With both Republicans and Democrats taking on these Goliaths individually, this could be a watershed moment for bi-partisan action.
The push and pull between providers and insurance companies is as old as our health payment system. Doctors have long argued insurers pay too little and that they too often interfere in patient care.
Dramatic increases in prior authorization, aggressive payment negotiations and less-generous reimbursement to doctors by Medicare Advantage plans show there’s little question the balance of power in this equation has swung toward payers.
These practices have led some doctors to look for outside investment, namely private equity, to keep their cash flow healthy and their operations functional. The trend of private equity acquisitions of physician practices is worthy of the federal scrutiny it has attracted. Insurers have noticed this trend, too, and appear ready to propose a profitable partnership.
Bloomberg recentlyreported that CVS/Aetna is looking for a private equity partner to invest in Oak Street Health, the primary care business CVS acquired for $9.5 billion last year. Oak Street is a significant player in primary care delivery, particularly for Americans on Medicare, with more than 100 clinics nationwide. CVS is said to be exploring a joint venture with a private equity firm to significantly expand Oak Street’s footprint and therefore also expand the parent corporation’s direct control over care for millions of seniors and disabled Americans across hundreds of communities.
Republicans have led scrutiny of pharmacy benefit managers on Capitol Hill. And Democratic attacks on private equity in health care have recently intensified. I hope, then, that both parties would find common ground in being watchful of a joint venture between private equity and one of the country’s largest PBMs, Caremark, also owned by CVS/Aetna.
The combination of health insurers and PBMs over the last decade – United Healthcare and Optum; CVS/Aetna and Caremark, and Cigna and Express Scripts – has increasingly handed a few large corporations the ability to approve or deny claims, set payment rates for care, choose what prescriptions to dispense, what prescriptions should cost, and how much patients must pay out-of-pocket for their medications before their coverage kicks in.
As enrollment in Medicare Advantage plans has grown to include a majority of the nation’s elderly and disabled people, we have seen insurers source record profits off the backs of the taxpayer-funded program. But in recent months, insurers have told investors they have had higher than expected Medicare Advantage claims – in particular CVS/Aetna, which took a hammering on Wall Street recently because its Medicare Advantage enrollees were using more health care services than company executives had expected.
It is natural, then, that one of the largest insurer-owned PBMs is looking to expand its hold on primary care for older Americans. Primary care is often the gateway to our health care system, driving referrals to specialists and procedures that lead to the largest claims insurers and their employer customers have to pay. By employing a growing number of primary care providers, CVS/Aetna can increasingly influence referrals to specialists and therefore the care or pharmacy benefit costs those patients may incur.
Control of primary care doctors holds another benefit for insurers: determination of what primary care doctor a patient sees.
People enrolled in an Aetna Medicare Advantage or employer-sponsored plan may find that care is easier to access at Oak Street clinics. Unfortunately, while that feels monopolistic and ethically alarming, this vertical integration has received relatively little scrutiny by lawmakers and regulators.
No law prevents an insurance company or PBM from kicking doctors it does not own out of network while creating preferential treatment for doctors directly employed by or closely affiliated with the corporate mothership.
In fact, the system largely incentivizes this. And shareholders expect insurers to keep up with their peers. As UnitedHealth Group has become increasingly aggressive in its acquisitions of physician practices – now employing or affiliated with about one in ten of the nation’s doctors – it has also become increasingly aggressive in its contract negotiations with physicians it does not control, particularly the specialists who depend on the referrals that come from primary care physicians.
That’s another area where looking to expand Oak Street Health makes smart business sense for CVS/Aetna. Specialist physicians are historically accustomed to higher compensation than primary care doctors and are used to striking hard-fought deals with insurers to stay in-network.
By controlling the flow of primary care referrals to specialists, CVS/Aetna can control what insurers have long-desired greater influence over: patient utilization. As a key driver of referrals to specialists in a specific market, CVS/Aetna will have even more power in contract negotiations with specialists.
As Oak Street’s clinics grow market share in the communities they serve, specialists in that market will feel even more pressured to stay in-network with Aetna and to refer prescriptions to CVS pharmacies. That has the dual benefit for CVS/Aetna of helping to predict what patients will be treated for once they go to a specialist and control over what the insurer will have to pay that specialist.
With different corporate owners, this sort of model could easily run afoul of the federal Anti-Kickback Statute and Stark Law.
No doctor or physician practice is allowed to receive anything of value for the referral of a patient. But that law only applies when there is separate ownership between the referring doctor and the specialist.
CVS/Aetna would clearly be securing value – in the form of lower patient utilization and effective reimbursement rates – under this model. But with Oak Street owned by CVS/Aetna and specialists forced to agree to lower reimbursement rates through negotiations with an insurer that appears separate from Oak Street, there’s no basis for a claim under the Stark Law. There may be antitrust implications, but those are more difficult and take longer to prove – and the fact the federal government cleared CVS/Aetna to acquire Oak Street Health last year wouldn’t help that argument.
This model is already of concern, which is why I continue to urge examination of increasing insurer control of physicians across the country. Their embrace of private equity to accelerate this model is truly alarming. And given Democrats’ recent focus on private equity in health care, they should work with their Republican colleagues who are rightly alarmed about the increasingly anti-competitive, monopolistic health insurance industry.
The Affordable Care Act turned 14 on March 23. It has done a lot of good for a lot of people, but big changes in the law are urgently needed to address some very big misses and consequences I don’t believe most proponents of the law intended or expected.
At the top of the list of needed reforms: restraining the power and influence of the rapidly growing corporations that are siphoning more and more money from federal and state governments – and our personal bank accounts – to enrich their executives and shareholders.
I was among many advocates who supported the ACA’s passage, despite the law’s ultimate shortcomings. It broadened access to health insurance, both through government subsidies to help people pay their premiums and by banning prevalent industry practices that had made it impossible for millions of American families to buy coverage at any price. It’s important to remember that before the ACA, insurers routinely refused to sell policies to a third or more applicants because of a long list of “preexisting conditions” – from acne and heart disease to simply being overweight – and frequently rescinded coverage when policyholders were diagnosed with cancer and other diseases.
While insurance company executives were publicly critical of the law, they quickly took advantage of loopholes (many of which their lobbyists created) that would allow them to reap windfall profits in the years ahead – and they have, as you’ll see below.
I wrote and spoke frequently as an industry whistleblower about what I thought Congress should know and do, perhaps most memorably in an interview with Bill Moyers. During my Congressional testimony in the months leading up to the final passage of the bill in 2010, I told lawmakers that if they passed it without a public option and acquiesced to industry demands, they might as well call it “The Health Insurance Industry Profit Protection and Enhancement Act.”
A health plan similar to Medicare that could have been a more affordable option for many of us almost happened, but at the last minute, the Senate was forced to strip the public option out of the bill at the insistence of Sen. Joe Lieberman (I-Connecticut), who died on March 27, 2024. The Senate did not have a single vote to spare as the final debate on the bill was approaching, and insurance industry lobbyists knew they could kill the public option if they could get just one of the bill’s supporters to oppose it. So they turned to Lieberman, a former Democrat who was Vice President Al Gore’s running mate in 2000 and who continued to caucus with Democrats. It worked. Lieberman wouldn’t even allow a vote on the bill if it created a public option. Among Lieberman’s constituents and campaign funders were insurance company executives who lived in or around Hartford, the insurance capital of the world. Lieberman would go on to be the founding chair of a political group called No Labels, which is trying to find someone to run as a third-party presidential candidate this year.
The work of Big Insurance and its army of lobbyists paid off as insurers had hoped. The demise of the public option was a driving force behind the record profits – and CEO pay – that we see in the industry today.
The good effects of the ACA:
Nearly 49 million U.S. residents (or 16%) were uninsured in 2010. The law has helped bring that down to 25.4 million, or 8.3% (although a large and growing number of Americans are now “functionally uninsured” because of unaffordable out-of-pocket requirements, which President Biden pledged to address in his recent State of the Union speech).
The ACA also made it illegal for insurers to refuse to sell coverage to people with preexisting conditions, which even included birth defects, or charge anyone more for their coverage based on their health status; it expanded Medicaid(in all but 10 states that still refuse to cover more low-income individuals and families); it allowed young people to stay on their families’ policies until they turn 26; and it required insurers to spend at least 80% of our premiums on the health care goods and services our doctors say we need (a well-intended provision of the law that insurers have figured out how to game).
The not-so-good effects of the ACA:
As taxpayers and health care consumers, we have paid a high price in many ways as health insurance companies have transformed themselves into massive money-making machines with tentacles reaching deep into health care delivery and taxpayers’ pockets.
To make policies affordable in the individual market, for example, the government agreed to subsidize premiums for the vast majority of people seeking coverage there, meaning billions of new dollars started flowing to private insurance companies. (It also allowed insurers to charge older Americans three times as much as they charge younger people for the same coverage.) Even more tax dollars have been sent to insurers as part of the Medicaid expansion. That’s because private insurers over the years have persuaded most states to turn their Medicaid programs over to them to administer.
We invite you to take a look at how the ascendency of health insurers over the past several years has made a few shareholders and executives much richer while the rest of us struggle despite – and in some cases because of – the Affordable Care Act.
BY THE NUMBERS
In 2010, we as a nation spent $2.6 trillion on health care. This year we will spend almost twice as much – an estimated $4.9 trillion, much of it out of our own pockets even with insurance.
In 2010, the average cost of a family health insurance policy through an employer was $13,710. Last year, the average was nearly $24,000, a 75% increase.
The ACA, to its credit, set an annual maximum on how much those of us with insurance have to pay before our coverage kicks in, but, at the insurance industry’s insistence, it goes up every year. When that limit went into effect in 2014, it was $12,700 for a family. This year, it has increased by 48%, to $18,900. That means insurers can get away with paying fewer claims than they once did, and many families have to empty their bank accounts when a family member gets sick or injured. Most people don’t reach that limit, but even a few hundred dollars is more than many families have on hand to cover deductibles and other out-of-pocket requirements. Now 100 million Americans – nearly one of every three of us – are mired in medical debt, even though almost 92% of us are presumably “covered.” The coverage just isn’t as adequate as it used to be or needs to be.
Meanwhile, insurance companies had a gangbuster 2023. The seven big for-profit U.S. health insurers’ revenues reached $1.39 trillion, and profits totaled a whopping $70.7 billion last year.
SWEEPING CHANGE, CONSOLIDATION–AND HUGE PROFITS FOR INVESTORS
Insurance company shareholders and executives have become much wealthier as the stock prices of the seven big for-profit corporations that control the health insurance market have skyrocketed.
NOTE: The Dow Jones Industrial Average is listed on this chart as a reference because it is a leading stock market index that tracks 30 of the largest publicly traded companies in the United States.
REVENUES collected by those seven companies have more than tripled (up 346%), increasing by more than $1 trillion in just the past ten years.
PROFITS (earnings from operations) have more than doubled (up 211%), increasing by more than $48 billion.
The CEOs of these companies are among the highest paid in the country. In 2022, the most recent year the companies have reported executive compensation, they collectively made $136.5 million.
U.S. HEALTH PLAN ENROLLMENT
Enrollment in the companies’ health plans is a mix of “commercial” policies they sell to individuals and families and that they manage for “plan sponsors” – primarily employers and unions – and government/enrollee-financed plans (Medicare, Medicaid, Tricare for military personnel and their dependents and the Federal Employee Health Benefits program).
Enrollment in their commercial plans grew by just 7.65% over the 10 years and declined significantly at UnitedHealth, CVS/Aetna and Humana. Centene and Molina picked up commercial enrollees through their participation in several ACA (Obamacare) markets in which most enrollees qualify for federal premium subsidies paid directly to insurers.
While not growing substantially, commercial plans remain very profitable because insurers charge considerably more in premiums now than a decade ago.
(1) The 2013 total for CVS/Aetna was reported by Aetna before its 2018 acquisition by CVS. (2) Humana announced last year it is exiting the commercial health insurance business. (3) Enrollment in the ACA’s marketplace plans account for all of Molina’s commercial business.
By contrast, enrollment in the government-financed Medicaid and Medicare Advantage programs has increased 197% and 167%, respectively, over the past 10 years.
(1) The 2013 total for CVS/Aetna was reported by Aetna before its 2018 acquisition by CVS.
Of the 65.9 million people eligible for Medicare at the beginning of 2024, 33 million, slightly more than half, enrolled in a private Medicare Advantage plan operated by either a nonprofit or for-profit health insurer, but, increasingly, three of the big for-profits grabbed most new enrollees.
Of the 1.7 million new Medicare Advantage enrollees this year, 86% were captured by UnitedHealth, Humana and Aetna.
Those three companies are the leaders in the Medicare Advantage business among the for-profit companies, and, according to the health care consulting firm Chartis, are taking over the program “at breakneck speed.”
(1) The 2013 total for CVS/Aetna was reported by Aetna before its 2018 acquisition by CVS. (2,3) Centene’s and Molina’s totals include Medicare Supplement; they do not break out enrollment in the two Medicare categories separately.
It is worth noting that although four companies saw growth in their Medicare Supplement enrollment over the decade, enrollment in Medicare Supplement policies has been declining in more recent years as insurers have attracted more seniors and disabled people into their Medicare Advantage plans.
OTHER FEDERAL PROGRAMS
In addition to the above categories, Humana and Centene have significant enrollment in Tricare, the government-financed program for the military. Humana reported 6 million military enrollees in 2023, up from 3.1 million in 2013. Centene reported 2.8 million in 2023. It did not report any military enrollment in 2013.
Elevance reported having 1.6 million enrollees in the Federal Employees Health Benefits Program in 2023, up from 1.5 million in 2013. That total is included in the commercial enrollment category above.
At Cigna, Express Scripts’ pharmacy operations now contribute more than 70% to the company’s total revenues. Caremark’s pharmacy operations contribute 33% to CVS/Aetna’s total revenues, and Optum Rx contributes 31% to UnitedHealth’s total revenues.
WHAT TO DO AND WHERE TO START
The official name of the ACA is the Patient Protection and Affordable Care Act. The law did indeed implement many important patient protections, and it made coverage more affordable for many Americans.
But there is much more Congress and regulators must do to close the loopholes and dismantle the barriers erected by big insurers that enable them to pad their bottom lines and reward shareholders while making health care increasingly unaffordable and inaccessible for many of us.
Several bipartisan bills have been introduced in Congress to change how big insurers do business. They include curbing insurers’ use of prior authorization, which often leads to denials and delays of care; requiring PBMs to be more “transparent” in how they do business and banning practices many PBMs use to boost profits, including spread pricing, which contributes to windfall profits; and overhauling the Medicare Advantage program by instituting a broad array of consumer and patient protections and eliminating the massive overpayments to insurers.
And as noted above, President Biden has asked Congress to broaden the recently enacted $2,000-a-year cap on prescription drugs to apply to people with private insurance, not just Medicare beneficiaries. That one policy change could save an untold number of lives and help keep millions of families out of medical debt. (A coalition of more than 70 organizations and businesses, which I lead, supports that, although we’re also calling on Congress to reduce the current overall annual out-of-pocket maximum to no more than $5,000.)
I encourage you to tell your members of Congress and the Biden administration that you support these reforms as well as improving, strengthening and expanding traditional Medicare. You can be certain the insurance industry and its allies are trying to keep any reforms that might shrink profit margins from becoming law.
In 46 states, once you choose Medicare Advantage at 65, you can almost never leave.
Medicare was founded in 1965 to end the crisis of medical care being denied to senior citizens in America, but private insurers have been able to progressively expand their presence in Medicare.
One of the biggest selling points of Obamacare was that it would finally end discrimination against patients on the basis of pre-existing conditions.
But for one vulnerable sector of the population, that discrimination never ended. Insurers are still able to deny coverage to some Americans with pre-existing conditions. And it’s all perfectly legal.
Sixty-five million seniors are in Medicare open enrollment from October 15 until December 7. Nearly 32 million of those patients are enrolled in Medicare Advantage, a set of privately run plans that have come under fire for denying treatment and overbilling the government.
Medicare Advantage patients theoretically have the option to return to traditional Medicare. But in 46 states, it is nearly impossible for those people to do so without exposing themselves to great financial risk.
Traditional Medicare has no out-of-pocket cap and covers 80 percent of medical expenses. Unlike Medicare Advantage plans, in traditional Medicare, seniors can choose whatever provider they want, and coverage limitations are far less stringent. Consequently, there’s a huge upside to going with traditional Medicare, and the downside is mitigated by the purchase of a Medigap plan, which covers the other 20 percent that Medicare doesn’t pay.
While this coverage is more expensive than most Medicare Advantage plans, nearly everybody in their old age would like to be able to choose their doctor and their hospitals, and everybody would want the security of knowing that they won’t be denied critical treatments. In 46 states, however, Medigap plans are allowed to engage in what’s called underwriting, or medical health screening, after seniors have already chosen a Medicare Advantage plan at age 65.
Only four states—New York, Connecticut, Maine, and Massachusetts—prevent Medigap underwriting for Medicare Advantage patients trying to switch back to traditional Medicare. The millions of Americans not living in those states are trapped in Medicare Advantage, because Medigap plans are legally able to deny them insurance coverage.
Medicare Advantage little resembles Medicare as it was traditionally intended, with tight networks and exorbitant costs that threaten to bankrupt the Medicare trust fund. (A recent estimate from Physicians for a National Health Program found that the program costs Medicare $140 billion annually.)
Jenn Coffey, a former EMT in New Hampshire who has been a vocal critic of her Medicare Advantage insurers’ attempts to deny her needed care, told the Prospect that she would jump back to traditional Medicare in a second. But because she became eligible prior to turning 65 due to a disability, she never had the option to pursue traditional Medicare with a Medigap plan. Instead, she pays premiums for a Medicare Advantage plan that nearly mirror what the cost of Medigap would be. But New Hampshire, like most other states, allows Medigap plans to reject her.
“I tried to find out if I could switch to traditional Medicare,” said Coffey. “When I talked to an insurance broker they said that I could. I made an appointment with an insurance agent, who then started looking at my pre-existing conditions, and they said, ‘We’re never going to get somebody to underwrite you.’”
Coffey was stunned by the agent’s words. “I honestly thought that we were completely done with pre-existing conditions” as a determinant for insurance coverage, she said. “Medigap plans are the only place where they are allowed to discriminate against us.”
Medicare Advantage now covers a majority of Medicare participants, thanks to extremely aggressive marketing and perks for healthier seniors like gym memberships.
In the 46 states that lack protections for people with pre-existing conditions, “lots of people don’t know that they may not be able to buy a Medigap plan if they go back to traditional Medicare from Medicare Advantage,” said Tricia Neuman, a senior vice president at KFF who has studied this particular issue.
Technically speaking, they can still go back to traditional Medicare if they don’t like their Medicare Advantage options, Neuman explained. But without access to a Medigap plan, they would be on the hook for 20 percent of their medical costs, which is unaffordable for most seniors.
Neuman told the Prospect about “cases where people have serious medical problems, and wanted to see a specialist,” but were blocked by their Medicare Advantage plan. Those same people had no ability to switch to traditional Medicare with a Medigap plan at precisely the time they need it the most, in nearly every state in the U.S.
“Medigap wasn’t a part of the ACA discussion on pre-existing conditions,” Neuman added. “A lot of people have no idea about this restriction on Medicare coverage, until they find themselves in a position that they want to go back and then it could be too late.”
Academic research shows that seniors often seek to return to traditional Medicare when they become sick.
The critical component that both Medigap and Medicare Advantage plans offer, which traditional Medicare does not, is out-of-pocket caps, said Cristina Boccuti, a director at the West Health Policy Center. “People who want to leave their Medicare Advantage plan, maybe because they are experiencing problems in their plan’s network, decide to disenroll and can’t obtain an out-of-pocket limit which they had previously had in Medicare Advantage,” Boccuti said.
That’s exactly the problem facing Rick Timmins, a retired veterinarian in Washington state. When Timmins was continually delayed care for melanoma, he explored getting out of his Medicare Advantage plan. “I wanted out of Medicare Advantage big-time,” said Timmins. But when he began to look at Medigap plans, he was told that he wouldn’t be guaranteed to get a plan, and that the insurance company could raise premiums based on a pre-existing condition.
“I doubt that I’ll be able to switch over to traditional Medicare, as I can’t afford high premiums,” Timmins said. “I’m still paying off some old medical debt, so it adds to my medical expenses.”
Medicare was founded in 1965 to end the crisis of medical care being denied to senior citizens in America. “No longer will older Americans be denied the healing miracle of modern medicine,” Lyndon Johnson said at the time. “No longer will illness crush and destroy the savings that they have so carefully put away over a lifetime so that they might enjoy dignity in their later years. No longer will young families see their own incomes, and their own hopes, eaten away simply because they are carrying out their deep moral obligations to their parents, and to their uncles, and their aunts.”
But slowly, private insurers were able to progressively expand their presence in Medicare, with a colossal advance made through George W. Bush’s Medicare prescription drug program in 2003. Now, Medicare Advantage covers a majority of Medicare participants, thanks to extremely aggressive marketing and perks for healthier seniors like gym memberships.
Numerous recent studies have shown Medicare Advantage plans to deny care while boosting the profits of private insurance companies. Defenders of Medicare Advantage argue that managed care—which practically speaking means insurance employees denying care to seniors—improves our health care system.
Denial-of-care issues,
combined with the aforementioned $140 billion drain on the trust fund, have attracted far more scrutiny of the program than in years past. Community organizations like People’s Action, along with other groups like Be A Hero, have stepped up their criticism of the program. The Biden administration proposed new rules this year to curb overbilling through the use of medical codes, but a furious multimillion-dollar lobbying campaign from the health insurance industry led to the rules being implemented gradually.
Still, members of Congress have become more emboldened to speak out against abuses in Medicare Advantage. A recent Senate Finance Committee hearing featured bipartisan complaints about denying access to care. And House Democrats have urged the Centers for Medicare & Medicaid Services to crack down on increases in prior authorizations for certain medical procedures, as well as the use of artificial-intelligence programs to drive denials.
Megan Essaheb, People’s Action’s director of federal affairs, said that Medicare Advantage has become a drain on the federal trust fund. “These private companies are making tons of money,” Essaheb said. “The plans offer benefits on the front end without people understanding that they will not get the benefits of traditional Medicare, like being able to choose your doctor.”
Despite the growing scrutiny, the trapping of patients who want to get out of Medicare Advantage hasn’t gotten as much attention from either Congress or state legislatures that could end the practice.
Coffey, the retired EMT from New Hampshire, told the Prospect that she has paid $6,000 in out-of-pocket expenses this year under a Medicare Advantage program. “If I could go to Medigap, I would have better access to care, I wouldn’t be forced to give up Boston doctors,” she said.
“These insurance companies are allowed to reap as much profit as possible for as little service as they can get away with. They pocket all of our money and they don’t pay for anything, they sit there and deny and delay.”
The rebates that will be issued later this year will be larger than those issued in most prior years, the analysis found.
Health insurers are projected to pay about $1.1 billion in Affordable Care Act medical loss ratio rebates this year, a new KFF report finds.
The medical loss ratio (MLR) provision of the ACA limits the amount of premium income that insurers can keep for administration, marketing and profits. Insurers that fail to meet the applicable MLR threshold are required to pay back excess profits or margins in the form of rebates to individuals and employers that purchased coverage.
The $1.1 billion in estimated total rebates across commercial markets are similar to the $1 billion in total rebates issued in 2022, and the $950 million issued in 2023. Last year, rebates were issued to 1.7 million people with individual coverage and 4.1 million people with employer coverage. In the individual market, the 2023 average rebate per person was $196, while the average rebates per person for the small group market and the large group market were $201 and $104, respectively.
The rebates, to be issued later this year, will be larger than those issued in most prior years, the analysis found, but they’ll fall short of the recent rebate totals of $2.5 billion issued in 2020 and $2 billion issued in 2021, which coincided with the onset of the COVID-19 pandemic.
WHAT’S THE IMPACT?
In the individual and small group markets, insurers are required to spend at least 80% of their premium income on healthcare claims and quality improvement efforts, leaving the remaining 20% for administration, marketing expenses and profit.
The MLR threshold is higher for large group insurers, which have to spend at least 85% of their premium income on healthcare claims and quality-improvement efforts.
MLR rebates are based on a three-year average, meaning that rebates issued in 2024 will be calculated using insurers’ financial data in 2021, 2022 and 2023, and will go to people and businesses who bought health coverage in 2023.
In 2023, the average individual market simple loss ratio – meaning there’s no adjustment for quality improvement expenses or taxes, and doesn’t align perfectly with ACA MLR thresholds – was 84%. That shows insurers spent an average of 84% of their premium income in the form of health claims in 2023, according to KFF data.
However, rebates issued in 2024 are based on a three-year average of insurers’ experience in 2021-2023. Consequently, even insurers with high loss ratios in 2023 may expect to owe rebates if they were highly profitable in the prior two years.
In the small and large group markets, 2023 average simple loss ratios were 84% and 88%, respectively. Only fully insured group plans are subject to the ACA MLR rule, while roughly two-thirds of covered workers are in self-funded plans, to which the MLR threshold doesn’t apply.
THE LARGER TREND
KFF cautioned that the rebate amounts are still preliminary. Rebates and notices are mailed out by the end of September, and the federal government will post a summary of the total amount owed by each issuer in each state later in the year.
Insurers in the individual market can either issue rebates in the form of a check or premium credit. For people with employer coverage, the rebate can be shared between the employer and the employee, depending on the way in which they share premium costs.
If the amount of the rebate is exceptionally small – less than $5 for individual rebates and less than $20 for group rebates – insurers are not required to process the rebate, as it may not warrant the administrative burden required to do so, KFF said.
In recent years, the Medicare Advantage (MA) program enjoyed both rapid membership growth and positive attention from healthcare organizations and advocates. As of the beginning of 2024, 33.4 million Americans were enrolled in MA, up 7% from 2023.
More than half of all Medicare-eligible individuals are now enrolled in MA.
Interest and growth in MA has been buoyed by a number of factors: a growing eligible population as Baby Boomers continue to age into Medicare eligibility; affordable benefit packages with low or zero monthly premiums; regulatory changes providing for more flexibility in plan and member design; consumer-centric programs and care models tailored to the needs of beneficiaries; increased marketing and sales efforts through direct mailings, telemarketing, and online advertising.
The program has also delivered meaningful value to members, who are more likely than traditional Medicare beneficiaries to have an annual income less than $40,000. In addition, the average monthly premium for Medicare beneficiaries enrolled in an MA plan has dropped by almost one-third in the last four years, reaching $18 per month in 2023.
Ideally, success in MA can take the form of a virtuous cycle: an improved margin on MA for a plan enables reinvestment in related products to grow membership and better manage health outcomes, which leads to further reinvestment (Figure 1). Sustained success is contingent on meaningful collaboration between payers and providers.
FIGURE 1: The Virtuous Cycle of MA Success
MA Hits Headwinds
However, after several high-growth years, payers and providers are currently confronting multiple MA-related challenges. Many providers have recently posted losses as their contractual yields decrease and authorizations for care have become more restrictive. The bar for risk adjustment and Star Ratings is also rising. Only 6% of plans received a 5-star rating from the Center for Medicare & Medicaid Services (CMS) for 2024, down from 22% in 2023. CMS also recently confirmed plans for rate cuts in 2025, with critics arguing that benefits for beneficiaries may become more limited. Providers are also reeling from related bureaucratic headaches.
Current MA members also have expressed concerns with the program’s trajectory. While roughly two-thirds of MA and traditional Medicare beneficiaries recently surveyed by the Commonwealth Fund said their coverage has met their expectations, MA members were more likely to report delays in care while awaiting prior approval (22% vs. 13%) or difficulty affording care due to copayments or deductibles (12% vs. 7%).
Despite current challenges, many providers and health plans believe they need to continue to participate in and/or prioritize MA, given the program’s scale and overall benefits to their organizations and the communities they serve.
For instance, the success of MA risk contracts predicated on collaborating around delivering healthcare value suggests a possible path forward.
According to a JAMA study of more than 300,000 Medicare Advantage beneficiaries, members in value-based care MA arrangements with risk for both payers and providers had lower rates of inpatient admission, emergency department visits, and readmissions. In addition, CMS’s robust risk scoring model ensures that providers are paid fairly for the true cost of providing care to the populations they serve.
Percent of premium contracts, where payers delegate a share of the premium to providers to manage, are predictable, align payer and provider interests, easy to understand, and increasingly common.
In addition, the high cost of caring for Medicare enrollees makes the population health focus on VBC arrangements economical. Medicare members have the highest utilization of any insurance class, so intensive services like care management, disease management, and care coordination are more likely to have a positive return on investment.
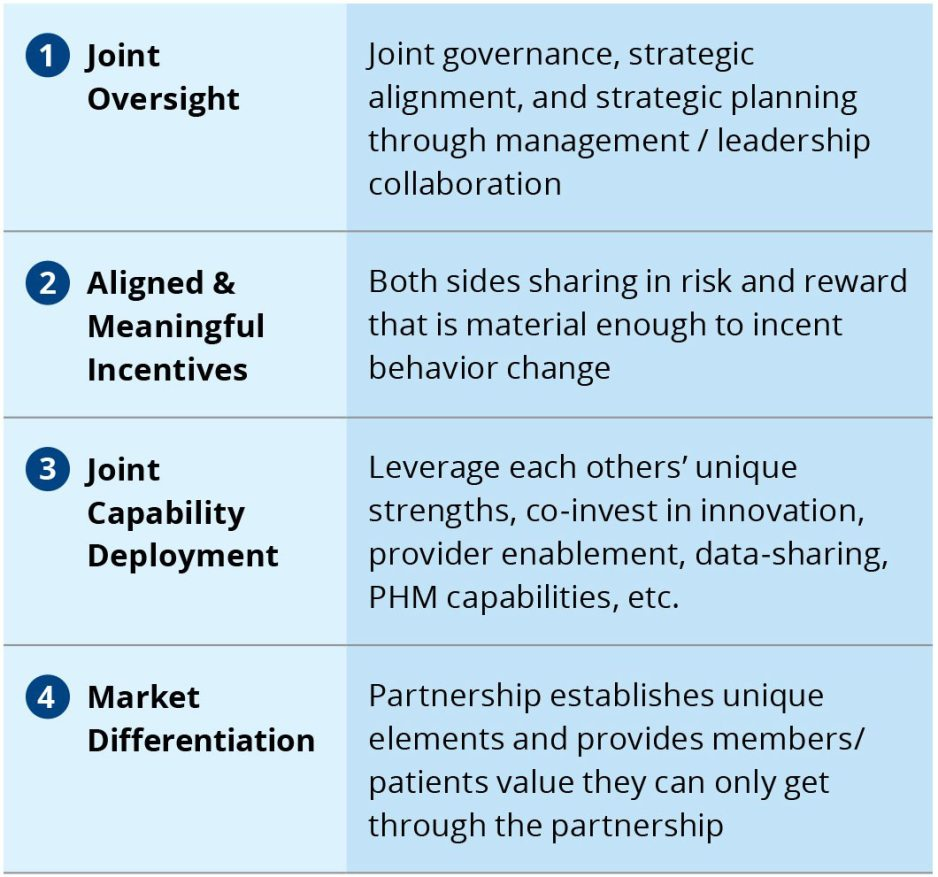
Successful VBC arrangements share several core tenets, grounded in the need for close collaboration between participating parties (Figure 2).
FIGURE 2: Core Tenets of Successful Payer-Provider Value-Based Care Models
However, VBC arrangements are not the only option. Value-centric collaborations can take on a wide range of forms, depending on the amount of risk providers are willing to assume and the partnerships’ risk-related capabilities. The full continuum of value-centric collaborations runs the gamut from shared savings contracts with no downside risk for providers to full vertical integration into a single organization (Figure 3).
FIGURE 3: Understanding the Continuum of Value-Based Care Arrangements
Looking Into the Crystal Ball: Three Future State Scenarios
As the MA market confronts new headwinds after years of growth and favorable attention, we anticipate three possible future state scenarios. These possibilities can be applied to both the outlook nationally, as well as the actions of payers and providers within specific markets.
Scenario 1: A renewal of growth
In this scenario, better sense prevails, and plans and providers collaborate to address the core issues facing the program. A pause/adjustment in the market is followed by a period of renewed growth. From a national standpoint, this scenario is contingent on neutral to favorable regulatory treatment.
Scenario 2: Uneasy stabilization
In this scenario, contention is partially resolved through some degree of collaboration between payers and providers. This scenario is also dependent on neutral to favorable regulatory treatment.
Scenario 3: Implosion
In this scenario, high levels of contention continue, and more providers go out of network. Middle-income Medicare members opt out of MA and go back to traditional Medicare when feasible. This scenario accounts for heightened regulatory pressure on risk adjustment and utilization management practices, which further pressures margins.
Conclusion
Despite MA’s recent, publicly documented challenges, the program now accounts for more than half of all Medicare beneficiaries—a patient population that every healthcare organization must engage in some form or fashion.
As providers and payers decide how to approach the program—and each other—amid uncertainty and contention, the path forward can appear unclear. However, healthcare leaders seeking to emerge from the current environment of MA contention have an opportunity to shape the future of MA and will play a major role determining which of the three scenarios outlined in this article comes to fruition.
Ultimately, organizations must be able to develop a business model that both delivers quality care and manageable per capita costs—and critically, find ways to work through today’s pressing concerns with other MA stakeholders and partners.
One of the things I’ve always found most fascinating about news coverage and policymaker attention to health insurers is how little focus is placed on what these companies say to their investors.
It’s no secret that each quarter, all public companies update their shareholders and provide guidance for the future. When I was at Cigna, preparing the CEO to speak with reporters and investor analysts was arguably considered the most important role I had every three months.
Mining insights from those earnings reports has been a focus of mine since I became an insurance industry whistleblower. Recently, for example, we’ve highlighted how CVS/Aetna, in particular, has taken a beating on its stock price for reporting increased spending on medical care by seniors in Medicare Advantage plans.
Now, though, CEOs have become even more public and open, beyond their quarterly earnings calls, about the challenges they are having extracting further profit from the Medicaid and Medicare programs. This should be noted, particularly by the bipartisan group of lawmakers in Washington increasingly eyeing regulatory reform on insurer practices like prior authorization, as evidence that insurers are going to become even more aggressive in limiting care to preserve their 2024 profits.
Centene’s CEO saida few days ago that medical claims are increasing in the company’s managed Medicaid business. UnitedHealth and Elevance, which owns several Blue Cross Blue Shield companies that have converted to for-profit status, also recently reported they’re seeing similar results. Combined with increased medical spending on Medicare Advantage claims, one might guess this would begin to worry investors that insurers would lower their profit forecasts.
But none of these companies have so far expressed concern about not meeting their 2024 profit expectations.
So, medical claims in Medicaid and Medicare Advantage plans – now the majority of the business for many of the largest insurers – are rising, but these companies aren’t expecting to disappoint Wall Street with a drop in profits. How is that possible?
Because insurers can deploy the tools to prevent patients from accessing care. And their playbook isn’t secret, or complicated.
By further increasing prior authorization in Medicaid and Medicare Advantage plans, insurers can limit how many seniors and low-income Americans follow through with legitimate care and procedures. (Here’s a recent congressional report on increased hurdles insurers have put in place to prevent children from receiving preventive care in Medicaid plans. And insurers’ increasing use of prior authorization in Medicare Advantage is something we’ve regularly covered.)
Unlike their marketplace and employer-based plans, insurers can’t negotiate reimbursement rates for Medicaid and Medicare Advantage plans that they manage.
But beyond prior authorization, they can put other layers of bureaucracy in place that increase how long it takes a provider to be reimbursed for providing care – and to make it more complicated for doctors to ensure they’re reimbursed fully for the care they provide.
In effect, these tactics can amount to decreasing the already industry-low rate of reimbursement for doctors from the Medicaid and Medicare Advantage programs. Physicians, you should expect to see more hurdles to reimbursement in these programs throughout the balance of 2024 as insurers look to hoard as much cash as they can.
In Medicare Advantage plans, insurers can pursue the industry jargon of a “benefit buydown” to further shift costs onto plan enrollees and off insurers themselves. Because the federal government pays insurers a flat amount per Medicare Advantage enrollee, regardless of how much health care spending each patient has, it is in the insurers’ financial interest to claim that seniors and disabled people enrolled in their plans are sicker than they really are.
Rising out-of-pocket costs that seniors and disabled people in Medicare Advantage plans are facing is a consequence of insurers wanting to squeeze further profits out of the program, and is a way to maintain direct government payments per enrollee within the insurers’ coffers.
On the one hand, the alternative to traditional Medicare is still popular among consumers, who have been lured by the promises of lower out-of-pocket costs and increased supplemental benefits.
On the other hand,Medicare Advantage profitability is on the decline, as shown in recent quarterly reports from the large insurers. The headwinds, executives said during recent earnings calls, have been due to greater than expected utilization of benefits and lower than expected reimbursement from the government.
Adding to MA’s margin challenges are providers who are making the decision to cut their ties with MA plans rather than deal with delays in prior authorization and claims payments.
Moody’s Investors Service said this year, and an HFMAsurvey from March indicates 19% of health systems have discontinued at least one Medicare Advantage plan, while 61% are planning to or considering dropping Medicare Advantage payers.
Until recently, the story of Medicare Advantage was one of ascendancy. Just last year it hit a milestone: More than half of eligible Medicare beneficiaries are now in MA plans. So why is business taking a step back?
WHY THIS MATTERS
There are many factors at play, but a big one is the 3.7% rate increase for 2025 that Medicare Advantage plans will receive from the Centers for Medicare and Medicaid Services. The federal government is projected to pay between $500 and $600 billion in Medicare Advantage payments to private health plans, according to the 2025 Advance Notice for the Medicare Advantage and Medicare Part D Prescription Drug Programs released in April.
The payment rate was considered inadequate by insurers, who were also troubled over other key factors, including a 0.16% reduction in the Medicare Advantage benchmark rate for 2025, which represents a 0.2% decrease.
“AHIP has strong concerns that the estimated growth rate in the Advance Notice – an average of 2.44% – will lead to benchmark changes that are insufficient to cover the cost of caring for 33 million MA beneficiaries in 2025,” AHIP president and CEO Mike Tuffin said in April. “The estimate does not reflect higher utilization and cost trends in the healthcare market that are expected to continue into 2025.”
According to Karen Iapoce, vice president Government Programs at ZeOmega, the cost of running an MA business is increasing due to the burdens being placed on health plans.
“If you sit inside with a health plan, they’re asked to do a lot with not as much bandwidth as they had before,” said Iapoce. “For example, health equity requires plans to have new regulatory guidance they need to meet. There’s a host of measures around health equity. Our plans are not in the business of really understanding how to manage transportation, how to manage housing, so they’re working with other entities. This requires an expert to sit in with the health plan … and then track and report. On the business end, they want to show an ROI, but that could be six months or a year down the line.”
Because of that, she said, the benchmark rate is likely insufficient to cover the projected increase in administrative and other costs. Iapoce said the benchmark rates represent the maximum amount that will be paid to a person in a given county; this is used as a reference point for calculation. If a plan is higher than the benchmarks, the premiums end up going to the beneficiary. More commonly, the plans bid below the benchmark, and the difference represents the rebate plans will receive. But they also factor into risk adjustment.
“The plans are getting into these contract negotiations, so they have to know what goes into that benchmark,” said Iapoce. “I might not be a high utilizer, but you may be. If we’re bringing in a community of high utilizers, there’s no one offsetting that. There’s no balance.”
Richard Gundling, senior vice president, content and professional practice guidance at HFMA, said MA plans started running into these issues when the program crossed over the threshold of more than 50% of beneficiaries.
“When a Medicare Advantage plan comes in, then all the extra administrative burdens come into play,” said Gundling. “So you have prior authorizations, all the issues around lack of payment and denials. Patients get caught in the middle, and in particular elderly patients think they’re still on traditional Medicare.
“It used to be that healthier beneficiaries went into Medicare Advantage,” he added. “Sicker beneficiaries tended to stay in traditional Medicare. That’s not the case anymore, and so there’s a higher spend.”
Gundling said beneficiaries are likely flocking to MA with visions of lower costs and increased benefits such as eyeglasses and hearing aids, and many don’t realize the tradeoffs, such as prior authorizations and network restrictions.
MA remains popular with seniors, but studies show the plans cost the government more money than original Medicare.
A 2023 Milliman report showed annual estimated healthcare costs per beneficiary are $3,138, compared to $5,000 for traditional fee-for-service Medicare, and over $5,700 if a traditional Medicare beneficiary also buys a Medigap plan.
MA membership has grown nationally at an annual rate of 8% to approximately 32 million, while traditional Medicare has declined at an average annual rate of 1%. As that has happened the percentage of people choosing MA has grown to 49% from 28%, data shows.
Yet Medicare Advantage profitability is on the decline, Moody’s found in February. That’s largely because of a significant spike in utilization for most of the companies, which Moody’s expects will result in lower full-year MA earnings for insurers. Adding to that is lower reimbursement rates for the first time in years that are likely to remain weaker in 2025 and 2026, which is credit negative.
Moody’s analysts contend that MA may have “lost its luster,” citing as evidence Cigna’s efforts to sell its MA business, even after a failed merger with Humana.Cigna this past winter announced it had entered into a definitive agreement to sell its Medicare Advantage, Supplemental Benefits, Medicare Part D and CareAllies businesses to Health Care Service Corporation (HCSC) for about $3.7 billion.
Iapoce said Medicare Advantage may be a victim of its own success.
“Because of all this great promotion about what a Medicare Advantage plan can do for you, you’re seeing an increase in enrollment, or more people moving over, and the demographics are starting to change,” she said.
For many consumers, the appeal of an MA plan is the same as that of an online retailer like Amazon, said Iapoce. Such retailers offer one-stop shopping for a variety of goods, and the perception is that MA essentially offers one-stop shopping for a variety of healthcare services and benefits.
But while this massive shift is happening, it puts providers in an awkward position, said Iapoce.
“Their reimbursement is almost being dictated, in essence, by a health plan,” she said. “It almost feels like the payer has the upper hand over the provider. Think: I’m a provider. It’s my job to get this female with this particular age and condition a mammogram, and the health plan has told me to get her a mammogram. But you, as the health plan, get the money for it. I, as the provider … what am I getting? What’s it doing for me? It becomes this very tense situation, and the provider is probably the entity that is running on the thinnest of staff.”
Gundling expects that despite some “growing pains,” MA will remain viable and continue to grow.
“Nobody’s going to stay still,” said Gundling. CMS has to consider, ‘Are we paying the health plans appropriately for the types of patients they have?’ And then health plans will need to look at their medical utilization rules – ‘Are we overdoing pre-authorization or denying things appropriately?’ And providers need to say, ‘This is a market we need to continue to grow.’
“There’s still going to be a role for it,” he said. “It’s just that we’ve introduced a larger population into it, and I think that’s where a lot of the surprises come in.”
THE LARGER TREND
CVS reportedearlier this month that healthcare-benefits medical costs, primarily due to higher-than-expected Medicare Advantage utilization, came in approximately $900 million above expectations.
Last month, Humana said it expected membership may take a hit from future Medicare Advantage pricing resulting from the CMS payment rate notice. Humana is actively evaluating plan level pricing decisions and the expected impact to membership, president and COO James Rechtin said on the call.
Elevance Health, formerly Anthem, reported a 12.2% earnings increase for Q1, but company margins have not been as affected as those insurers that are heavily invested in the MA market. Fewer of its members are in MA plans compared to other large insurers Humana, CVS Health or UnitedHealth Group, executives said.
Speaking of Andrew Witty, the UnitedHealth chief spurred a freakout last week on Wall Street after he said the company was beginning to see a “disturbance” in its Medicaid medical costs. More people on Medicaid are going to the doctor and hospital, which eats into the insurance company’s profits.
The biggest insurers that run state Medicaid programs — UnitedHealth, Elevance Health, Centene, and Molina Healthcare — all saw their stocks take a dive after Witty’s disclosure. For the past year, the surge in medical services has mostly been confined to older adults in Medicare Advantage plans.
Wall Street largely did not account for that trend creeping into Medicaid, which covers low-income people.
This switch is largely a function of the government’s Medicaid “redeterminations” process, Centene CEO Sarah London said at a banking conference Friday. During the pandemic, states didn’t have to kick people off Medicaid if they no longer were eligible. But over the past year, states had to redetermine if someone still qualified for coverage, and to boot those that no longer did. As fewer people remain enrolled in Medicaid, the ones who have stayed are sicker and are getting more care.
Looking ahead, London told investors not to worry. That’s because Centene and other insurers will get more money from state Medicaid programs (translation: taxpayers) over the next several months, through routine payment updates, to match how sick its enrollees are. The explanation worked: The stocks of all the Medicaid insurers rose on Friday.
“We know how to do this,” London said. “This dynamic of redeterminations is unprecedented right now because of the scale. But matching rates to acuity in Medicaid is normal course.”
As campaigns for November elections gear up for early voting and Congress considers bipartisan reforms to limit consolidation and enhance competition in U.S. healthcare, prospective voters are sending a cleat message to would-be office holders:
Healthcare Affordability must be addressed directly, transparently and now.
Polling by Gallup, Kaiser Family Foundation and Pew have consistently shown healthcare affordability among top concerns to voters alongside inflation, immigration and access to abortion. It is higher among Democratic-leaning voters but represents the majority in every socio-economic cohort–young and old, low and middle income and households with/without health insurance coverage., urban and rural and so on.
It’s understandable: household economic security is declining: per the Federal Reserve’s latest household finances report:
72% of US adults say they are doing well financially (down from 78% in 2021)
54% say they have emergency savings to cover 3 months expenses ($400)—down from high of 59% in 2015.
69% say their finances deteriorated in 2023. They’re paying more for groceries, fuel, insurance premiums and childcare.
Renters absorbed a 10% increase last year and mortgage interest spike has put home ownership beyond reach for 6 in 10 households
Thus, household financial security is the issue and healthcare expenses play a key role. Drug prices, hospital consolidation, price transparency and corporate greed will get frequent recognition in candidate rhetoric. “Reform” will be promised. And each sector in the industry will offer solutions that place the blame on others.
Granted, the U.S. health system lacks a uniform definition of healthcare affordability. It’s a flaw. In the Affordable Care Act, it was framed in the context of an individual’s eligibility for government-subsidized insurance coverage (8.39% adjusted gross income for households between 100% and 400% of the federal poverty level). But a broader application to the entire population was overlooked. Nonetheless, economists, regulators and consumers recognize the central role healthcare affordability plays in household financial security.
Handicapping the major players potential to win the hearts and minds of voters about healthcare affordability is tricky:
Each major sector has seen the ranks of its membership decrease and the influence (and visibility) of its bigger players increase. They’re easy targets for industry critics.
Each sector is seeing private equity and non-traditional players play bigger roles. The healthcare landscape is expanding beyond the traditional players.
Each sector is struggling to make their cases for incremental reforms while employers, legislators and consumers want more. Bipartisan support for anything is a rarity: an exception is antipathy toward healthcare consolidation and lack of price transparency.
All recognize that affordability is complicated. Unit cost and price increases for goods and services are the culprit: excess utilization is secondary.
Against this backdrop, here’s a scorecard on the current state of preparedness as each navigates affordability going into Campaign 2024:
Sector
Advantages
Disadvantages
Handicap Score1=Unprepared to5=Well Prepared
Hospitals
Community presence (employer, safety net) Economic impact Influence in Congress Scale: 30% of spending + direct employment of 52% of physicians Access to capital
Lack of costs & price transparency Unit costs inflation due to wage, supply chain & admin Shifting demand for core services. Low entry barriers for key services Regulator headwind (state, federal). Operating, governing culture Value proposition erosion with employers, pre-Medicare populations Consumer orientation
3
Physicians
Consumer trust Influence in Congress Shared savings (Medicare) Essentiality Specialization Access to technology
Care continuity Inadequacy of primary care Disorganization (fragmentation) Value of shared savings to general population (beyond Medicare) Culture: change-averse (education, licensing performance measurement, et al) Data: costs, outcomes
2
Drug Manufacturers
Increasing product demand Influence in Congress Public trust in drug efficacy Insurance structure that limits consumer price sensitivity to OOP Potential for AI -enabled discovery, market access Access to private capital Congress’ constraint on PBMs
Unit cost escalation Lack of price transparency Growing disaffection for FDA Long-term Basic Research Funding State Price Control Momentum Market access Restrictive Formulary Growth Transparency in Distributor-PBM business relationships Public perception of corporate greed
2
Health Insurers
Availability of claims, cost data Employer tax exemptions Growing government market Plan design: OOP, provider access Public association: coverage = financial security Access to private capital
Escalating premiums Declining group market Growing regulatory scrutiny (consolidation, data protection) Tension with health systems Value proposition erosion among government, employers, consumers
4
Retail Health
Non-incumbrance of restrictive regulatory framework Consumer acceptance Breadth of product opportunities Access to private capital Opportunity for care management (i.e. CVS- Epic) Operational orientation to consumers (convenience, pricing, et al) Potential with employers,
Lack of access, coordination with needed specialty care Threat of regulatory restraint on growth Risks associated with care management models
3
The biggest, investor-owned health insurers own the advantage today. As in other sectors, they’re growing faster than their smaller peers and enjoy advantages of scale and private capital access to fund their growth. A handful of big players in the other sectors stand-out, but their affordability solutions are, to date, not readily active.
In each sector above, there is consensus that a fundamental change in the structure, function and oversight of the U.S. health is eminent. In all, tribalism is an issue: publicly-owned, not for profits vs. investor-owned, independent vs. affiliated, big vs. small and so on.
Getting consensus to address affordability head on is hard, so not much is done by the sectors themselves. And none is approaching the solution in its necessary context—the financial security of a households facing unprecedented pressures to make ends meet. In all likelihood, the bigger, more prominent organizations in their ranks of these sectors will deliver affordability solutions well-above the lowest common denominators that are comfortable for most Thus, health care affordability will be associated with organizational brands and differentiated services, not the sectors from which their trace their origins. And it will be based on specified utilization, costs, outcome and spending guarantees to consumers and employers that are reasonable and transparent.