Several hospitals in Los Angeles County are preparing for the possibility of restrategizing care delivery in the coming weeks amid growing COVID-19 hospitalizations, according to the Los Angeles Times.
Los Angeles County reported 6,018 COVID-19 hospitalizations Dec. 20 — a 2.5 percent increase from the day prior — with 1,198 patients in ICUs, according to the state’s data dashboard. Statewide, 17,750 patients are hospitalized with COVID-19, 3,710 of them in ICUs.
The LA Times obtained a document recently circulated among physicians at the four county-run hospitals that outlines resource allocation in crisis situations. The guidelines call for physicians to save as many patients as possible versus trying everything to save a patient, meaning those less likely to survive will not receive the level of care they would have otherwise. L.A. County Health Services Director Christina Ghaly, MD, told the LA Times that the guidelines were not in place as of Friday night.
California activated its “mass fatality” program last week, which coordinates mutual aid across several government agencies when more deaths take place in a period of time than can be handled by local coroner or medical emergency personnel, NPR reports.
Nearly all of the state is under stay-at-home orders, with residents prohibited from gathering with anyone outside their immediate household.
“I have yet to see any clear signals that things are slowing down, and I’m very concerned about the next two months,” Timothy Brewer, MD, an epidemiologist with UCLA Health, told the LA Times. He said UCLA Health is scheduling several infectious disease specialists to be on call at any time, and the biggest issue is that hospitals may quickly run out of providers who can administer ICU-level care.
Congressional leaders have reached an agreement on a $900 billion COVID-19 relief package and $1.4 trillion government funding deal with several healthcare provisions, according to Senate Majority Leader Mitch McConnell, R-Ky., and Minority Leader Chuck Schumer, D-N.Y.
Here are seven things to know about the relief aid and funding deal:
1. Congressional leaders have yet to release text of the COVID-19 legislation, but have shared a few key details on the measure, according to CNBC.Becker’s breaks down the information that has been released thus far.
2. The COVID-19 package includes $20 billion for the purchase of vaccines, about $9 billion for vaccine distribution and about $22 billion to help states with testing, tracing and other COVID-19 mitigation programs, according to Politico.
3. Lawmakers are also expected to include a provision changing how providers can use their relief grants. In particular, the bill is expected to allow hospitals to calculate lost revenue by comparing budgeted revenue for 2020. Hospitals have said this tweak will allow them to keep more funding.
4. The agreement also allocates $284 billion for a new round of Paycheck Protection Program loans.
5. The COVID-19 relief bill also provides$600 stimulus checks to Americans earning up to $75,000 per year and $600 for their children, according to NBC. It also provides a supplemental $300 per week in unemployment benefits.
6. The year-end spending bill includes a measure to ban surprise billing. Under the measure, hospitals and physicians would be banned from charging patients out-of-network costs their insurers would not cover. Instead, patients would only be required to pay their in-network cost-sharing amount when they see an out-of-network provider, according to The Hill.The agreement gives insurers 30 days to negotiate a payment on the outstanding bill. After that period, they can enter into arbitration to gain higher reimbursement.
7. Lawmakers plan to pass the relief bill and federal spending bill Dec. 21.
As the first Americans receive COVID vaccines, supplies remain limited even for the highest-risk populations. And with doses now in the pipeline, states are facing more intense questions about how they will prioritize vaccine delivery across demographic and at-risk groups. The graphic above shows an estimated vaccination timeline, based on the Centers for Disease Control and Prevention’s (CDC) recommended schedule. It illustrates the relative size of different populations in each allocation phase, along with the likely difficulty of targeting them and verifying eligibility. The first phase is divided into three waves (1a, 1b, 1c) for at-risk populations and essential workers, while the second phase includes the rest of the adult population, as well as children (though pediatric clinical trials are still in early stages).
Unsurprisingly, the CDC recommends that those most at risk for infection and severe disease—healthcare workers and nursing home residents—receive the 20M doses available by year’s end.While most states are generally adhering to the initial recommendations on priority groups for phase 1a set by the CDC’s Advisory Committee on Immunization Practices (ACIP), several have made adjustments. At least three are including law enforcement personnel in phase 1a, and others are further categorizing healthcare workers into high-, medium-, and low-risk groups. This weekend, ACIP will reconvene to create its official recommendations for phases 1b and 1c, which include the much larger populations of adults over age 65, and those with high-risk medical conditions.
Beyond eligibility guidelines, larger questions loom. How would someone “verify” that they have a high-risk condition? Who will reach out to older Americans to let them know they are eligible, and where to access the vaccine? As vaccine rollout continues, providers should anticipate the role they will likely play in managing patients “in the queue”, documenting eligible conditions and establishing regular information channels to keep people informed about the current status of vaccine planning and access.
But first, we have a difficult period to get through. This week again saw record-breaking numbers of cases, hospitalizations, and deaths from COVID-19, with Thursday alone bringing more than 238,000 new cases—and a staggering 3,293 fatalities.
Nearly 115,000 Americans are currently hospitalized with COVID, a rise of 16 percent from just two weeks ago, and in many places a precarious capacity situation has turned perilous. Conditions have worsened precipitously in California, with only Tennessee, Oklahoma, and Rhode Island registering more daily COVID cases per 100,000 population than the Golden State, although cases are still on the rise across 80 percent of states and territories.
Intensive care availability in Southern California hit zero, with ICU volume there expected to double or triple by this time next month. The same stresses are playing out in dozens of markets across the country, leading to a staffing sustainability crisis that can’t be solved through paying overtime, cancelling vacations or looking to travel nurses to fill the gaps in a now nationwide crisis. With the Christmas and New Year’s holidays still ahead, experts predictCOVID cases won’t peak until sometime in mid-January, with a peak in hospitalizations and deaths following several weeks after.
Several states and cities tightened restrictions on gatherings and issued new stay-at-home orders, in an effort to keep new cases at a level that allows hospitals to manage through the next several weeks and maintain care quality and access for COVID and non-COVID patients alike. The coming weeks will require every American to take greater precautions than at any time during the course of this pandemic.
An Oregon physician who publicly spoke out against wearing a mask to slow the spread of COVID-19 has had his medical license suspended, according to The Washington Post.
In a written order Dec. 4, the Oregon Medical Board suspended the license of Steven A. LaTulippe, MD, a family medicine physician at South View Medical Arts in Dallas, Ore. The board alleges Dr. LaTulippe engaged in “conduct that is contrary to medical ethics and does or might constitute a danger to the health or safety of the public.”
It also accuses him of “gross negligence.”
Specific acts cited in the letter include the physician’s alleged advice to a Medicaid patient. According to the board, the patient contacted Dr. LaTulippe’s medical clinic in July for guidance on COVID-19 and was told asymptomatic people should not be tested, that wearing masks does not prevent virus transmission, and the patient was told not to self-isolate because exposure to others would provide COVID-19 immunity.
The board said the patient seeking the guidance from Dr. LaTulippe’s clinic was terminated as a patient after questioning the appropriateness of the guidance.
The board also contends workers in Dr. LaTulippe’s clinic refuse to wear masks at work and urge people who enter the clinic wearing masks to remove them.
Dr. LaTulippe “regularly tells his patients that masks are ineffective in preventing the spread of COVID-19 and should not be worn”; “directs patients to a YouTube video providing false information about mask-wearing” ; and “regularly advises, particularly for his elderly and pediatric patients, that it is ‘very dangerous’ to wear masks because masks exacerbate [chronic obstructive pulmonary disease] and asthma and cause or contribute to multiple serious health conditions,” according to the board.
The Post could not immediately reach Dr. LaTulippe for comment Dec. 5.
In a recent interview, Dr. LaTulippe told NBC News he believes there is “bad science behind” wearing masks.
“I have absolutely zero problems with infectivity, and I have completely successful treatments, so I ask, ‘What is the problem?’ Why would I be demonized if I know what I’m doing?” he told the news network.
The CDC has advocated wearing masks to combat COVID-19.
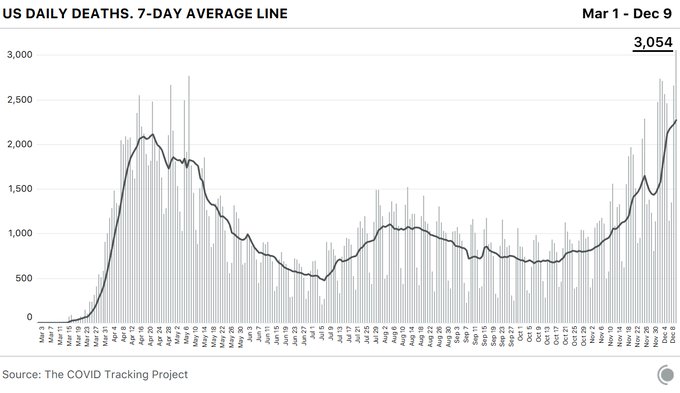
The coronavirus pandemic pushed the U.S. past another dire milestone Wednesday, the highest daily death toll to date, even while the mortality rate has decreased as health experts learn more about the disease.
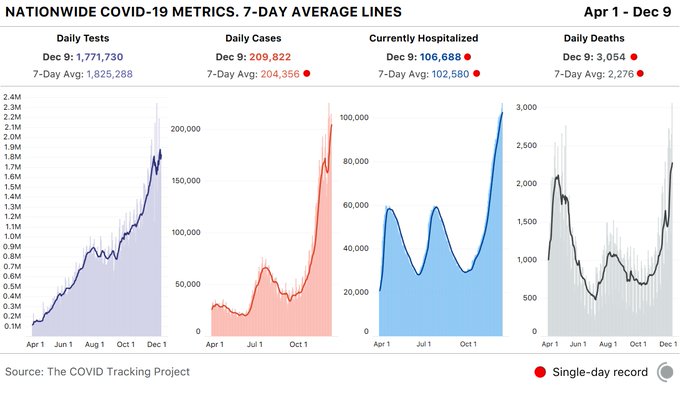
The Covid Tracking Project, which tracks state-level coronavirus data, reported 3,054 COVID-19 related deaths — a significant jump from the previous single-day record of 2,769 on May 7.
The spread of the disease has shattered another record with 106,688 COVID-19 patients in U.S. hospitals. And overall, states reported 1.8 million tests and 210,000 cases. According to the group, the spike represents more than a 10% increase in cases over the last 7 days.
Additionally, California nearly topped its single-day case record at 30,851. It is the second highest case count since December 6, the organization reported.
The staggering spike in fatalities and infections has overwhelmed hospitals and intensive care units across the nation, an increase attributed by many experts to people relaxing their precautions at Thanksgiving.
Many hospitals are temporarily or permanently reducing the size of their workforce as they grapple with depleted revenues and the thorny question of when they can return to normal operating capacity. Here’s a tracker to follow the latest updates.
Hospitals across the country, financially battered as they face the dual challenges of sick COVID-19 patients and a precipitous decline in patient volume, are struggling to balance quickly shifting staffing needs. While some face and others brace for intense demand, many have announced furloughs of specialists and others that work in elective surgeries that have been drastically scaled back.
Thousands of healthcare workers at hospitals big and small have been asked not to return to work, and it’s still unclear how soon non-essential services will return. While some governors announce plans to reopen businesses, others have extended stay-at-home orders.
Most recent data from the U.S Bureau of Labor doesn’t cover the second half of March or early April, but during the first half of March, the healthcare industry shed 43,000 jobs — reversing a decade of growth in the sector. According to BLS data, the industry added 49,000 jobs in March 2019.
“Even our emergency room has seen a significant drop in patients coming in,” Sue Philips, an ICU nurse at Palomar Pomerado Health in Northern San Diego, told Healthcare Dive.
Phillips is a spokesperson with National Nurses United, the country’s largest nurses union. Palomar Health, which runs three medical centers in northern San Diego County, recently instituted 21-day temporary layoffs of 221 employees.
On April 28, Palomar announced that most of those layoffs were becoming permanent. The system laid off 5% of its workforce, eliminating 317 positions. Fifty of those employees were clinical RNs, mostly in part-time positions, and the rest spread across the organization ranging from clerical staff to technicians.
Due to a 50% decrease in patient volumes, Palomar lost $10 million in revenue in March alone, according to a statement. In April the system said it stands to lose $20 million or more.
“I’m an ICU nurse, so my job is pretty much protected,” Phillips said. “But you didn’t think you were expendable until you became expendable, and that’s a hard pill for nurses and caregivers to swallow.”
Congress has attempted to financially support struggling hospitals through ongoing coronavirus relief legislation, approving some $175 billion thus far. But without knowing what will come next, hospitals are attempting to remain nimble while reining in one of their most costly expenses — paying employees.
The following information is based on publicly reported data, along with interviews with hospital representatives and union members.
It’s not an exhaustive list, but features nonprofit and for-profit hospital systems that reported revenue above $10 billion in 2019. It also takes a look at smaller, more regionally based systems that have announced similar cutbacks.
Click on link above to use the dropdown to find a company.
Healthcare job losses reached staggering levels amid stay-at-home orders and the widespread cancellation of elective procedures when the COVID-19 pandemic first hit this spring. Dentists and ambulatory services were particularly hard hit.
While the industry has since recovered many of the 1.3 million jobs lost this April, it’s still 527,000 short from February levels, and monthly gains have slowed since, according to the latest data from the Bureau of Labor Statistics.
At the same time, some of the major hospitals that issued furloughs or layoffs early in the pandemic are now further reducing the size of their workforce.
The stagnation will likely continue, as companies “don’t hire as many people, then lay some people off to also try and save money, because worse times may be ahead,” said Erica Groshen, former BLS commissioner and senior labor economics adviser at Cornell’s School of Industrial and Labor Relations.
One example is Dallas-based Baylor Scott & White, which laid off 3% of its workforce, or 1,200 employees in May. It’s now laying off a third of its corporate finance staff, though some impacted employees are being offered positions with a third-party vendor, the system said in a Monday statement.
Providence Health & Serviceslaid off 183 employees in mostly administrative roles as a result of transitioning work to a third-party vendor, while five employees were laid off “as a result of business need,” according to a WARN notice letter the system sent to an Oregon state agency Nov. 16. It previously issued an unknown number of furloughs across its 51-hospital system.
And Utah-based Intermountain Healthsaid it would cut 250 business-related jobs by offering 750 employees voluntary separation packages on Oct. 13.
The moves come even while hospitals are stretched to the brink from the highest surge of coronavirus cases the country has yet seen. In the past few weeks, many have halted elective procedures and paid steep rates for temporary nursing staff, further straining finances.
And other healthcare establishments, such as some doctor’s offices and medical labs, are still struggling to get reluctant patients back in.
A recent Labor Department survey covering the onset of the pandemic through September found among all healthcare businesses, 64% experienced a decrease in demand while only 13% experienced an increase in demand.
In November, healthcare businesses overall added 46,000 jobs in — fewer than the 58,000 jobs added in October; 53,000 in September; and 75,000 in August, according to BLS data.
Hospitals added about 4,000 jobs in November and are about 100,000 jobs short from February.
The financial challenges caused by the COVID-19 pandemic have forced hundreds of hospitals across the nation to furlough, lay off or reduce pay for workers, and others have had to scale back services or close.
Lower patient volumes, canceled elective procedures and higher expenses tied to the pandemic have created a cash crunch for hospitals. U.S. hospitals are estimated to lose more than $323 billion this year, according to a report from the American Hospital Association.
Hospitals are taking a number of steps to offset financial damage. Executives, clinicians and other staff are taking pay cuts, capital projects are being put on hold, and some employees are losing their jobs. More than 260 hospitals and health systems furloughed workers this year and dozens of others have implemented layoffs.
Below are 15 hospitals and health systems that announced layoffs since Sept. 1, many of which were attributed to financial strain caused by the pandemic.
1. Minneapolis-based Children’s Minnesota is laying off 150 employees, or about 3 percent of its workforce. Children’s Minnesota cited several reasons for the layoffs, including the financial hit from the COVID-19 pandemic. Affected employees will end their employment either Dec. 31 or March 31.
2. Dallas-based Baylor Scott & White Health announced in early December that it will lay off 102 employees in finance and accounting roles. The duties of the affected workers will be outsourced to a third-party vendor in India.
3. Eastern Niagara Hospitalin Lockport, N.Y., announced in early November that it plans to end intensive care unit services and move surgical services from the hospital to a surgery center. The changes will result in the loss of 80 jobs.
4. Detroit Medical Centerconfirmed in November that it laid off employees but declined to disclose the number of employees affected. Clinical staff, administrative assistants and employees at the management level were affected by the layoffs, sources told Crain’s Detroit Business.
5. Mercy Iowa City (Iowa) laid off 29 employees in November to address financial strain tied to the COVID-19 pandemic.
6. NorthBay Healthcare, a nonprofit health system based in Fairfield, Calif., announced Nov. 2 that it is laying off 31 of its 2,863 employees as part of its pandemic recovery plan.
7. Brattleboro Retreat, a psychiatric and addiction treatment hospital in Vermont, notified 85 employees in late October that they would be laid off within 60 days.
8. Oakland, Calif.-based Kaiser Permanente notified the state of Hawaii in November that it planned to lay off 45 employees within 60 days. “The COVID-19 public health crisis has placed unprecedented demands on the entire health care system, including Kaiser Permanente,” a Kaiser spokesperson said in an email to Pacific Business News. “Even before the pandemic, we had been transparent in sharing that Kaiser Permanente Hawaii faced ongoing financial challenges and that we were on a path to address our internal structure in a way that ensured we would be able to continue to deliver high-quality, affordable care and coverage to our members in Hawaii for years to come.” The health system said most of the positions eliminated were administrative or in non-patient facing areas.
9. Citing a need to offset financial losses, Minneapolis-based M Health Fairview said in October it plans to downsize its hospital and clinic operations. As a result of the changes, 900 employees, about 3 percent of its 34,000-person workforce, will be laid off.
10. Lake Charles (La.) Memorial Health System laid off 205 workers, or about 8 percent of its workforce, in October as a result of damage sustained from Hurricane Laura. The health system laid off employees at Moss Memorial Health Clinic and the Archer Institute, two facilities in Lake Charles that sustained damage from the hurricane.
11. Burlington, Mass.-based Wellforcelaid off 232 employees in September as a result of operating losses linked to the COVID-19 pandemic. The health system, comprising Tufts Medical Center, Lowell General Hospital and MelroseWakefield Healthcare, experienced a drastic drop in patient volume earlier this year due to the suspension of outpatient visits and elective surgeries.
12. Baptist Health Floydin New Albany, Ind., part of Louisville, Ky.-based Baptist Health, eliminated 36 positions in late September. The hospital said the cuts, which primarily affected administrative and nonclinical roles, are due to restructuring that is “necessary to meet financial challenges compounded by COVID-19.”
13. Cincinnati-based UC Health laid off about 100 employees in September. The job cuts affected both clinical and non-clinical staff. A spokesperson for the health system said no physicians were laid off.
14. Springfield, Ill.-based Memorial Health System laid off 143 employees in September, or about 1.5 percent of the five-hospital system’s workforce. The health system cited financial pressures tied to the pandemic as the reason for the layoffs.
15. Watertown, N.Y.-based Samaritan Health announced Sept. 8 that it laid off 51 employees and will make other cost-cutting moves to offset financial stress tied to the COVID-19 pandemic.
Letter of Intent offered to acquire Rhode Island-based Care New England Health System
StoneBridge Healthcare, LLC (StoneBridge), an innovative company formed to buy, save and turn around distressed hospitals in the cities and suburbs of America, today announced it has presented a Letter of Intent (LOI) to purchase Rhode Island-based Care New England Health System. StoneBridge would make a significant investment in order to financially stabilize Care New England to allow the health system to continue its mission to transform the future of health care for the communities it serves.
“Care New England Health System has provided outstanding care to its patients for many years, and StoneBridge Healthcare is committed to the continuation of this high standard of care in Rhode Island,” said Joshua Nemzoff, Chief Executive Officer, StoneBridge Healthcare. “We believe that StoneBridge Healthcare is in a strong position to help Care New England to continue delivering cutting-edge care to the communities it serves for years to come.”
StoneBridge has offered a transaction value of $550 million with a purchase price of $250 million and a $300 million investment in capital improvements over six years to further transform the health system. The offer that StoneBridge has submitted includes a provision that will fully fund the employee’s pension plan at closing – a plan that is currently underfunded by more than $125 million. Care New England hospitals include the following: Butler Hospital, Kent Hospital, Women & Infants Hospital of Rhode Island, Care New England Medical Group, the VNA of Care New England, The Providence Center, and a certified accountable care organization (ACO) Integra.
“As the cost of care has risen and the COVID-19 pandemic has placed a tremendous strain on health systems across the nation, StoneBridge Healthcare is ready to assist Care New England during these challenging times to continue delivering an outstanding continuum of care to the region,” Nemzoff added. “StoneBridge Healthcare has the expertise and financial resources needed to help lead Care New England to a promising future.”
The LOI is not binding, and a Definitive Agreement would be finalized in a short period of time once comprehensive due diligence is performed. StoneBridge is a privately-owned company capitalized through a multi-layered composite finance group that includes nationally known debt and equity sources.
Earlier this year, StoneBridge submitted an offer to acquire the Erlanger Heath System in Tennessee for a transaction value of $475 million. StoneBridge is actively pursuing discussions related to this transaction, which is a system of similar size to Care New England and has also been devastated by the impact of the COVID-19 pandemic.
About StoneBridge Healthcare StoneBridge Healthcare is an innovative company formed to buy, save and turn around deeply distressed hospitals in the cities and suburbs of America. StoneBridge is capitalized through a multi-layered composite finance group that includes nationally known debt and equity sources. The company features a nationally recognized team of experts in healthcare operations, finance, acquisitions and turnarounds.
Our decades of experience, our financial investment and our commitment to expand primary care into the urban areas we serve make our company the only one of its kind. StoneBridge Healthcare plans to purchase and turn around acute care hospitals that are in significant economic distress and could otherwise be forced to close. StoneBridge will identify and buy hospitals that can be saved, and then work urgently to make sure these hospitals survive and succeed.
StoneBridge is committed to responding to the healthcare needs of the urban markets it operates in through an initiative that is known as “The Mission Project.” Using the hospitals it acquires as a base of operations, StoneBridge will bring much-needed services into the community. StoneBridge will listen to and work with local groups to understand the gaps in community care – and then put money and time into offering clinics or other life-changing help. The solutions may look different in each market, but the commitment will be consistent. The hospitals can provide the doctors, nurses, pharmacies, kitchens and vehicles to bring care and support to people where they live. For more information please visit: stonebridgehealthcare.com.