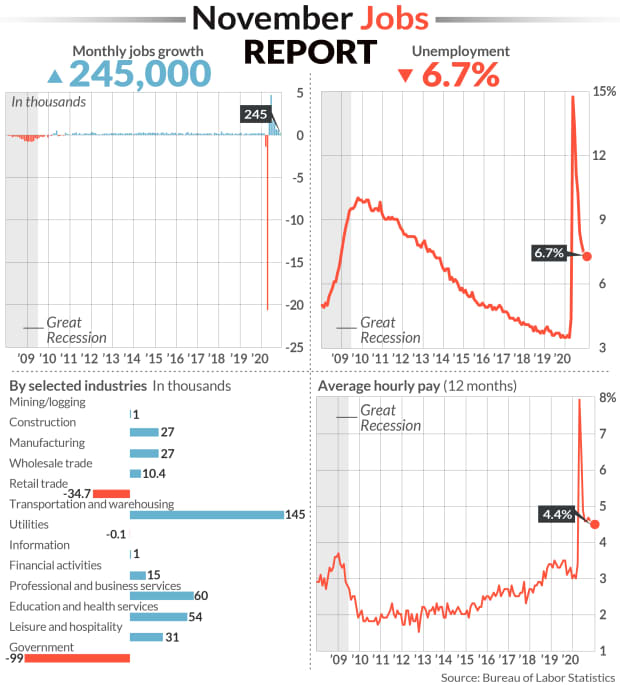
The U.S. economy added back the smallest number of jobs in seven months in November, as the labor market endured mounting pressure from the coronavirus pandemic while businesses wait for a vaccine to be distributed next year.
The U.S. Department of Labor released its monthly jobs report Friday morning at 8:30 a.m. ET. Here were the main results from the report, compared to Bloomberg consensus data as of Friday morning:
Change in non-farm payrolls: +245,000 vs. +460,000 expected and a revised +610,000 in October
Unemployment rate: 6.7% vs. 6.7% expected and 6.9% in October
Average Hourly Earnings month-over-month: 0.3% vs. +0.1% expected and +0.1% in October
Average Hourly Earnings year-over-year: 4.4% vs. +4.2% expected and a revised +4.4% in October
During November, a plethora of new stay-in-place measures and curfews swept the nation as COVID-19 cases, hospitalizations and deaths swelled to record levels. These renewed restrictions weighed on the rate of the recovery in the labor market, which had already been slowing after a record surge in rehiring followed the initial wave of lockdowns in the spring.
To that end, job gains in November sharply missed expectations. Non-farm payrolls grew by just 245,000 during the month for the smallest number since April’s record, virus-induced decline. October’s payroll gain was downwardly revised to 610,000 from the 638,000 reported earlier, while September’s gain was raised to 711,000 from 672,000.
A third straight month of declining government employment served as a drag on the headline payrolls figure, as another 93,000 temporary workers hired for the 2020 Census were let go.
In the private sector, retail trade industries shed nearly 35,000 jobs following a gain of 95,000 in October. Leisure and hospitality employers added just 31,000 jobs during November, declining by nearly 90% from October. And in goods-producing industries, manufacturing jobs rose by only 27,000 for the month, falling short of the 40,000 expected.
But a handful of other industries added more jobs in November from October: Transportation and warehousing jobs grew by 145,000 to more than double October’s advance, and growth in wholesale trade positions also doubled to 10,400.
November’s unemployment rate also improved just marginally to 6.7% from the 6.9% reported in October. While down from a pandemic-era high of 14.7% in April, the jobless rate remains nearly double that from before the pandemic.
Other employment reports this week underscored the decelerating trend. Private-sector hiring fell to the lowest level in four months in November, according to data tracked by ADP. New weekly jobless claims began rising again around the 12th of the month, when the Labor Department conducts its surveys for its monthly jobs report. And in the Federal Reserve’s November Beige Book, the central bank noted that nearly all districts reported rising employment, “but for most, the pace was slow, at best, and the recovery remained incomplete.”
The U.S. economy still has a ways to go before fully making up for the drop in payrolls induced by the pandemic.Even with a seventh straight month of net job gains, the economy remains about 9.8 million jobs short of its pre-pandemic level in February. The U.S. economy lost more than 22 million jobs between March and April.
And worryingly, the number of the long-term unemployed has kept climbing. Those classified as “permanent job losers” totaled 3.7 million in November, eclipsing the number of individuals on temporary layoff for the second time since the start of the pandemic. Permanent job losers have increased by 2.5 million since February, before the pandemic meaningfully hit the U.S. economy.
In Washington, congressional lawmakers have for months been at a stalemate over the size and scope of another stimulus package, which could help provide funds for businesses to help keep workers employed, and offer extended unemployment benefits for those the pandemic has kept out of work. Federal unemployment programs authorized under the CARES Act in the spring are poised to expire at the end of the month. These include the Pandemic Emergency Unemployment Compensation and Pandemic Unemployment Assistance programs, which together provide benefits for more than 13 million Americans.
“The only thing that matters about today’s NFP [non-farm payrolls] report is whether it increases the likelihood of a stimulus deal getting done during the lame duck session,” Peter Tchir, head of macro strategy for Academy Securities, said in an email Friday morning. “While the unemployment rate shrunk and wages ticked up nicely, the headline number dropped significantly, was well below average expectations, and included some downward revisions to last month (and upward revisions to 2 months ago) – all of which point to a less robust job market.”
More than 100,200 Americans were hospitalized as of Wednesday due to the coronavirus for the first time since the outbreak began in early 2020, per the COVID Tracking Project.
The big picture: The milestone comes as health officials anticipated cases to surge due to holiday travel and gatherings. The impact of the holiday remains notable, as many states across the country are only reporting partial data.
Meanwhile, more hospitals are running out of beds or turning away new patients, limiting the care available to both coronavirus patients and those with other health care emergencies, Axios Caitlin Owens reports.
Flashback:The daily rate of new coronavirus infections rose by about 10% in week leading up to Thanksgiving, continuing a dismal trend that may get even worse in the weeks to come.