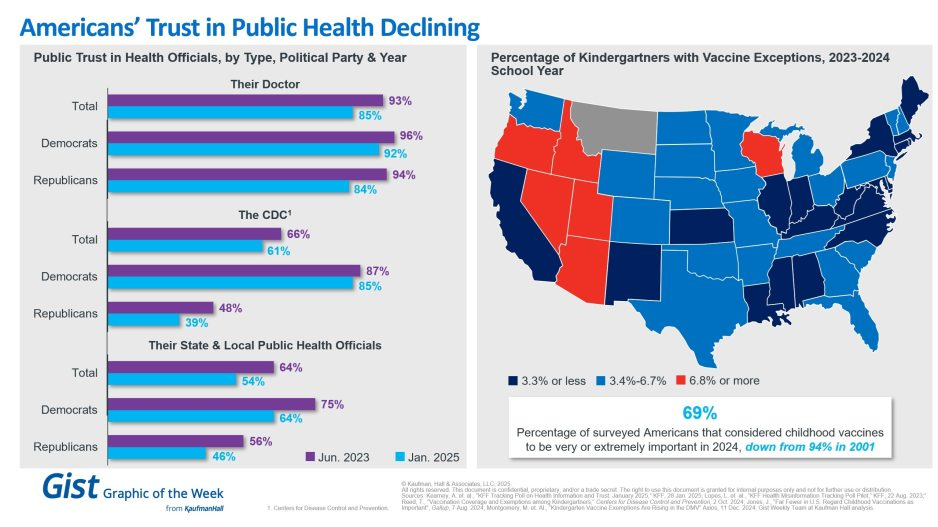
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
The murder of UnitedHealthcare CEO Brian Thompson in December 2024 represented a horrific and indefensible act of violence. As a physician and healthcare leader, I initially declined to comment on the killing. I felt that speculating about the shooter’s intent would only sensationalize a terrible act.
Regardless of the circumstances, vigilante violence has no place in a free and just society.
Now, more than a month later, I feel compelled to address one aspect of the story that has been widely misunderstood: the public’s reaction to the news of Thompson’s murder. Specifically, why tens of thousands of individuals “liked” and “laughed” at a post on Facebook announcing the CEO’s death.
What causes someone to ‘like’ murder?
News analysts have attributed the social media response to America’s “simmering anger” and “frustration” with a broken healthcare system, pointing to rising medical costs, insurance red tape and time-consuming prior authorization requirements as justifications.
These are all, indeed, problems and may explain some of public’s reaction. Yet these descriptions grossly understate the lived reality for most of those affected. When I speak with individuals who have lost a child, parent or spouse because of what they perceive as an unresponsive and uncaring system, their pain is raw, intense. What they feel isn’t frustration—it’s agony.
By framing healthcare’s failures in terms of statistical measures and policy snafus, we reduce a deeply personal crisis to an intellectual exercise. And it’s this very detached, cognitive approach that has allowed our nation to disregard the emotional devastation endured by millions of patients and their families.
When journalists, healthcare leaders and policymakers cite eye-popping statistics on healthcare expenditures, highlight exorbitant insurer profits or deride the bloated salaries of executives, they leave out a vital part of the story. They omit the unbearable human suffering behind the numbers. And I fear that until we approach healthcare as a moral crisis—not merely an economic or political puzzle to solve—our nation will never act with the urgency required to relieve people’s profound pain.
A pain beyond reason
In Dante’s Inferno, hell is a place where suffering is eternal and the cries of the damned go unheard. For countless Americans who feel trapped in our healthcare system, that metaphor rings true. Their anguish and pleas for mercy are met with silence.
It is this sense of abandonment and powerlessness, not mere frustration, that fuels both a desperate rage and an anger at a system and its leaders who appear not to care. The response isn’t one of glee—it’s a visceral reaction born of pain and unrelenting remorse.
As a clinician, I’ve seen life-destroying pain in my patients—and even within my own family. When my cousin Alan died in his twenties from a then-incurable cancer, my aunt and uncle were powerless to save him. Their grief was profound, unrelenting and eternal.They never recovered from the loss. But Alan’s death, heartbreaking as it was, stemmed from the limits of science at the time.
What millions of Americans endure today is different. Their loved ones die not because cures don’t exist but because the healthcare system treats them like a number. Bureaucratic inefficiencies, profit-driven delays and systemic indifference produce avoidable tragedies.
To appreciate this depth of pain, imagine standing behind a chain-link fence, watching someone you love being tortured. You scream and plead for help, but no one listens. That is what healthcare feels like for too many Americans. And until all of us acknowledge and feel their pain, little will improve.
Curing America’s indifference
When we focus solely on cold numbers—the millions who’ve lost Medicaid coverage, the hundreds of thousands of avoidable deaths each year, or the life-expectancy gap between the U.S. and other nations—we strip healthcare of its humanity.
But once we stop framing these failures as bureaucratic inefficiencies or frustrations and, instead, focus on the devastation of having to watch a loved one suffer and die needlessly, we are forced to confront a moral imperative. Either we must act with urgency and resolve the problem or admit we simply don’t care.
In the halls of Congress, lawmakers continue to weigh modest reforms to prior authorization requirements and Medicaid spending—baby steps that won’t fix a system in crisis. The truth is that without bold, transformative action, healthcare will remain unaffordable and inaccessible for millions of families whose anguish will grow.
Here are three examples of the scale of transformation required:
Reverse the obesity epidemic with a two-part strategy. Congress will need to tax ultra-processed, sugary foods that drive hundreds of billions of dollars in healthcare costs each year. In parallel, lawmakers should cap the manufacturer-set price of weight-loss medications like Ozempic and Wegovy to be no higher than in peer nations.
Change clinician payments from volume to value. Current fee-for-service payment systems incentivize unnecessary tests, treatments and procedures rather than better health outcomes. Transitioning to pay-for-value would reward healthcare providers, and specifically primary care physicians, who successfully prevent chronic diseases, better manage existing conditions, and reduce complications such as heart attacks, strokes and kidney failure.
Empower patients and save lives with generative AI. Tools like ChatGPT can help reduce the staggering 400,000 annual deaths from misdiagnoses and 250,000 more from preventable medical errors. By integrating AI into healthcare, we can enable at-home care, continuous disease monitoring and personalized treatment, making medical care safer, more accessible and more efficient.
If elected officials, payers and regulators fail to act, they will have chosen to perpetuate the unbearable pain and suffering patients and families endure daily. They need to hear the cries of people. The time for transformative action is now.
I never met Brian Thompson. His senseless death is first and foremost a human tragedy.
Second, it’s a business story that continues to unfold. Speculation about the shooter’s motive and whereabouts runs rampant.
But media attention has seized on a larger theme: the business of health insurance and its role in U.S. healthcare.
Headlines like these illustrate the storyline that has evolved in response to the killing: health insurance is part of a complicated industry where business practices are often geared to corporate profit.
Some on Social Media See Suspect in C.E.O. Killing as a Folk Hero New York Times
In this coverage and social media postings, health insurer denials are the focal point: journalists and commentators have seized on the use of Artificial intelligence-based tools used by plans like United, Cigna, Aetna and most others to approve/deny claims and Thompson’s role as CEO of UHG’s profitable insurance division.
The bullet-casing etchings “Deny. Defend. Depose” is now a T-shirt whistle to convey a wearer’s contempt for corporate insurers and the profit-seeking apparatus in U.S. healthcare.
Laid bare in the coverage of Brian’s death is this core belief: the majority of Americans think the U.S. health system is big business and fundamentally flawed.
As noted in last week’s Gallup Poll, and in previous polling by Pew, Harris, Kaiser Family Foundation and Keckley, only one in three Americans believe the health system performs well. Accessibility, costs, price transparency and affordability are dominant complaints. They believe the majority of health insurers, hospitals and prescription drug companies put their financial interests above the public’s health and wellbeing. They accept that the health system is complex and expensive but feel helpless to fix it.
This belief is widely held: its pervasiveness and intensity lend to misinformation and disinformation about the system and its business practices.
Data about underlying costs and their relationship to prices are opaque and hard to get. Clinical innovation and quality of care are understood in the abstract: self-funded campaigns touting Top 100 recognition, Net Promoter Scores are easier. The business of healthcare financing and delivery is not taught: personal experiences with insurers, hospitals, physicians and drugs are the basis for assessing the system’s effectiveness…and those experiences vary widely based on individual/household income, education, ethnicity and health status.
The majority accept that operators in every sector of healthcare apply business practices intended to optimize their organization’s finances. Best practices for every insurer, hospital, drug/device manufacturer and medical practice include processes and procedures to maximize revenues, minimize costs and secure capital for growth/innovation.
But in healthcare, the notion of profit remains problematic: how much is too much? and how an organization compensates its leaders for results beyond short-term revenue/margin improvement are questions of growing concern to a large and growing majority of consumers.
In every sector, key functions like these are especially prone to misinformation, disinformation and public criticism:
Among insurers, provider credentialing, coverage allowance and denial management, complaint management and member services, premium pricing and out-of-pocket risks for enrollees, provider reimbursement, prior authorization, provider directory accuracy, the use of AI in plan administration and others.
Among hospitals, price setting, employed physician compensation, 340B compliance, price and cost transparency, revenue-cycle management and patient debt collection, workforce performance composition, evaluation and compensation, integration of AI in clinical and administrative decision-making, participation in gainsharing/alternative payment programs, clinical portfolio and others.
And across every sector, executive compensation and CEO pay, Board effectiveness, and long-term strategies that balance shareholder interests with broader concern for the greater good.
The bottom line:
The public is paying attention to business practices in healthcare. The death of Brian Thompson opened the floodgate for criticism of health insurers and the U.S. healthcare industry overall. It cannot be ignored. The public thinks industry folks are shrewd operators and they’re inclined to conclude they’re screwed as a result.
The sports betting market has multiplied tenfold in three years and may have reached $7 billion in 2022. More than half of the nation can now legally gamble on sports. Fifty million Americans are expected to bet on the upcoming Super Bowl.
Five years ago, betting on live games was illegal in most of the United States. A Supreme Court ruling in 2018 removed the ban and transformed the industry. Now, 33 states and the District of Columbia allow wagers on games.
Addiction experts fear a coming national epidemic to rival the opioid crisis.
“Gambling is a very different addiction from drugs or alcohol,” said Lia Nower, a professor and director of the Center for Gambling Studies at Rutgers University. “If I’m drunk or high, at some point my family is going to figure it out. With gambling, I can be sitting with my kids, watching cartoons, and gambling away my house, my car, everything I own, on my mobile phone. How would you know?”
The Supreme Court ruling struck down a federal law that had banned most commercial sport wagering outside Las Vegas. The subsequent spread of legal gambling was stunningly swift.
Lobbyists pampered state lawmakers with parties and promises, predicting millions in new tax dollars. Much of the promised revenue hasn’t reached the states, according to a New York Times investigation.
But gambling dollars have reached the betting operators. The industry reaped $4.3 billion in revenue on $57 billion in wagers in 2021. In the first 11 months of 2022, Americans bet $83 billion on sports and delivered $6.6 billion to betting firms. That figure is 15 times what the sports gambling industry reaped in 2018.
“We have a movement toward expanding what was once considered a sin, what was once considered a vice, and embedding it at every level of American culture, down to kindergarten,” said Timothy Fong, a clinical professor of psychiatry at the Jane and Terry Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles.
“Sports gambling market. Ten years ago, those words didn’t exist,” Fong said. “What you have is this massive, exponential expansion of gambling into homes, faster than we can study or monitor it.”
A record 50 million Americans, one adult in five, will bet on Super Bowl LVII, according to an American Gaming Association survey. They will wager $16 billion, twice as much as last year.
Celebrity athletes shill for betting firms on television. Betting firms promote gambling on college campuses. Professional teams court “official mobile sports betting partners.”
“Pete Rose was banned from baseball and blocked from the Hall of Fame because he gambled,” said Nower, of Rutgers. “Now, we’ve got professional ballplayers who are partnering with gambling companies. Now, kids are seeing these things inextricably linked.”
Teams and league owners love sports betting because they “have found that engagement is off the charts among people who are placing bets on games,” said Daniel Barbarisi, author of “Dueling with Kings: High Stakes, Killer Sharks, and the Get-Rich Promise of Daily Fantasy Sports.”
People who bet on games “are not just tuning out if it’s a blowout,” Barbarisi said, because they bet on more than the final score. Fans can place wagers on the margin of victory, the combined point total from both teams and other metrics — such as whether Aaron Judge will hit a home run or Max Scherzer will ring up double-digit strikeouts.
Sports bettors are predominantly male, surveys show. They are mostly under 45. Some are wealthy, but a Rutgers study found that half of sports gamblers earn less than $50,000 a year. Some hail from a distinct subpopulation of Americans who get a thrill from risking money on the Next Big Thing.
“You can kind of draw a through line from the people who were involved in the poker boom in the early 2000s to the daily fantasy thing in the 2010s and then to the crypto thing,” Barbarisi said.
“I don’t know if you can say it’s a small group of guys anymore. It’s a big group of guys.”
Gambling is unquestionably addictive, and arguably immoral: Not for nothing did Las Vegas earn the Sin City sobriquet. Now that betting on sports is broadly legal, however, Americans are warming to the idea.
A poll by The Washington Post and University of Maryland found that 66 percent of Americans approved of legal sports betting in 2022, up from 55 percent in 2017, a year before the Supreme Court decision.
Nower suspects most Americans remain naive about gambling’s ills, much as society once cheerily embraced smoking and drinking. “We are where cigarettes were in the 1940s and alcohol was in the 1950s,” she said.
Most Americans ignored the opioid crisis, a staggering increase in overdose deaths in the 1990s and 2000s, until the government and news media processed the data and tendered a response.
With sports betting, “you have the exact same players you had with opioids,” Fong said. “You have government. You have industry. You have civilians, a lot of whom will benefit from this. And then you have a population who will develop an addiction, let’s say 1, 1.5 percent of the population.”
With legal sports gambling, “It’s a hidden addiction,” Fong said. “You can’t see it, you can’t smell it, you can’t taste it.”
Fong points to one of his patients, a man in his 20s who earns $160,000 a year and owes $40,000 in gambling debts.
“On face value, he can pay his rent, he’s not gonna die,” Fong said. “But he’s miserable. He’s just not happy.”
Over time, researchers say, sports-betting addiction will take a toll in rising rates of bankruptcy, domestic violence, depression, anxiety and suicide.
The federal government takes a keen interest in regulating alcohol, tobacco and drugs. In sports gambling, by contrast, “there is no federal presence at all,” Nower said. “And that is the biggest problem.”
Oversight of the booming sports-betting industry has been mostly left to states.
States that allow legal sports gambling “are not disinterested parties,” the Times wrote in its 2022 investigation. “They collect taxes on gambling, and the more people bet, the more governments get. One result is that states have, in many ways, given gambling companies free rein.”
New Jersey, the state at the heart of the 2018 Supreme Court ruling, offers a rare exception, Nower said.
Gambling regulators in New Jersey studied “the relationship between gambling and problem gambling” before they allowed legal gambling on sports, Nower said. She knows of no other state that took that step.
New Jersey uses gambling data to identify “people who may be exhibiting problem symptoms,” Nower said: Shuffling several payment methods, overdrawing their cards, doubling down on bets, gambling more frequently.
Most other states “are just legalizing this stuff without any idea of the effects,” she said.
The sports betting landscape will remain untamed, researchers say, until governments recognize gambling as a matter of public health.
“I do think there are watershed moments in all public health crises,” Nower said. “Unfortunately, it usually takes some kind of crisis or tragedy to turn the tide.”
A storm of these proportions should demand not only crisis clinical measures, but also community prevention efforts. Yet instead of deploying public health strategies to weather the storm, the U.S. is abandoning them.
Even before the arrival of the so-called tripledemic, U.S. health systems were on the brink. But as the fall surge of illness threatens to capsize teetering hospitals, the will to deploy public health measures has also collapsed. Pediatricians are declaring “This is our March 2020” and issuing pleas for help while public health efforts to flatten the curve and reduce transmission rates of Covid-19 — or any infectious disease — have effectively evaporated. Unmanageable patient volumes are seen as inevitable, or billed as the predictable outcome of an “immunity debt,” despite considerable uncertainty surrounding the scientific underpinnings and practical utility of this concept.
The Covid-19 pandemic should have left us better prepared for this moment. It helped the public to understand that respiratory viruses primarily spread through shared indoor air. Public health practices to stop the spread of Covid-19 — such as masking, moving activities outdoors, and limiting large gatherings during surges — were incorporated into the daily routines of many Americans. RSV and flu are also much less transmissible than Covid-19, making them easier to control with common-sense public health practices.
Instead of dialing up those first-line practices as pediatric ICUs overflow and classrooms close, though, the U.S. is relying on its precious and fragile last lines of defense to combat the tripledemic: health care professionals and medical facilities.
Warnings and advisories recently issued by U.S. public health leaders, clinical leaders, politicians, and the media have consistently neglected to mention masking as a powerful short-term public health strategy that can blunt the surge of viral illness. Instead, recent guidance has exclusively promoted handwashing and cough etiquette. These recommendations run counter to recent calls to build on improved understanding of the transmission of respiratory viruses.
In the U.S.’s efforts to “move on” from thinking about Covid, it has created a “new normal” that is deeply abnormal — one in which we normalize resorting to crisis measures, such as treating patients in tents, instead of using common-sense public health strategies. Treating Covid like the flu — or the flu like Covid — has effectively meant that we treat neither illness as if it were a serious threat to health systems and to public health. Mobilizing Department of Defense troops and Federal Emergency Management Agency personnel to cover health system shortfalls is apparently more palatable than asking people to wear masks.
The tripledemic has already claimed its first child deaths in the U.S., adding to a large ongoing death toll from Covid. Allowing health systems to reach the brink of collapse will lead to many more preventable deaths among pediatric and other vulnerable patients who can’t access the care they need.
By any accounting, these losses are shocking and tragic. But they should strike us as particularly abhorrent and shameful because the tripledemic is a crisis that leaders, health agencies, and institutions have, in a sense, chosen. Over the past year, the Biden administration and its allies have repeatedly encouraged the public to stand down on public health measures, with the President even stating in September that “the pandemic is over.” By moving real risks out of view and failing to push for more robust measures to mitigate Covid, these messages have put the country on a path to its present circumstances, in which pediatric RSV patients are transferred to hospitals hundreds of miles away because there is no capacity to treat them in their own communities.
Living with viruses should mean embracing simple public health measures rather than learning to live with staggering levels of illness and death. Leaders in public health and medicine should issue timely and appropriate guidance that reflects the latest science instead of second-guessing the prevailing winds in public opinion. Instead of self-censoring their recommendations out of fear of political consequences, they should continue to promote the full range of public health strategies, including masking in crowded indoor public places during surges.
The tripledemic should bring renewed urgency to policies that will reduce the toll of seasonal illness on health, education, and the economy. Improvements in indoor air quality in public spaces, including schools, child care centers, and workplaces, can limit the spread of diseases and have many demonstrated health and economic benefits, yet the U.S. continues to lack standards to guide infrastructure or workplace safety standards. Paid leave enabling workers to stay home when they are ill can reduce the transmission of disease as well as loss of income, yet the U.S. is one of the only high-income countries without universal paid sick leave or family medical leave.
Greater effort must also be made to increase vaccination coverage for flu and Covid and bring an RSV vaccine online as quickly as possible. Only about half of high-risk adults under 65 received a flu shot last year, a gap that can be closed with more energetic vaccination campaigns. Reducing annual flu deaths using a broader range of strategies enabled by the pandemic — rather than pegging Covid deaths to them — should be the goal.
Amid the many sobering stories of the tripledemic, there is some good news. As the experience of Covid-19 has shown, it is possible to limit the toll of respiratory viruses like flu and RSV. However, this work requires resources, appropriate policies, and political will. Americans don’t need to accept winter disease surges and overrun health systems as an inevitable new normal. Instead, the country should see the tripledemic as a call to reinvigorate public health strategies in response to these threats to the health of our communities.
The Department of Health and Human Services (HHS) appears set to extend the federal COVID PHE past its current expiration date of January 11, 2023, as HHS had promised to give stakeholders at least 60 days’ notice before ending it, and that deadline came and went on November 11th. Days later the Senate voted to end the PHE, a bill which Biden has promised to veto should it reach his desk. Measures set to expire with the PHE, or on a several month delay after it ends, include Medicare telehealth flexibilities, continuous enrollment guarantees in Medicaid, and boosted payments to hospitals treating COVID patients.
The Gist: Despite growing calls to end the PHE declaration, and even as White House COVID coordinator Dr. Ashish Jha has said another severe COVID surge this winter is unlikely, the White House is likely trying to buy time to resolve the complicated issues tied to the PHE, some of which must be dealt with legislatively.
And with a divided Congress ahead, it remains to be seen how these issues, especially Medicare telehealth flexibilities—a topic of bipartisan agreement—are sorted out. Meanwhile the continuation of the PHE prevents states from beginning Medicaid re-determinations, allowing millions of Americans to avoid being disenrolled.
New York Gov. Kathy Hochul on Sept. 9 declared a state of emergency amid evidence that polio is spreading in communities around the state. The move unlocks federal resources to help the state respond and boost vaccination rates.
Under the declaration, pharmacists, emergency medical personnel and midwives can now administer polio vaccines. The executive order also requires providers to send polio vaccination data to the state’s health department.
“On polio, we simply cannot roll the dice,”said Mary Bassett, MD, health commissioner at the state’s health department. “If you or your child are unvaccinated or not up to date with vaccinations, the risk of paralytic disease is real. I urge New Yorkers to not accept any risk at all.”
The declaration came the same day state health officials reported that the virus had been detected in wastewater samples from Nassau County. Officials have also found the virus in sewage samples from New York City, Orange County, Sullivan County and Rockland County, where the nation’s first polio case in nearly a decade was confirmed July 21 in an unvaccinated man. Health officials have suggested the Rockland County case may just be the “tip of the iceberg” with hundreds of other cases potentially going undetected in the state.
The threat of polio’s resurgence is magnified by the many pockets of unvaccinated residents throughout the state. New York’s polio vaccination rate is 78.96 percent. That figure is lower in many of the counties where the virus has been detected in wastewater. In Rockland County, for example, the polio vaccination rate is 60.3 percent, state data shows. Nationwide, polio vaccination coverage sits at about 93 percent, according to the CDC.
This week, the Food and Drug Administration (FDA) announced a change intended to stretch out the limited supply of monkeypox vaccine doses, allowing the shots to reach five times the number of patients. Monkeypox, a disease in the smallpox family, is spread primarily through skin-to-skin contact, often causing patients to develop painful lesions.
Although most cases resolve within a few weeks, the rapid growth in cases, now more than 9K domestically and 30K globally, is still a cause for concern, leading federal officials to declare a public health emergency last week. The FDA is also recommending that providers administer the vaccine between layers of skin, rather than below the skin into fatty tissue. This dosing change will allow providers to extend the nearly half a million doses not yet sent to states, in order to reach the more than 1.6M Americans considered highest risk.
The Gist: The country is now dealing with two public health emergencies from highly contagious diseases simultaneously. While monkeypox isn’t nearly as transmissible, deadly, or overwhelming to the healthcare system as COVID, the public health response has nonetheless been lackluster (and this week’s new COVID guidance suggests that the CDC has largely given up on managing the response, devolving responsibility to individuals in nearly all settings).
For those hoping that the COVID experience would spark faster action by our public health system, the federal response to monkeypox shows we haven’t applied the lessons learned. Public health authorities aren’t conducting rigorous disease surveillance, testing and treatments remain hard to get, and Congress isn’t dedicating funds for the response. The lack of proactive leadership is likely to result in healthcare providers again bearing the brunt of efforts to manage another unsuppressed viral outbreak.
The Biden administration has declared the monkeypox outbreak a public health emergency — a move that gives officials more flexibility to tackle the virus’ spread.
Details: Department of Health and Human Services secretary Xavier Becerra made the announcement Thursday in a briefing on monkeypox.
Federal health officials can now expedite preventative measures to treat monkeypox without going through a full federal review, the Washington Post reports.
What they’re saying: “We’re prepared to take our response to the next level in addressing this virus,” Becerra said Thursday. “We urge every American to take monkeypox seriously and to take responsibility to help us tackle this virus.”
Dr. Rochelle Walensky, the director of the Centers for Disease Control and Prevention, said the declaration will help “exploit the outbreak” and potentially increase access to care for those at risk.
Dr. Demetre Daskalakis, the White House national monkeypox response deputy coordinator, said “today’s actions will allow us to meet the needs of communities impacted by the virus … and aggressively work to stop this outbreak.”
State of play: Dr. Robert Califf, the commissioner of the Food and Drug Administration, said the U.S. is “at a critical inflection point” in the monkeypox outbreak, requiring “additional solutions to address the rise in infection rates.”
There are 6,600 cases of monkeypox in the U.S. as of Thursday, Becerra said.
There were less than 5,000 cases of monkeypox last week, he added.
The big picture: Biden’s decision to declare monkeypox a public emergency allows him to raise awareness of the virus and unlock more flexibility for spending on ways to treat and tackle the virus.
About 20% of Americans are worried they’ll contract monkeypox, Axios previously reported. But there are still some gaps in Americans’ knowledge of the virus and how it impacts our population.
What’s next: U.S. health officials said that 800,000 monkeypox vaccine doses will be made available for distribution. But in hotspot states for the monkeypox outbreak, there’s a drastic disconnect between the number of doses that local health officials say they need versus what they have been allotted.
The U.S. will receive another 150,000 monkeypox vaccine doses in the strategic national stockpile in September, Dawn O’Connell, administrator at HHS’ Administration for Strategic Preparedness & Response, told reporters Thursday. These were previously scheduled to arrive in October.
New York state declared an imminent threat and San Francisco issued a state of emergency over monkeypox July 28 as the virus continues to spread in the U.S., NBC News reported.
The news comes after the World Health Organization declared monkeypox a global emergency July 23 and as the CDC reported 4,907 confirmed cases nationwide as of July 28. California and New York account for more than 40 percent of the reported cases in the U.S., according to The Washington Post.
In a statement, New York State Commissioner of Health Mary Bassett, MD, said the declaration allows local health departments “to access additional state reimbursement, after other federal and state funding sources are maximized, to protect all New Yorkers and ultimately limit the spread of monkeypox in our communities.” It covers monkeypox prevention response and activities from June 1 through the end of the year.
In San Francisco, the monkeypox public health emergency takes effect Aug. 1, city officials said in a news release. The release, from Mayor London Breed and the San Francisco Department of Public Health, said the declaration “will mobilize city resources, accelerate emergency planning, streamline staffing, coordinate agencies across the city, allow for future reimbursement by the state and federal governments and raise awareness throughout San Francisco about [monkeypox].”
Four other updates:
1. HHS announced July 28 that nearly 800,000 additional monkeypox vaccine doses will be available for distribution to states and jurisdictions. The 786,000 additional doses are on top of the more than 300,000 doses already distributed. This means the U.S. has secured a total of about 1.1 million doses “that will be in the hands of those who need them in the next several weeks,” HHS Secretary Xavier Becerra said during a July 28 news conference. The additional doses will be allocated based on the total population of at-risk people and the number of new cases in each jurisdiction. “This strategy ensures that jurisdictions have the doses needed to complete the second dose of this two-dose vaccine regimen for those who have been vaccinated over the past month,” HHS said in a news release.
2. As of the morning of July 29, the U.S. has held off on declaring a national monkeypox emergency. Mr. Becerra said July 28 that HHS “continue[s] to monitor the response throughout the country on monkeypox” and will weigh any decision regarding a public health emergency declaration based on the response.
3. The monkeypox response is straining public health workers. Health experts are concerned over how the monkeypox response will further deplete the nation’s public health workforce, still strained and burnt out from the ongoing COVID-19 pandemic. Barriers to testing, treatment and vaccine access largely mirror the missteps in the early coronavirus response, Megan Ranney, MD, emergency physician and academic dean of Brown University School of Public Health in Providence, R.I, told The Washington Post. “I can’t help but wonder if part of the delay is that our public health workforce is so burned out,” she said. “Everyone who’s available to work on epidemiology or contract tracing is already doing it for COVID-19.”
4. Monkeypox testing demand is low, commercial laboratories told CNN. In recent weeks, five major commercial laboratories have begun monkeypox testing, giving the nation capacity to conduct 80,000 tests per week. While Mayo Clinic Laboratories can process 1,000 samples a week, it’s received just 45 specimens from physicians since it began monkeypox testing July 11, according to the July 28 CNNreport. “Without testing, you’re flying blind,” William Morice, MD, PhD, president of Mayo’s lab and chair of the board of directors at the American Clinical Laboratory Association, told the news outlet. “The biggest concern is that you’re not going to identify cases and [monkeypox] could become an endemic illness in this country. That’s something we really have to worry about.”