The entities agreed to maintain services, provide capital investments and protect competition in the healthcare market.
California Attorney General Rob Bonta announced a settlement agreement this week reached by The Regents of the University of California and UCSF Health regarding their $100 million purchase of Dignity Health’s two San Francisco hospitals, St. Mary’s Medical Center (SMMC) and Saint Francis Memorial Hospital (SFMH).
Dignity Health is a nonprofit public benefit corporation that owns and operates SFMH, a 259-licensed-bed general acute care hospital, and SMMC, a 240-licensed-bed general acute care hospital. Both hospitals serve a diverse community, including a large number of elderly, unhoused and publicly insured patients who may rely on Medi-Cal, Medicare or charity care to access essential health services.
Under the settlement agreement approved by the San Francisco Superior Court, The Regents and UCSF Health commit to maintain services for the unhoused and Medi-Cal and Medicare beneficiaries, provide $430 million in capital investments, protect competition in the healthcare market and safeguard the affordability of and access to services for residents of San Francisco.
WHAT’S THE IMPACT
The Regents and UCSF Health agreed to a number of conditions over the next 10 years, including operating and maintaining SFMH and SMMC as licensed general acute care hospitals with the same types and levels of services, and associated staffing. They also agreed to continue participating in Medi-Cal and Medicare.
Also agreed upon was providing an annual amount of charity care at SFMH equal to or greater than $6.5 million and at SMMC equal to or greater than $3.5 million, with an annual increase of 2.4% at both hospitals.
The two entities agreed to provide an annual amount of community benefit spending for community healthcare needs at SFMH equal to or greater than $1.6 million and at SMMC equal to or greater than $10.7 million, to increase yearly by 2.4% at both hospitals.
UCSF Health and The Regents also pledged to invest at least $430 million, including at least $80 million for electronic medical record systems and related technologies, and at least $350 million in deferred maintenance and physical infrastructure improvements at both hospitals.
In addition to those agreements, they also agreed to a number of conditions over a seven-year period meant to maintain competition in the healthcare market, in part by maintaining contracts with the City and County of San Francisco for services at SFMH and SMMC unless terminated for cause.
The Regents and UCSF Health agreed to not condition medical staff privileges or contracts on the employment, contracting, affiliation, or appointment status of a physician with UCSF Health or any affiliate; not impose any requirement on any member of the hospitals’ medical staff, as a condition of either their medical staff membership or privileges that restricts them from contracting with providers other than UC Health; and negotiate all payer contracts for the hospitals separately and independently from payer contracts for UCSF Health, and maintain an information firewall between the two negotiating teams.
Finally, the two entities agreed to require, for five years, a price growth cap that limits the maximum that the hospitals may charge a payer from year to year upon renegotiation of contracts.
THE LARGER TREND
Mergers and acquisitions are expected to rebound this year after M&A activity fell to its lowest level in 10 years globally in 2023, according to Reuters.
Deal making last year was weighed down by high interest rates, economic uncertainty and a regulatory scrutiny, with all but the last factor slowly abating for renewed confidence.
Health systems put an emphasis on strategy over scale in hospital transactions announced in the second quarter of 2024, according to a July 9 report from Kaufman Hall.
“As pressure intensifies to transform the current healthcare system to bring greater value to patients and communities, the impetus for M&A activity will rely less on seeking capital in traditional ways and instead move toward new, strategic partnership models,” Anu Singh, managing director and mergers & acquisitions practice leader with Kaufman Hall, said in a July 9 news release. “Many of these M&A transactions enable hospitals to sustain and enhance access to care, launch new services, or strengthen and stabilize systems, which allows for future growth.”
Five things to know:
1. There were 11 hospital transactions announced in the second quarter of 2024, below historic Q2 averages. There were 20 hospital transactions announced in the second quarter of 2023.
2. Despite fewer overall deals, total transacted revenue in the quarter remained near historic highs at $10.8 billion.
3. Three of the 11 announced transactions involved religiously affiliated acquirers. Two involved academic or university-affiliated acquirers. The other six involved not-for-profit health system acquirers.
4. For the first time since Kaufman Hall tracked this data, there were no for-profit health system acquirers in the quarter. Kaufman Hall said in the report that this continues a trend of low for-profit buy-side activity. In the first quarter of 2024, just one of the 20 announced transactions involved a for-profit acquirer.
5. The emphasis on strategy over scale “characterized the most significant transactions of Q2 2024 and built upon trends we have been commenting on in recent past reports,” Kaufman Hall said.
Those trends are:
Pursuit of intellectual capital and new or complementary capabilities through a strategic partnership, often involving an innovative partnership model.
Focus of large regional or national systems on market reorganization and strategic realignment of their system portfolios.
The development of networks involving academic health systems and community hospital partners to sustain and enhance access to care.
A health system CEO recently reached out to me with a specific complaint that’s become a hot-button issue for an increasing number of systems:
“Medicare Advantage (MA) is no longer a good payer for us. When you factor in all the pre-auths and denials, we’re now getting four points less yield from our MA patients than from our traditional Medicare patients.
But our market is swinging hard toward MA, and I know the program’s not going anywhere…so how can we rethink our MA business model to make it more profitable?
After more than a decade of rapid growth, MA plans are now running into headwinds that are reducing their margins and creating an even more contentious negotiating environment with providers. However, these heightened competitive pressures could also be seen as an opportunity for provider organizations.
Rather than treating all of their MA payers as a monolith, a health system or other larger provider organization should be reassessing its MA book of business with the goal of identifying priority MA payers with which to pursue deeper, mutually beneficial partnerships.
The first step here is usually for a system to undergo a holistic tiering or ranking exercise for all of their MA payers according to factors like market share, contribution margin, value-based incentives, overall relationship dynamic, and projected market growth.
This exercise will identify not only which MA payers may not be high-priority, long-term partners, but also which MA payers are suitable for developing deeper relationships with (e.g., simplifying administrative burden, better rewards for value-based care, creating a joint insurance product).
If your system is facing challenges with MA and is interested in rethinking its MA portfolio strategy, please don’t hesitate to reach out.
A number of hospitals and health systems are reducing their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations announced this year.
June
West Monroe, La.-based Glenwood Regional Medical Center, part of Dallas-based Steward Health Care, laid off 23 employees. Affected roles included leadership, a spokesperson for the hospital said in a statement shared with Becker’s.
Cleveland-based University Hospitals is reducing its leadership structure by more than 10% as part of more than 300 layoffs. COO Paul Hinchey, MD, told Becker’s C-suite level leaders and vice presidents were included in the cuts.
Portland-based Oregon Health & Science Universitytold staff June 6 that it plans to lay off at least 500 employees, citing financial issues. The news follows the institution and Portland-based Legacy Health signing a binding, definitive agreement to come together as one health system under OHSU Health.
May
The All of Us Research Program, a collaboration of the University of Arizona in Tucson and Phoenix-based Banner Health, plans to lay off 45 workers due to reduced federal research funding, according to an Arizona WARN notice filed May 28. The program, launched in 2018, is part of HHS’ National Institutes of Health.
Burlington, Mass.-based Tufts Medicine will lay off 174 employees due to industry challenges, the health system confirmed in a May 21 statement shared with Becker’s. The layoffs, which have varying effective dates, will primarily affect administrative and non-direct patient care roles. Some leadership roles were affected, a spokesperson told Becker’s.
Doral, Fla.-based Sanitas Medical Centerlaid off 56 employees between May 17 and May 20. Some of the affected roles included nine care coordinators, one care educator, and two case managers, according to a May 20 WARN notice accessed by Becker’s.
Select Specialty Hospital in Longview, Texas, will close on or about June 30, affecting 94 employees, Becker’s has confirmed. The hospital, operated by Mechanicsburg, Pa.-based Select Medical, is a 32-bed, critical illness recovery facility.
White Rock Medical Center in Dallaslaid off nearly 35% of its staff. The hospital temporarily stopped taking patients transported by emergency medical services due to the layoffs, The Dallas Morning News reported. It has since resumed accepting those patients.
Oakland-based Kaiser Foundation Hospitals is laying off 76 workers in California. The layoffs primarily affect employees in IT and marketing, according to regulatory documents filed with the state May 1.
April
Pittsburgh-based UPMC will lay off approximately 1,000 employees. The layoffs, which represent more than 1% of the health system’s 100,000 workforce will primarily affect nonclinical, administrative and non-member-facing employees.
Union Springs, Ala.-based Bullock County Hospitallaid off 95 employees beginning April 9, according to regulatory documents filed with the state. The layoffs occurred as Bullock seeks to become a rural emergency hospital and is ending psychiatric services as part of the shift, AL.com reported April 25.
Jackson Health Systemreduced compensation programs for senior leaders; laid off fewer than 25 people, including one hospital CEO; and froze many vacant positions, especially in support and nonclinical areas, a spokesperson for the Miami-based organization confirmed to Becker’s. President and CEO Carlos Migoya shared these efforts in a message to staff, citing financial challenges.
Coos Bay, Ore.-based Bay Area Hospital plans to conduct layoffs as it outsources its revenue cycle management operations, a spokesperson for the hospital confirmed to Becker’s. The transition will affect 27 positions.
Manchester, N.H.-based Catholic Medical Centerplans to cut 142 positions, including 54 layoffs. An April 18 letter to employees from CMC president and CEO Alex Walker, obtained by Becker’s, said cuts would occur through the 54 staff eliminations, open position cuts, reduced hours, planned departures, and resource redeployment in satellite locations for CMC.
Marshfield (Wis.) Clinic Health System will lay off furloughed staff, effective in early May. The health system furloughed about 3% of its workforce in January, affecting positions mostly in non-patient-seeing departments, including leadership roles.
Norwalk, Ohio-based Fisher-Titus Medical Centerlaid off some workers in nonclinical roles and reduced hours for others. Seven employees, about 0.5% of the health system’s workforce, were laid off April 1. Work hours were reduced for another 10 positions, a hospital spokesperson told Becker’s.
March
Robbinsdale, Minn.-based North Memorial Health is laying off 103 employees in clinical and nonclinical roles, citing financial challenges. The layoffs affect several services across the two-hospital system.
AHMC’s San Gabriel (Calif.) Valley Medical Center is laying off 62 workers, according to regulatory documents filed with the state March 13. The layoffs take effect May 13.
Miami-based North Shore Medical Center, part of Steward Health Care, started conducting layoffs as part of cuts to some of its programs amid the Dallas-based health system’s continued financial struggles. Around 152 workers represented by 1199SEIU were laid off, a union spokesperson confirmed. However that number could be higher as their members do not represent every employee at NSMC, the spokesperson said.
Oakland, Calif.-based Kaiser Foundation Hospitals is laying off more than 70 employees. The layoffs primarily affect those in IT roles.
February
Lion Star, the group that operates Nacogdoches (Texas) Memorial Hospital, is closing four of its clinics on March 22, which will result in fewer than 50 layoffs, a Lion Star spokesperson confirmed to Becker’s. No additional layoffs are planned.
Little Rock-based Arkansas Heart Hospital has laid off fewer than 50 employees since the beginning of 2024, citing low reimbursement rates. The layoffs affected lower-paying positions, Bruce Murphy, MD, CEO of the hospital, said, according to Arkansas Business.
Cincinnati-based Mercy Health will lay off some call center positions. The system attributed the move to its partnership with a third party to operate its enterprise contact center for primary care scheduling.
Ridgecrest (Calif.) Regional Hospital announced more layoffs to avoid closure. It is laying off 31 more employees, including seven licensed vocational nurses and four registered nurses, two months after it announced plans to lay off nearly 30 others and suspend its labor and delivery unit, Bakersfield.com reported Feb. 15.
Medford, Ore.-based Asante health system laid off about 3% of its workforce. The layoffs primarily affected administrative and support roles and were necessary to offset “financial headwinds” over the past several years, according to a report from NBC affiliate KOBI-TV, which is based on an internal memo sent to staff Feb. 9.
Oakdale, Calif.-based Oak Valley Hospital District is scaling back services and laying off workers to improve its finances. The hospital said in a Feb. 2 statement shared with Becker’s that it will close its five-bed intensive care unit, discontinue its family support network department and lay off 28 employees, including those in senior management and supervisor positions.
Chicago-based Rush University System for Healthlaid off an undisclosed number of workers in administrative and leadership positions, citing “financial headwinds affecting healthcare providers nationwide.” No additional information was provided about the layoffs, including the number of affected employees.
University of Chicago Medical Center laid off about 180 employees, or less than 2% of its roughly 13,000-person workforce. The majority of affected positions are not direct patient facing, the organization said in a statement shared with Becker’s.
Fountain Valley, Calif.-based MemorialCarelaid off 72 workers due to restructuring efforts at its Long Beach (Calif.) Medical Center and Long Beach, Calif.-based Miller Children’s and Women’s Hospital. The layoffs include 13 positions at Long Beach Medical Center’s outpatient retail pharmacy, which is closing Feb. 2, a spokesperson for MemorialCare said in a statement shared with Becker’s.
January
George Washington University Hospital in Washington, D.C., part of King of Prussia, Pa.-based Universal Health Services, is laying off “less than 3%” of its employees. The move is attributed to restructuring efforts.
Amarillo-based Northwest Texas Healthcare System, also part of Universal Health Services, announced plans to lay off a “limited number of positions.” The move is attributed to restructuring efforts.
Lehigh Valley Health Network is cutting its chiropractic services and laying off 10 chiropractors. The layoffs are effective April 12 and due to restructuring. The Allentown, Pa.-based health system has 10 chiropractic locations, according to its website.
Central Maine Healthcare is laying off 45 employees as part of management reorganization. The Lewiston-based system, which also ended urgent care services at its Maine Urgent Care on Sabattus Street in Lewiston on Jan. 12, has 3,100 employees total.
University of Vermont Health Network, based in Burlington, is cutting 130 open positions. The move is part of the health system’s efforts to reduce expenses by $20 million.
Med-Trans, a medical transport provider based in Lewisville, Texas,closed its UF Health ShandsCair base serving Gainesville, Fla.-based UF Health Shands Hospital on Jan. 10 due to decreased transportation demands. The move also resulted in layoffs, a spokesperson for UF Health, the hospital’s parent company, told Becker’s in a statement.
RWJBarnabas Health, based in West Orange, N.J., is laying off 79 employees, according to documents filed with the state on Jan. 8. The layoffs are effective March 31 and April 5. A spokesperson for the health system told Becker’s that 74 of the positions were “time-limited information technology training job functions.” The other layoffs were due to closure of an urgent care center.
Risant Health, a nonprofit formed under Oakland, Calif.-based Kaiser Permanente, has signed a definitive agreement to acquire Greensboro, N.C.-based Cone Health.
The news comes less than three months after Risant acquired its first health system, Danville, Pa.-based Geisinger Health. If the transaction closes, Cone Health will operate independently as a regional and community-based health system under Risant, which supports organizations with technology and services to improve outcomes and lower care costs in diverse business models.“Cone Health’s impressive work for decades in moving value-based care forward aligns so well with Risant Health’s vision for the future of healthcare. Their longstanding success and deep commitment to providing high-quality care to North Carolina communities make them an ideal fit to become a part of Risant Health,” CEO, Jaewon Ryu, MD, said in a June 21 news release. “We will work together to share our industry-leading expertise and innovation to expand access to value-based care to more people in the communities we serve.”
Cone Health includes four acute-care hospitals, a behavioral health facility, three ambulatory surgery centers, eight urgent care centers and more than 120 physician practices, according to its website. It has more than 13,000 employees and over 700 physicians, along with 1,800 partner physicians. “As part of Risant Health, Cone Health will build upon its long track record of success making evidence-based health care more accessible and affordable for more people. The people across the Triad will be among the first to benefit,” Cone Health President and CEO Mary Jo Cagle, MD, said.
Cone Health will maintain its brand, name and mission, and maintain its own board, CEO and leadership team. It will continue to work with health plans, provider organizations and independent physicians. Dr. Cagle said she does not anticipate changes in the types of care Cone Health provides as a result of becoming part of Risant. The proposed transaction is subject to regulatory approvals and closing conditions.
Here are 48 health systems with strong operational metrics and solid financial positions, according to reports from credit rating agencies Fitch Ratings and Moody’s Investors Service released in 2024.
AdventHealth has an “AA” rating and stable outlook with Fitch. The rating is based on the Altamonte Springs, Fla.-based system’s competitive market position—especially in its core Florida markets—and its financial profile, Fitch said.
Advocate Health members Advocate Aurora Health and Atrium Health have “Aa3” ratings and positive outlooks with Moody’s. The ratings are supported by the Charlotte, N.C.-based system’s significant scale, strong market share across several major metro areas, and good financial performance and liquidity, Moody’s said.
Ann & Robert H. Lurie Children’s Hospital of Chicago has an “AA” rating and stable outlook with Fitch. The rating is supported by the system’s strong balance sheet with low leverage ratios derived from modest debt, Fitch said.
Avera Health has an “AA-” rating and a stable outlook with Fitch. The rating reflects the Sioux Falls, S.D.-based system’s strong operating risk and financial profile assessments, and significant size and scale, Fitch said.
Beacon Health System has an “AA-” rating and stable outlook with Fitch. Fitch said the rating reflects the strength of the South Bend, Ind.-based system’s balance sheet.
Carle Health has an “AA-” rating and stable outlook with Fitch. The rating reflects the Urbana, Ill.-based system’s distinctly leading market position over a broad service area and Fitch’s expectation that the system will sustain its strong capital-related ratios in the context of the system’s midrange revenue defensibility and strong operating risk profile assessments.
Carilion Clinic has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Roanoke, Va.-based system’s scale, regional significance as a tertiary referral system with broad geographic capture, and a highly integrated physician base with a well-defined culture, Moody’s said.
Cedars-Sinai Health System has an “AA-” rating and a stable outlook with Fitch. The rating reflects the Los Angeles-based system’s consistent historical profitability and its strong liquidity metrics, historically supported by significant philanthropy, Fitch said.
Children’s Health has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Dallas-based system’s continued strong performance from a focus on high margin and tertiary services, as well as a distinctly leading market share, Moody’s said.
Children’s Hospital Medical Center of Akron (Ohio) has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the system’s large primary care physician network, long-term collaborations with regional hospitals, and leading market position as its market’s only dedicated pediatric provider, Moody’s said.
Children’s Hospital of Orange County has an “AA-” rating and a stable outlook with Fitch. The rating reflects the Orange, Calif.-based system’s position as the leading provider for pediatric acute care services in Orange County, a position solidified through its adult hospital and regional partnerships, ambulatory presence, and pediatric trauma status, Fitch said.
Children’s Minnesota has an “AA” rating and stable outlook with Fitch. The rating reflects the Minneapolis-based system’s strong balance sheet, robust liquidity position, and dominant pediatric market position, Fitch said.
Cincinnati Children’s Hospital Medical Center has an “Aa2” rating and stable outlook with Moody’s. The rating is supported by its national and international reputation in clinical services and research, Moody’s said.
Cleveland Clinic has an “Aa2” rating and stable outlook with Moody’s. The rating reflects the system’s strength as an international brand in highly complex clinical care and research and centralized governance model, the ratings agency said.
Cook Children’s Medical Center has an “Aa2” rating and stable outlook with Moody’s. The ratings agency said the Fort Worth, Texas-based system will benefit from revenue diversification through its sizable health plan, large physician group, and an expanding North Texas footprint.
El Camino Health has an “AA” rating and a stable outlook with Fitch. The rating reflects the Mountain View, Calif.-based system’s strong operating profile assessment with a history of generating double-digit operating EBITDA margins anchored by a service area that features strong demographics as well as a healthy payer mix, Fitch said.
Froedtert ThedaCare Health has an “AA” rating and stable outlook with Fitch. The rating reflects the Milwaukee-based system’s solid market position, track record of strong utilization and operations, and strong financial profile, Fitch said.
Hoag Memorial Hospital Presbyterian has an “AA” rating and stable outlook with Fitch. The Newport Beach, Calif.-based system’s rating is supported by its strong operating risk assessment, leading market position in its immediate service area, and strong financial profile, Fitch said.
Inspira Health has an “AA-” rating and stable outlook with Fitch. The rating reflects Fitch’s expectation that the Mullica Hill, N.J.-based system will return to strong operating cash flows following the operating challenges of 2022 and 2023, as well as the successful integration of Inspira Medical Center of Mannington (formerly Salem Medical Center).
JPS Health Network has an “AA” rating and stable outlook with Fitch. The rating reflects the Fort Worth, Texas-based system’s sound historical and forecast operating margins, the ratings agency said.
Mass General Brigham has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Somerville, Mass.-based system’s strong reputation for clinical services and research at its namesake academic medical center flagships that drive excellent patient demand and help it maintain a strong market position, Moody’s said.
Mayo Clinic has an “Aa2” rating and stable outlook with Moody’s. The rating reflects the Rochester, Minn.-based system’s preeminent reputation for clinical care and research, including new discoveries and cutting-edge treatment, Moody’s said.
McLaren Health Care has an “AA-” rating and stable outlook with Fitch. The rating reflects the Grand Blanc, Mich.-based system’s leading market position over a broad service area covering much of Michigan, the ratings agency said.
Med Center Health has an “AA-” rating and stable outlook with Fitch. The rating reflects the Bowling Green, Ky.-based system’s strong operating risk assessment and leading market position in a primary service area with favorable population growth, Fitch said.
Memorial Healthcare System has an “Aa3” rating and stable outlook with Moody’s. Moody’s said the rating reflects that the Hollywood, Fla.-based system will continue to benefit from good strategic positioning of its large, diversified geographic footprint.
Memorial Hermann Health System has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Houston-based system’s leading and expanding market position and strong demand in a growing region, Moody’s said.
Methodist Health System has an “Aa3” rating and stable outlook with Moody’s. Moody’s said the rating reflects the Dallas-based system’s consistently strong operating performance, excellent liquidity, and very good market position.
Nationwide Children’s Hospital has an “Aa2” rating and stable outlook with Moody’s. The rating reflects the Columbus, Ohio-based system’s strong market position in pediatric services, growing statewide and national reputation, and continued expansion strategies.
Nicklaus Children’s Hospital has an “AA-” rating and stable outlook with Fitch. The rating is supported by the Miami-based system’s position as the “premier pediatric hospital in South Florida with a leading and growing market share,” Fitch said.
North Mississippi Health Services has an “AA” rating and stable outlook with Fitch. The rating reflects the Tupelo-based system’s strong cash position and strong market position with a leading market share in its primary services area, Fitch said.
Novant Health has an “AA-” rating and stable outlook with Fitch. The ratings agency said the Winston-Salem, N.C.-based system’s recent acquisition of three South Carolina hospitals from Dallas-based Tenet Healthcare will be accretive to its operating performance as the hospitals are highly profited and located in areas with growing populations and good income levels.
Oregon Health & Science University has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Portland-based system’s top-class academic, research, and clinical capabilities, Moody’s said.
Orlando (Fla.) Health has an “AA-” rating and stable outlook with Fitch. The rating reflects the health system’s strong and consistent operating performance and a growing presence in a demographically favorable market, Fitch said.
Parkland Health has an “AA-” rating and stable outlook with Fitch. The rating reflects Fitch’s expectation that the Dallas-based system will remain the leading provider of public (safety net) services in the vast Dallas County service area, supported by its tax levy.
Presbyterian Healthcare Services has an “AA” rating and stable outlook with Fitch. The Albuquerque, N.M.-based system’s rating is driven by a strong financial profile combined with a leading market position with broad coverage in both acute care services and health plan operations, Fitch said.
Rush University System for Health has an “AA-” rating and stable outlook with Fitch. The rating reflects the Chicago-based system’s strong financial profile and an expectation that operating margins will rebound despite ongoing macro labor pressures, the rating agency said.
Saint Francis Healthcare System has an “AA” rating and stable outlook with Fitch. The rating reflects the Cape Girardeau, Mo.-based system’s strong financial profile, characterized by robust liquidity metrics, Fitch said.
Saint Luke’s Health System has an “Aa2” rating and stable outlook with Moody’s. The Kansas City, Mo.-based system’s rating was upgraded from “A1” after its merger with St. Louis-based BJC HealthCare was completed in January.
Salem (Ore.) Health has an “AA-” rating and stable outlook with Fitch. The rating reflects the system’s dominant marketing position in a stable service area with good population growth and demand for acute care services, Fitch said.
Seattle Children’s Hospital has an “AA” rating and a stable outlook with Fitch. The rating reflects the system’s strong market position as the only children’s hospital in Seattle and provider of pediatric care to an area that covers four states, Fitch said.
SSM Health has an “AA-” rating and stable outlook with Fitch. The St. Louis-based system’s rating is supported by a strong financial profile, multistate presence and scale with good revenue diversity, Fitch said.
St. Elizabeth Medical Center has an “AA” rating and stable outlook with Fitch. The rating reflects the Edgewood, Ky.-based system’s strong liquidity, leading market position, and strong financial management, Fitch said.
Stanford Health Care has an “Aa3” rating and positive outlook with Moody’s. The rating reflects the Palo Alto, Calif.-based system’s clinical prominence, patient demand, and its location in an affluent and well-insured market, Moody’s said.
UChicago Medicine has an “AA-” rating and stable outlook with Fitch. The rating reflects the system’s strong financial profile in the context of its broad and growing reach for high-acuity services, Fitch said.
University Health has an “AA+” rating and stable outlook with Fitch. The San Antonio-based system’s outlook is based on the Bexar County Hospital District’s significant tax margin, good cost management, and strong leverage position relative to its liquidity and outstanding debt.
University of Colorado Health has an “AA” rating and stable outlook with Fitch. The Aurora-based system’s rating reflects a strong financial profile benefiting from a track record of robust operating margins and the system’s growing share of a growth market anchored by its position as the only academic medical center in the state, Fitch said.
VCU Health has an “Aa3” rating and stable outlook with Moody’s. The rating reflects the Richmond, Va.-based system’s status as one of Virginia’s leading academic medical centers and essential role as its largest safety net provider, supporting excellent patient demand at high acuity levels, Moody’s said.
Willis-Knighton Medical Center has an “AA-” rating and positive outlook with Fitch. The outlook reflects the Shreveport, La.-based system’s improving operating performance relative to the past two fiscal years combined with Fitch’s expectation for continued improvement in 2024 and beyond.
Citing financial challenges, Cleveland-based University Hospitals is reducing its leadership structure by more than 10% as part of more than 300 layoffs.
Rising costs of supplies, labor and purchase services, and reduced Medicare reimbursement rates, have affected UH and various other systems, according to COO Paul Hinchey, MD.
“All of that’s creating significant downward pressure on our revenue,” Dr. Hinchey told Becker’s.
The news from UH follows a national trend of hospitals facing significant headwinds. Kaufman Hall found in early June that 40% of hospitals in the U.S. are still losing money.
At UH, revenue has increased nearly 9% year over year due to various changes, such as increased access for patients and implementing a new EHR system, according to UH.
“[However], in spite of our efforts and being successful in growth, that downward pressure on revenue and the increasing prices is pinching our margin,” said Dr. Hinchey.
Dr. Hinchey said the health system has been optimizing operations since the end of the pandemic.
“We took a look at our cost structure and recognized we needed to get our cost structure down,” he said. “We’ve done a couple initiatives that we put under the auspices of a Medicare break-even initiative to try to drive down our cost structure.”
Some actions already taken have included increasing efficiency, consolidating service lines and closing hospitals in Bedford and Richmond Heights, according to UH.
Most recently, the health system identified an opportunity to make cuts to leadership. Dr. Hinchey said C-suite level leaders and vice presidents were included in the cuts.
“These decisions are never easy,” Cliff Megerian, MD, CEO and Jane and Henry Meyer Chief Executive Officer Distinguished Chair, said in a news release. “The important thing is that we make these strategic moves now so we can continue to serve our community and fulfill our mission for decades to come. We are thankful for our hometown team that delivers lifesaving care to our neighbors, friends and relatives each and every day.”
Dr. Hinchey said UH began notifying employees of the layoffs on June 17. Affected workers will receive a severance package aligned with their roles and tenure.
Last week, 2 important economic reports were released that provide a retrospective and prospective assessment of the U.S. health economy:
The CBO National Health Expenditure Forecast to 2032:
“Health care spending growth is expected to outpace that of the gross domestic product (GDP) during the coming decade, resulting in a health share of GDP that reaches 19.7% by 2032 (up from 17.3% in 2022). National health expenditures are projected to have grown 7.5% in 2023, when the COVID-19 public health emergency ended. This reflects broad increases in the use of health care, which is associated with an estimated 93.1% of the population being insured that year… During 2027–32, personal health care price inflation and growth in the use of health care services and goods contribute to projected health spending that grows at a faster rate than the rest of the economy.”
The Congressional Budget Office forecast that from 2024 to 2032:
National Health Expenditures will increase 52.6%: $5.048 trillion (17.6% of GDP) to $7,705 trillion (19.7% of GDP) based on average annual growth of: +5.2% in 2024 increasing to +5.6% in 2032
NHE/Capita will increase 45.6%: from $15,054 in 2024 to $21,927 in 2032
Physician services spending will increase 51.2%: from $1006.5 trillion (19.9% of NHE) to $1522.1 trillion (19.7% of total NHE)
Hospital spending will increase 51.6%: from $1559.6 trillion (30.9% of total NHE) in 2024 to $2366.3 trillion (30.7% of total NHE) in 2032.
Prescription drug spending will increase 57.1%: from 463.6 billion (9.2% of total NHE) to 728.5 billion (9.4% of total NHE)
The net cost of insurance will increase 62.9%: from 328.2 billion (6.5% of total NHE) to 534.7 billion (6.9% of total NHE).
The U.S. Population will increase 4.9%: from 334.9 million in 2024 to 351.4 million in 2032.
The Bureau of Labor Statistics CPI Report for May 2024 and Last 12 Months (May 2023-May2024):
“The Consumer Price Index for All Urban Consumers (CPI-U) was unchanged in May on a seasonally adjusted basis, after rising 0.3% in April… Over the last 12 months, the all-items index increased 3.3% before seasonal adjustment. More than offsetting a decline in gasoline, the index for shelter rose in May, up 0.4% for the fourth consecutive month. The index for food increased 0.1% in May. … The index for all items less food and energy rose 0.2% in May, after rising 0.3 % the preceding month… The all-items index rose 3.3% for the 12 months ending May, a smaller increase than the 3.4% increase for the 12 months ending April. The all items less food and energy index rose 3.4 % over the last 12 months. The energy index increased 3.7%for the 12 months ending May. The food index increased 2.1%over the last year.
Medical care services, which represents 6.5% of the overall CPI, increased 3.1%–lower than the overall CPI. Key elements included in this category reflect wide variance: hospital and OTC prices exceeded the overall CPI while insurance, prescription drugs and physician services were lower.
Physicians’ services CPI (1.8% of total impact): LTM: +1.4%
Hospital services CPI (1.0% of total impact): LTM: +7.3%
Prescription drugs (.9% of total impact) LTM +2.4%
Over the Counter Products (.4% of total impact) LTM 5.9%
Health insurance (.6% of total) LTM -7.7%
Other categories of greater impact on the overall CPI than medical services are Shelter (36.1%), Commodities (18.6%), Food (13.4%), Energy (7.0%) and Transportation (6.5%).
Three key takeaways from these reports:
The health economy is big and getting bigger. But it’s less obvious to consumers in the prices they experience than to employers, state and federal government who fund the majority of its spending. Notably, OTC products are an exception: they’re a direct OOP expense for most consumers. To consumers, especially renters and young adults hoping to purchase homes, the escalating costs of housing have considerably more impact than health prices today but directly impact on their ability to afford coverage and services. Per Redfin, mortgage rates will hover at 6-7% through next year and rents will increase 10% or more.
Proportionate to National Health Expenditure growth, spending for hospitals and physician services will remain at current levels while spending for prescription drugs and health insurance will increase. That’s certain to increase attention to price controls and heighten tension between insurers and providers.
There’s scant evidence the value agenda aka value-based purchases, alternative payment models et al has lowered spending nor considered significant in forecasts.
The health economy is expanding above the overall rates of population growth, overall inflation and the U.S. economy. GDP. Its long-term sustainability is in question unless monetary policies enable other industries to grow proportionately and/or taxpayers agree to pay more for its services. These data confirm its unit costs and prices are problematic.
As Campaign 2024 heats up with the economy as its key issue, promises to contain health spending, impose price controls, limit consolidation and increase competition will be prominent.
Public sector actions
will likely feature state initiatives to lower cost and spend taxpayer money more effectively.
Private sector actions
will center on employer and insurer initiatives to increase out of pocket payments for enrollees and reduce their choices of providers.
Thus, these reports paint a cautionary picture for the health economy going forward. Each sector will feel cost-containment pressure and each will claim it is responding appropriately. Some actually will.
PS: The issue of tax exemptions for not-for-profit hospitals reared itself again last week.
The Committee for a Responsible Federal Budget—a conservative leaning think tank—issued a report arguing the exemption needs to be ended or cut. In response,
the American Hospital Association issued a testy reply claiming the report’s math misleading and motivation ill-conceived.
This issue is not going away: it requires objective analysis, fresh thinking and new voices. For a recap, see the Hospital Section below.
In recent years, the Medicare Advantage (MA) program enjoyed both rapid membership growth and positive attention from healthcare organizations and advocates. As of the beginning of 2024, 33.4 million Americans were enrolled in MA, up 7% from 2023.
More than half of all Medicare-eligible individuals are now enrolled in MA.
Interest and growth in MA has been buoyed by a number of factors: a growing eligible population as Baby Boomers continue to age into Medicare eligibility; affordable benefit packages with low or zero monthly premiums; regulatory changes providing for more flexibility in plan and member design; consumer-centric programs and care models tailored to the needs of beneficiaries; increased marketing and sales efforts through direct mailings, telemarketing, and online advertising.
The program has also delivered meaningful value to members, who are more likely than traditional Medicare beneficiaries to have an annual income less than $40,000. In addition, the average monthly premium for Medicare beneficiaries enrolled in an MA plan has dropped by almost one-third in the last four years, reaching $18 per month in 2023.
Ideally, success in MA can take the form of a virtuous cycle: an improved margin on MA for a plan enables reinvestment in related products to grow membership and better manage health outcomes, which leads to further reinvestment (Figure 1). Sustained success is contingent on meaningful collaboration between payers and providers.
FIGURE 1: The Virtuous Cycle of MA Success
MA Hits Headwinds
However, after several high-growth years, payers and providers are currently confronting multiple MA-related challenges. Many providers have recently posted losses as their contractual yields decrease and authorizations for care have become more restrictive. The bar for risk adjustment and Star Ratings is also rising. Only 6% of plans received a 5-star rating from the Center for Medicare & Medicaid Services (CMS) for 2024, down from 22% in 2023. CMS also recently confirmed plans for rate cuts in 2025, with critics arguing that benefits for beneficiaries may become more limited. Providers are also reeling from related bureaucratic headaches.
Current MA members also have expressed concerns with the program’s trajectory. While roughly two-thirds of MA and traditional Medicare beneficiaries recently surveyed by the Commonwealth Fund said their coverage has met their expectations, MA members were more likely to report delays in care while awaiting prior approval (22% vs. 13%) or difficulty affording care due to copayments or deductibles (12% vs. 7%).
Despite current challenges, many providers and health plans believe they need to continue to participate in and/or prioritize MA, given the program’s scale and overall benefits to their organizations and the communities they serve.
For instance, the success of MA risk contracts predicated on collaborating around delivering healthcare value suggests a possible path forward.
According to a JAMA study of more than 300,000 Medicare Advantage beneficiaries, members in value-based care MA arrangements with risk for both payers and providers had lower rates of inpatient admission, emergency department visits, and readmissions. In addition, CMS’s robust risk scoring model ensures that providers are paid fairly for the true cost of providing care to the populations they serve.
Percent of premium contracts, where payers delegate a share of the premium to providers to manage, are predictable, align payer and provider interests, easy to understand, and increasingly common.
In addition, the high cost of caring for Medicare enrollees makes the population health focus on VBC arrangements economical. Medicare members have the highest utilization of any insurance class, so intensive services like care management, disease management, and care coordination are more likely to have a positive return on investment.
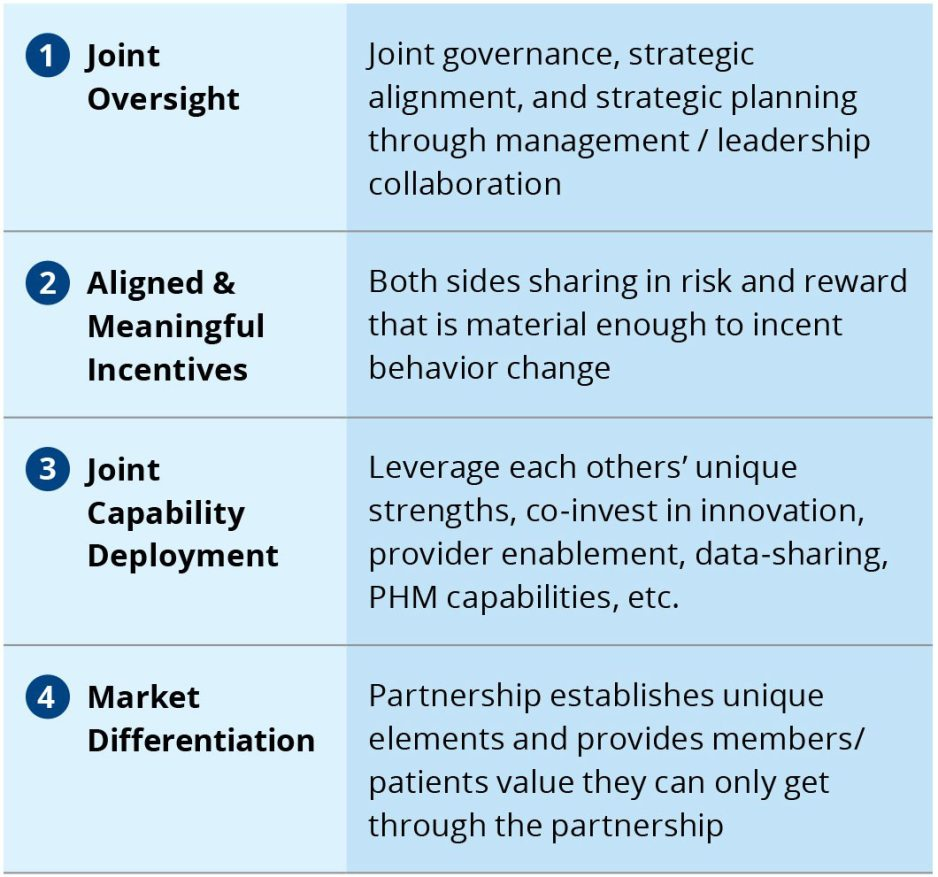
Successful VBC arrangements share several core tenets, grounded in the need for close collaboration between participating parties (Figure 2).
FIGURE 2: Core Tenets of Successful Payer-Provider Value-Based Care Models
However, VBC arrangements are not the only option. Value-centric collaborations can take on a wide range of forms, depending on the amount of risk providers are willing to assume and the partnerships’ risk-related capabilities. The full continuum of value-centric collaborations runs the gamut from shared savings contracts with no downside risk for providers to full vertical integration into a single organization (Figure 3).
FIGURE 3: Understanding the Continuum of Value-Based Care Arrangements
Looking Into the Crystal Ball: Three Future State Scenarios
As the MA market confronts new headwinds after years of growth and favorable attention, we anticipate three possible future state scenarios. These possibilities can be applied to both the outlook nationally, as well as the actions of payers and providers within specific markets.
Scenario 1: A renewal of growth
In this scenario, better sense prevails, and plans and providers collaborate to address the core issues facing the program. A pause/adjustment in the market is followed by a period of renewed growth. From a national standpoint, this scenario is contingent on neutral to favorable regulatory treatment.
Scenario 2: Uneasy stabilization
In this scenario, contention is partially resolved through some degree of collaboration between payers and providers. This scenario is also dependent on neutral to favorable regulatory treatment.
Scenario 3: Implosion
In this scenario, high levels of contention continue, and more providers go out of network. Middle-income Medicare members opt out of MA and go back to traditional Medicare when feasible. This scenario accounts for heightened regulatory pressure on risk adjustment and utilization management practices, which further pressures margins.
Conclusion
Despite MA’s recent, publicly documented challenges, the program now accounts for more than half of all Medicare beneficiaries—a patient population that every healthcare organization must engage in some form or fashion.
As providers and payers decide how to approach the program—and each other—amid uncertainty and contention, the path forward can appear unclear. However, healthcare leaders seeking to emerge from the current environment of MA contention have an opportunity to shape the future of MA and will play a major role determining which of the three scenarios outlined in this article comes to fruition.
Ultimately, organizations must be able to develop a business model that both delivers quality care and manageable per capita costs—and critically, find ways to work through today’s pressing concerns with other MA stakeholders and partners.
On average, supply costs comprise about 10.5% of a hospital’s budget, the American Hospital Association said its May 2 “Cost of Caring” report, citing data from Strata Decision Technology.
Having adequate and up-to-date medical supplies, devices and equipment are necessary for hospitals to deliver high quality care to patients, AHA said, but “most of these items are expensive to acquire and maintain and rely on increasingly volatile global supply chains.”
Here is a look at how supply costs have grown year over year at 20 hospitals for the quarter ended March 31: