Something I have been writing about and speaking about recently is how difficult it is to operate a hospital in post-Covid America.
The line-up of management and governing obstacles includes both old and new healthcare issues:
Financial instability
Ongoing labor disruption
Remnants of significant healthcare inflation
Payer chaos
A continuing pivot from inpatient to outpatient services
The endless introduction of alternative care options (CVS, Walgreens, Walmart, Amazon, and now Costco)
It takes considerable hard thinking within executive suites to figure out the best way forward; to find the best roadmap through—at a minimum—the six obstacles outlined above. And as I have noted in my recent speaking engagements, a solution to one of these obstacles might actually make others of these obstacles more difficult to solve.
I have in recent weeks been looking for a “thought platform” that can assist hospital C-suite executives in resetting managerial expectations and operational initiatives—expectations and initiatives that can more effectively cope with the current and distressingly difficult environment.
Moving the hospital organizational thought platform from its 2019 managerial themes to a more relevant platform that better suits the challenges of 2023 is a managerial problem all of its own. Simply telling a large and very complex healthcare organization to stop thinking in pre-Covid terms is not likely to accomplish much. Before you can establish the organizational thought platform that best guides your hospital forward, you will need a leadership team that is committed to creating a “listening and learning” healthcare company.
Mr. Watkins is a co-founder of Genesis Advisers and a professor at the IMD Business School in Lausanne, Switzerland. The First 90 Days was originally published in 2003 as a guide to business executives moving into new senior positions of major responsibility. But the book also contains general management advice which is relevant not only to new jobs, but also to executives struggling with fast-changing and especially difficult market conditions.
One of the most compelling chapters in The First 90 Days is a chapter that focuses on the absolute importance of executive learning and the need to accelerate that learning.
While Professor Watkins was making a general business point, I would suggest that the need to accelerate executive learning and listening was never more important than in the “right now” post-Covid healthcare environment. Professor Watkins posed a series of critical leadership learning questions that I have modified to reflect the complex operating conditions of the 2023 hospital.
From that perspective, here are six critical learning questions for the hospital leadership team:
How effective are you as a hospital leader at learning about your current job and how that current job is changing?
What is your learning agenda for your current assignment? Have your day-to-day responsibilities changed so dramatically that you no longer know what you need to know?
Given questions one and two, how should you go about gaining better insight?
What is the best structure for being a top-flight learner within your organization? Note that this is a question that has both individual and organizational implications.
What support is there within your organization for ongoing day-to-day learning? Note this should not be viewed as “training.” This is how executives “learn” through constant interaction with their changing jobs and changing market conditions. We are headed here not toward “skillsets” but toward “learned strategies and insights.” The difference is material.
Professor Watkins suggests creating a learning agenda that relates directly to an ongoing learning plan. What don’t you know right now and how are you going to learn what you don’t know? And, importantly, how has the healthcare macroeconomy made your job more difficult and why?
One of my last blogs focused on the importance of vision and strategy in the post-Covid hospital recovery process; the importance of reinventing the hospital of the future that best fits into a rapidly changing marketplace. This marketplace requires entirely new skillsets and functions on top of changing shared experiences and perceived social values. Finding the right going-forward strategy and vision is the first imperative.
But without executive learning and listening that leads directly to organizational-wide learning and listening, the chances of finding your way to that highest and best and most effective vision and strategy will be greatly diminished.
2022 and 2023 have been particularly difficult operating years for hospital providers. The financial challenges stand out but as we concluded in the August 7, 2023, blog, strategic planning and vision issues may be more compelling over the long term.
We previously identified two strategic issues that need to be reckoned with:
Strategic Relevance. Has everything changed organizationally post-Covid or does it just feel that way? If your strategy still seems dynamic and relevant, how do you capitalize on that? If your strategy feels entirely lost, how do you recapture organizational excitement and enthusiasm?
Vision. How important is organizational vision right now? You know the old saying, “a camel is a horse designed by a committee.” And many vision statements wind up looking more like that camel than like that desired horse. But be that as it may: Covid has been so disruptive to the organizational momentum of hospitals that finding a relevant and executable vision should be top of mind right now.
Given circumstances, one obvious conclusion is that any strategic exercise undertaken in the current moment needs to be well accomplished. Executive teams, clinicians, and Boards are simply too distracted or too tired to spend time on planning processes that are not well thought out and highly directed. This immediate observation next demands a discussion that outlines post-Covid strategic principles, definitions, and the creation of a vision that relates immediately to actionable strategy. It would be an understatement to note that for hospitals there is no “strategic time” to waste.
Start the post-Covid planning process with four very clear strategic definitions:
Vision: A time-bounded view of the future destination of your business.
Strategic Workstreams: The ways you devise to achieve the strategic vision.
Goals: Goals are the lag outcomes that you seek to achieve for your customers.
Metrics: Metrics measure the progress toward the goals.
Working from these definitions then allows you to move toward an organizationally appropriate vision and an actionable strategy that efficiently supports that vision as follows:
The vision should drive growth. Many hospital organizations have stopped growing organically. No growth is harmful financially, clinically, intellectually, and creatively.
The vision should differentiate the business from that of competitors. Everybody and everything competes with hospitals these days: other hospitals, pharmacy companies, insurers, private equity. It has no end.
The vision should endeavor to solve a basic customer problem or problems. The problem list is pretty apparent. The list of helpful solutions has been harder to come by.
The vision should be either incremental or transformational. In all candor, most hospitals’ post-Covid vision is going to be incremental. It takes considerable financial and capital capacity to move toward a transformational vision. That kind of capacity is available at only a small minority of hospitals nationwide.
Recognize that a transformational vision will require active management of culture and stakeholders. If you pivot to a transformational vision, you are likely to upset certain stakeholders and your existing culture may need to also adjust to the transformation.
Be prepared to modify or improve upon the vision, workstreams, and/or goals as you get ongoing feedback during the planning and execution process. Under any circumstances you need to be open to learning all along the way. For this to happen, your organization needs to be a listening organization and a learning organization. Not all hospitals and health systems are.
Does all this sound hard? It should sound hard because it is hard. Leading the hospital back to financial stability while finding a relevant post-Covid vison that proves to be competitive and, at the same time, energizes your team to find renewed purpose in your hospital’s work; that is unforgivably hard.
As Piet Hein, the Danish mathematician, profoundly said, “Problems worthy of attack prove their worth by fighting back.” And fighting back is the hospital job of the moment.
Note: “Culture eats strategy for breakfast” is a quote attributed to management consultant and writer Peter Drucker.
Fifty-four percent of CFOs say that their CEOs are asking them to focus on cost reduction while 40 percent indicate that their CEOs want them honing in on strategy and transformation, according to Deloitte’s “CFO Signals Survey 2Q 2023.”
More than one-quarter of CFOs in the survey reported that their CEOs are asking them to focus on working capital efficiency and risk management while over one-third of CFOs said their CEOs want them focused on strategy and transformation, performance management, revenue growth, investment and capital/financing.
Since 2010, Deloitte has surveyed leading CFOs representing some of North America’s largest companies to provide insight into the business environment, company priorities and expectations, finance priorities and CFOs’ priorities.
Participating CFOs represent diversified, large companies, with 81 percent of respondents reporting revenue in excess of $1 billion. Twenty-three percent are from companies with more than $10 billion in annual revenue, according to Deloitte.
As hospital leaders convene in Seattle this weekend for the American Hospital Association Leadership Summit, their future is uncertain.
Last week’s court decision in favor of hospitals shortchanged by the 340B drug program and 1st half 2023 improvement in operating margins notwithstanding, the deck is stacked against hospitals—some more than others. And they’re not alone: nursing homes and physician practices face the same storm clouds:
Decreased reimbursement from government payers (Medicare and Medicaid) coupled with heightened tension with national health insurers seeking bigger discounts and direct control of hospital patient care.
Persistent medical-inflation driving costs for facilities, supplies, wages, technologies, prescription drugs and professional services (legal, accounting, marketing, et al) higher than reimbursement increases by payers.
Increased competition across the delivery spectrum from strategic aggregators, private equity and health insurers diversifying into outpatient, physician services et al.
Increased discontent and burnout among doctors, nurses and care teams who feel unappreciated, underpaid and overworked.
Escalating media criticism of not-for-profit hospitals/health system profitability, debt collection policies, lack of price transparency, consolidation, executive compensation, charity care, community benefits and more.
Declining trust in the system across the board.
Most hospitals soldier on: they’re aware of these and responding as best they can. But most are necessarily focused only on the near-term: bed needs, workforce recruitment and staffing, procurement costs for drugs and supplies and so on. Some operate in markets less problematic than others, but the trends hold true directionally in every one of America’s 290 HRR markets.
Planning for the long-term is paralyzed by the tyranny of the urgent:
survival and sustainability in 2023 and making guarded bets about 2024 dominate today’s plans. That’s reality. Though the healthcare pie is forecast to get bigger, it’s being carved up by upstarts pursuing profitable niches and mega-players with deep pockets and a take-no-prisoners approach to their growth strategies. The result is an industry nearing meltdown.
Each traditional sector thinks it’s moral virtue more honorable than others. Each blames the other for avoidable waste and inaction in weeding out its bad actors. Each is pays lip service to “value-based care” and “system transformation” while doubling-down on making sure changes are incremental and painless for the near-term. And each believes the long-term destination of the system will be different than the past but no two agree on what that is.
Hospitals control 31% of the spend directly and as much as 43% with their employed physicians included. So, they’re a logical focus of attention from outsiders. Whether not for profit, public or investor owned, all are thought to be expensive and non-transparent and increasingly many are seen as ‘Big Business’ with excessive profits. Complaints about heavy-handed insurer reimbursement and price-gauging by drug companies fall on death ears in most communities. That’s why most are focused on near-term survival and few have the luxury or tools to plan for the future.
As a start, answers to the questions below in the 3-5 (mid-term) and 8–10-year (long-term) time frames is imperative for every hospital leadership team and Board:
Is the status quo sustainable? With annual spending projected to increase at 5.4%/year through 2031– well above population and economic growth rates overall– will employers remain content to pay 224% of Medicare rates to produce profits for hospitals, doctors, drug and device makers and insurers? Will they continue to pass these costs through to their customers and employees while protecting their tax exemptions or will alternative strategies prompt activism? Might employers drive system transformation by addressing affordability, effectiveness, consumer self-care and systemness et al. with impunity toward discomfort created for insiders? Or, might voters reject the status quo in subsequent state/federal elections in favor of alternatives with promised improvement? And who will the winners and losers be?
Are social determinants a core strategy or distraction? 70% of costs in the health system are directly attributable to social needs unmet—food insecurity. loneliness et al. But in most communities, programs addressing SDOH and public health programs that serve less-privileged populations are step-children to better funded hospitals and retail services targeted to populations that can afford them. Is the destination incremental bridges built between local providers and public health programs to satisfy vocal special interest groups OR comprehensive integration of SDOH in every domain of operation? Private investors are wading into SDOH if they’re attached to a risk-based insurance programs like Medicare Advantage and others, but sparingly in other settings. Does the future necessitate re-definition of “community benefits” or new regulations prompting providers, drug companies and payers to fair-share performance. Is the future modest improvement in the “Health or Human Services” status quo OR is system of “Health and Social Services” that’s fully integrated? And might interoperability and connectivity in the entire population become “true north” for tech giants and EHR juggernauts seeking to evade anti-trust constraint and demonstrate their commitment to the greater good? There’s no debate that SDOH is central to community health and wellbeing but in most communities, it’s more talk than walk. Yesterday, SDOH was about risk factors; today, it’s about low-income populations who lack insurance; tomorrow, it’s everyone.
How should the health system of the future be funded? The current system of funding is a mess: In 2021, the federal government and households accounted for the largest shares of national health spending (34 % and 27%, respectively), followed by private businesses (17%), state and local governments (15%), and other private revenues (7%). It will spend $4.66 trillion, employ 19 million and impact every citizen (and non-citizen) directly. But 4 of 10 households have unpaid medical bills. Big employers in certain industries provide rich benefits while half of small businesses provide none. Medicare depends on employer payroll taxes for the lion’s share of its Part A (Hospital) funding exposing the “trust fund” to a shortfall in 2028 and insolvency fears…and so on. Increased public funding via taxes is problematic and debt is more costly as interest rates go up and the municipal bond market tightens. Voters and private employers don’t seem inclined to pay higher taxes for healthcare–:is it worth $13,998 per capita today? $20,426 in 2031? Will high-cost inpatient care and specialty drugs become regulated public utilities in which access and pricing is tightly controlled and directly funded by government? Will private investors and strategic aggregators be required to take invest in community benefits to offset the disproportionate costs borne by hospitals, public health clinics and others? Is there a better formula for funding U.S. healthcare? Other systems of the world spend more on social services and preventive health and less on specialty care. They spend a third less and get comparable if not better outcomes though each is stretched to deal with medical inflation. And in most, government funding is higher, private funding lower and privileged populations have access to private services they pay for directly. Where do we start, and who demands the question be answered?
How will innovations in therapeutics and information technology change how individuals engage with the system? Artificial intelligence will directly impact 60% of the traditional health delivery workforce, negating jobs for many/most. Non-allopathic therapies, technology-enabled self-care, precision medicines, non-invasive and minimally invasive surgical techniques are changing change how care is delivered, by whom and where. Thus, lag indicators based on visits, procedures, admissions and volume are increasingly useless. How will demand be defined in the future? Who will own the data and how will it be accessed? And how will the rights of patients (consumers) be protected in courts and in communities? In the future, information-driven healthcare will be much more than encounter data from medical records and claims-based analyses from payers. It will be sourced globally, housed centrally and accessed by innovators and consumers to know more about their health now and next. Within 10 years, generative AI coupled with therapeutic innovation will fundamentally change roles, payments and performance measurement in every domain of healthcare. Proficiency in leveraging the two will anchor system reputations and facilitate significant market share shifts to high value, high outcome, lower cost alternatives…whether local or not.
How will regulators and court decisions enact fair competition, consumer choices and antitrust protections? The current political environment is united around reforms that encourage price transparency and affordability. FTC and DOJ leaders are aligned on healthcare oversight with a decided bent toward heightened enforcement and tighter scrutiny of proposed deals (both vertical and horizontal integration). But their leaders’ terms are subject to political appointments and elections: that’s an unknown. And while recent rulings of the conservative leaning Supreme Court are problematic to many in healthcare, their rulings are perhaps more predictable than policies, rules and regulations directly impacted by election results.
For hospital leaders gathering in Seattle this week, and in local board meetings nationwide, necessary attention is being given the near-term issues all face. But longer-term issues lurk: the future does not appear a modernized version of the past for anyone in U.S. healthcare, especially hospitals. And among hospitals, fundamental precepts—like tax exemptions for “not-for-profit” hospitals, community benefits and charity care in exchange for tax exemption, EMTALA et al. regulations that require access without pre-condition are among many that will re-surface as the long-term view of the health system is re-considered.
To that end, the questions above deserve urgent discussion in every hospital board room and C suite. Trade-offs aren’t clear, potential future state hospital scenarios are not discreet and winners and losers unknown. But a fact-driven process recognizing a widening array of players with deep pockets and fresh approaches is necessary.
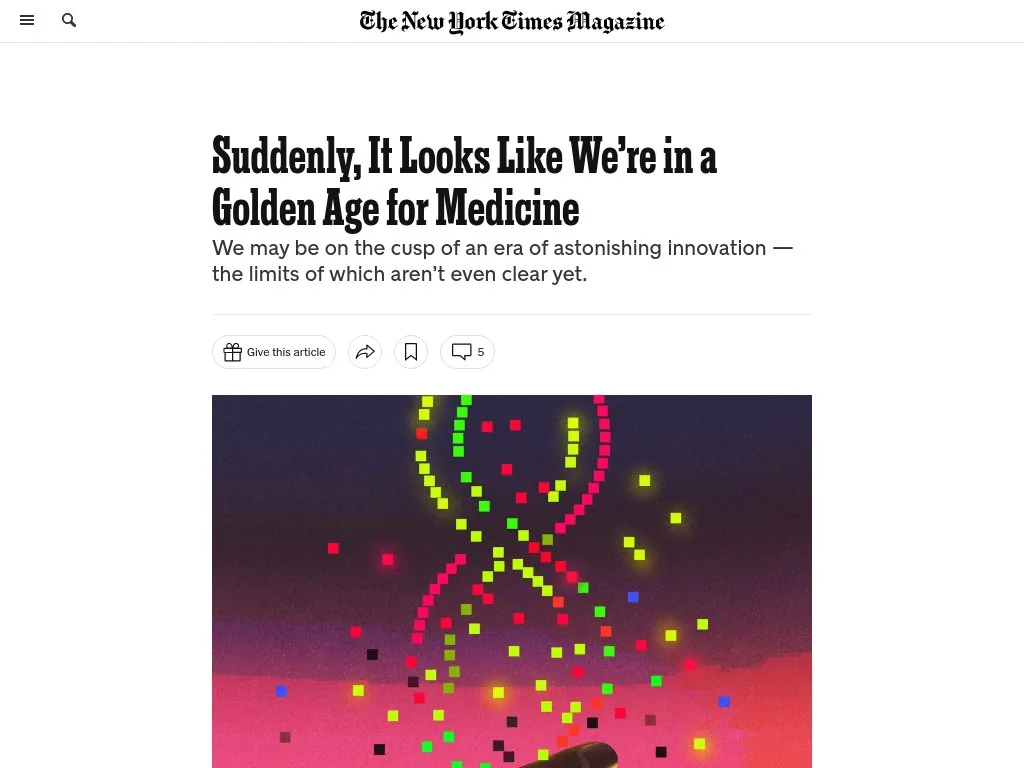
The New York Times Magazine published an encouraging piece about the impressive series of recent medical breakthroughs, many of which have been in the works for decades.
Challenging the conventional wisdom that disruptive scientific breakthroughs have slowed over time, the article points out that the last five years of medicine have featured the rollout of mRNA vaccines, the first instance of a person receiving CRISPR gene therapy, and development of next-generation cancer treatment and weight-loss drugs.
The Gist: The expanding innovation pipeline not only brings excitement and optimism for patients and physicians, but also has the potential to dramatically impact long-established care delivery pathways.
Case in point: used at scale, new weight loss drugs could curb obesity-related chronic diseases and joint replacements—while possibly increasing the incidence of Alzheimer’s disease and cancer as more people live longer lives.
Providers planning for facility and other long-term investments must think through scenarios about how these early, but very promising, innovations could alter demand and shift care delivery needs over coming decades.
Health systems are ramping up investments in ambulatory surgery centers and forming joint ventures with outpatient partners to accelerate the development of new centers. The trend is picking up steam as complex procedures increasingly move to ASCs, which are steadily growing as the preferred site of service for physicians, patients and payers.
Tenet Healthcare, one of the largest for-profit health systems in the country, has been paying close attention to outpatient migration for years and has cemented itself as the leader in the ASC space. It now operates more than 445 ASCs — the most of any health system — and 24 surgical hospitals, according to its first-quarter earnings report.
United Surgical Partners International, Tenet’s ASC company, strengthened its footing in the ASC market after its $1.2 billion acquisition of Towson, Md.-based SurgCenter Development and its more than 90 ASCs in December 2021. Over the next several years, USPI will inject more than $250 million into ASC mergers and acquisitions and work with SurgCenter to develop at least 50 more ASCs, according to terms of the transaction.
The SurgCenter acquisition was completed shortly after Tenet sold five Florida hospitals to Dallas-based Steward Health Care for $1.1 billion. In 2022, Tenet also acquired Dallas-based Baylor Scott & White Health’s 5 percent equity position in USPI to own 100 percent of the company’s voting shares and paid $78 million to acquire ownership of eight Compass Surgical Partners ASCs.
These ASC investments and hospital sales make it clear that CEO Saum Sutaria, MD, sees surgery centers to become Tenet’s main growth driver in the coming years. Dr. Sutaria has described USPI as the company’s “gem for the future,” and aims to have 575 to 600 ASCs by the end of 2025.
While Tenet continues to increase its ASC market share, its closest competitor is Deerfield, Ill.-based SCA Health, which UnitedHealth Group’s Optum acquired for $2.3 billion several years ago.
SCA has more than 320 ASCs, but has expanded its focus on value-based care under Optum and is doubling down on supporting physicians across the specialty care continuum rather than operating as an ASC company “singularly focused on partnering with surgeons in their ASCs,” SCA CEO Caitlin Zulla told Becker’s.
While Tenet may operate the most ASCs among health systems, it lags behind Optum in terms of the number of physicians it employs. Optum is now affiliated with more than 70,000 physicians, making it the largest employer of physicians in the country, and is continuing to add to that through mergers and acquisitions.
Nashville, Tenn.-based HCA Healthcare, another for-profit system, employs or is affiliated with more than 47,000 physicians, but is also ramping up its surgery center portfolio. HCA comprises 2,300 ambulatory care facilities, including more than 150 ASCs, freestanding emergency rooms, urgent care centers and physician clinics, according to its first-quarter earnings report.
Like Tenet and Optum, HCA is heavily focused on expanding its outpatient portfolio. The company ended 2021 with 125 ASCs, four more than it had at the end of 2020, and added more than 25 ASCs last year. It is focused on both developing and acquiring surgery centers in the coming years.
The other big ASC operators include Nashville, Tenn.-based AmSurg, with more than 250 surgery centers, and Brentwood, Tenn.-based Surgery Partners, with more than 120 centers. Surgery Partners spent about $250 million on ASCs acquisitions last year and recently signed collaboration agreements with two large health systems —- Salt Lake City-based Intermountain Health and Columbus-based OhioHealth.
Oakland, Calif.-based Kaiser Permanente has 62 freestanding ASCs and outpatient surgery departments on its hospital campuses, a spokesperson for the health system told Becker’s.
At the end of a meeting last week with a health system executive team, the system’s COO asked us a question: “Your concept of a consumer-focused health system centered around treating patients as members describes exactly how we want to relate to our patients, but we’re not sure about the timing. Could you give us a list of the ‘no regrets’ investments you’d recommend for health systems looking to do this?”
We frequently get asked about “no regrets” strategies:
decisions or investments that will be accretive in both the current fee-for-service system as well as a future payment and operational model oriented around consumer value. The idea is understandably appealing for systems concerned about changing their delivery model too quickly in advance of payment change. And there is a long list of strategies that would make a system stronger in both fee-for-service and value: cost reduction, value-driven referral management, and online scheduling, just to name a few.
But as we pointed out, the decision to pursue only the no-regrets moves is a clear signal that the organization’s strategy is still tied to the current payment model.
If the system is truly ready to change, strategy development should start with identifying the most important investments for delivering consumer value. It’s fine to acknowledge that a health system is not yet ready, but we cautioned the team that they should not rely on the external market to provide signals for when they should undertake real change in strategy.
External signals—from payers, competitors, or disruptors—will come too slowly, or perhaps never. At some point, the health system should be prepared to lead innovation, introduce a new model of value to the market, and define and promote the incentives to support it.
Real change will require disruption of parts of the current business and cannot be accomplished with “no-regrets investments” alone.
Healthcare’s most recent billion-dollar deal took the industry by surprise, leaving medical experts and hospital leaders grappling to comprehend its implications.
In case you missed it, California-based Kaiser Foundation Health Plan and Hospitals, which make up the insurance and facilities half of Kaiser Permanente, announced the acquisition of Geisinger, a Pennsylvania-based health system once acknowledged by President Obama for delivering “high-quality care.”
Upon regulatory approval, Geisinger will become the first organization to join Risant Health, Kaiser Foundation’s newly created $5 billion subsidiary. According to Kaiser, the aim is to build “a portfolio of likeminded, nonprofit, value-oriented, community-based health systems anchored in their respective communities.”
Having spent 18 years as CEO of The Permanente Medical Group, the half of Kaiser Permanente responsible for the delivery of medical care, I took great interest in the announcement. And I wasn’t alone. My phone rang off the hook for weeks with calls from reporters, policy experts and healthcare executives.
After hundreds of conversations, here are the three most common questions I received about the acquisition—and the implications for doctors, insurers, health-system competitors and patients all over the country.
Question 1: Why did Kaiser acquire Geisinger?
Most callers wanted to know about Kaiser’s motivation, figuring there must’ve been more to the acquisition than the press release indicated. Although I don’t have inside information, I believe they were right. Here’s why:
Kaiser Permanente has a long and ongoing reputation for delivering nation-leading care. The organization has consistently earned the highest quality and patient-satisfaction rankings from the National Committee for Quality Assurance (NCQA), Leapfrog Group, JD Power and Medicare.
And yet, despite a 78-year history, dozens of hospitals and 13 million members across eight states, Kaiser Permanente is still considered a coastal—not national—health system. It maintains a huge market share in California and a strong presence in the Mid-Atlantic states, yet the organization has failed repeatedly to replicate that success in other geographies.
With that context, I see two compelling reasons why the Kaiser Foundation Health Plan and Hospitals wish to become a national brand:
Influence. Elected officials and regulatory bodies often turn to healthcare’s biggest players to set legislative agendas and carve out national policy. At that table, there are a limited number of seats. By shedding its reputation as a “local” health system, Kaiser could earn one.
Survival. In recent years, companies like Amazon, CVS and Walmart have been scooping up organizations that provide primary care, telehealth, home health and specialty care services. These “retail giants” are spending up to $13 billion per acquisition. And they’re consuming already-successful healthcare companies like One Medical, Oak Street Health, Signify, Pill Pack and many others. Like an army preparing for war, these corporate behemoths are amassing the components needed to battle the traditional healthcare incumbents and ultimately oust them entirely.
The Geisinger deal expands Kaiser’s footprint, adding 600,000 patients, 10 hospitals and 100 specialty and primary care clinics. These assets lend gravitas, even though Geisinger also comes with a 2022 operating loss of $239 million.
The lesson to draw from this first question is clear: size matters. The days of solo physicians and stand-alone hospitals are over. Nostalgia for medicine’s folksy, home-spun past is understandable but futile. To survive, healthcare players must get bigger quickly or team up with someone who can. That insight leads to the next question and lesson.
Question 2: How much value will Kaiser give Geisinger?
Almost everyone I’ve spoken with understands Kaiser’s desire for greater national influence, but they’re less sure how this deal will affect Geisinger Health.
Geisinger’s Pennsylvania-based hospitals and clinics have been locked in territorial battles for years with surrounding health systems. More recently, the pandemic, combined with staffing shortages and national inflation, have challenged Geisinger’s clinical performance and eroded its bottom line.
Assuming Kaiser plans to invest roughly $1 billion in each of the four to five health systems it’s planning to acquire, that surge in cash inflow will provide Geisinger with temporary financial safety. But the bigger question is how will Kaiser improve Geisinger’s value-proposition enough to grow its market share?
In public comments, Kaiser leaders spoke of the acquisition as an opportunity for Risant to “improve the health of millions of people by increasing access to value-based care and coverage, and raising the bar for value-based approaches that prioritize patient quality outcomes.”
Many of the experts I spoke with understand Kaiser’s value intent. But they question how Kaiser can could deliver on that promise since The Permanente Medical Group (TPMG) wasn’t involved in the deal.
If, hypothetically, Kaiser and Permanente leaders were to strike a deal to collaborate in the future, TPMG’s physician leaders could bring tremendous knowledge, experience and expertise to the table. Otherwise, I agree with those who’ve expressed doubt that Kaiser, alone, will be able to significantly improve Geisinger’s clinical performance.
Health plans and insurance companies play an important role in financing medical care. They possess rich data on performance and can offer incentives that boost access to higher-quality care. But insurers don’t work directly with individual doctors to coordinate medical care or advance clinical solutions on behalf of patients. And without strong physician leadership, the pace of positive change slows to a crawl. As a example, research conducted within The Permanente Medical Group found that it takes only three years to turn a proven clinical advance into standard practice—that’s nearly six times faster than the national average.
For decades, the secret sauce for Kaiser Permanente has been the cohesive success of its three parts: Kaiser Health Plan, Kaiser Foundation Hospitals and The Permanente Medical Group.
And KP’s results speak for themselves:
90% control of hypertension for members (compared to 60% for the rest of the country)
30% fewer deaths from heart attack and stroke (compared to the rest of the country)
20% fewer deaths from colon cancer
The big lesson: insurance, by itself, doesn’t drive major improvements in medicine. It must be a combined effort between forward-looking insurers and innovative, high-performing clinicians.
But there’s another takeaway here for doctors everywhere: now is the time to join forces with other clinicians in your community. Together, you can collaborate to improve clinical quality. You can augment access and make care more affordable for patients. Simultaneously, this is the time for the insurers and the retail giants to figure out which medical groups can deliver the best care and make the best partners. Neither side will flourish alone. And this leads to a third question and lesson.
Question 3: Will the deal work?
Almost all of my conversations ended with this query. I say it’s too early to tell. But as I look years down the road, one part of the deal, in particular, gives me doubt.
Today, Geisinger uses a hybrid reimbursement model—blending both “value-based” care payments with traditional “fee-for-service” insurance plans. In addition to offering its own coverage, it contracts with a variety of other insurance companies. Rarely have I seen this scattered approach succeed.
Most healthcare observers understand the inherent flaw in the “fee for service” (FFS) model is also its greatest appeal to providers: the more you do the more you earn. FFS is how nearly all financial transactions take place in America (i.e., provide a service, earn a fee). In medicine, however, this financial model results in frequent over-testing and over-treatment with minimal if any improvement in clinical outcomes, according to researchers.
The “value-based” alternative to FFS involves prepaying for care—a model often referred to as “capitation.” In short, capitation involves a single fee, paid upfront for all the medical care provided to a defined population of patients for one year based on their age and health status. The better an organization at preventing disease and avoiding complications from chronic illness, the greater its success in both clinical quality and affordability.
Within the small world of capitated healthcare payments, there’s an important element that often gets overlooked. It makes a big difference who receives that lump-sum payment.
In the case of Kaiser Permanente, capitated payments are made directly to the medical group and the physicians who are responsible for providing care. In almost every other health system, an insurance company collects capitated payments but then pays the medical providers on a fee-for-service basis. Even though the arrangement is referred to as capitated, the incentives are overwhelmingly tied to the volume of care (not the value of that care).
In a mixed-payment model, doctors and hospitals invariably prioritize the higher paying FFS patients over the capitated ones. When I think about these conflicting incentives, I’m reminded of a prominent medical group in California. It had a main entrance for its fee-for-service patients and a second, smaller one off to the side for capitated patients.
I doubt the time spent with the patient—or the overall care provided—was equal for both groups. When income is based on quantity of care, not quality, clinicians focus more on treating the complications of chronic disease and medical errors rather than preventing them in the first place. Geisinger has walked this tightrope in the past, but as economic pressures mount, I fear doctors will find the two sets of incentives conflicting and difficult to navigate.
The big lesson: as financial pressures mount, the most effective approaches of the past will likely fail in the future. All healthcare organizations will need to make a decision: keep trying to drive volume and prices up through FFS or shift to capitation. Getting caught in the middle is a prescription for failure.
Examining the healthcare acquisitions made by Amazon and CVS, it’s clear these giants have decided to move aggressively toward a model more like Kaiser Permanente’s—one that brings insurance, pharmacy, physicians and sophisticated IT systems under one roof. These companies, along with Walmart, are aggressively marching down a path toward capitation, focusing on Medicare Advantage (the value-based option for Americans 65+) as an entry point.
So far, Geisinger has hedged its bets by maintaining a hybrid revenue stream. I doubt they can do so successfully in the future. That brings us to a final question.
The biggest question remaining
Over the next decade, hospital systems, insurers and retailers will battle for healthcare supremacy. The most recent Kaiser-Geisinger deal reflects an industry that’s undergoing massive change as health systems face intensifying pressure to remain relevant.
The most important issue to resolve is whether these shifts will ultimately help or harm patients. I’m optimistic for a positive outcome.
Whether or not the retail giants displace the incumbents, they will redefine what it takes to win. For all their faults, companies like Amazon and Walmart care a lot about meeting the needs of customers—a mindset rarely found in today’s healthcare world. As these companies grow ever larger, they’ll place consumer-oriented demands on doctors and hospitals. This will require care providers to deliver higher quality care at more affordable prices.
The retailers will only do deals with the best of the best. And they’ll kick the underachievers to the curb. They’ll use their sophisticated IT systems to better coordinate and innovate medical care. Insurers, hospitals and doctors who fail to keep up will be left behind.
Over time, patients will find themselves with far more choices and control than they have today. And I’m optimistic that will be good for the health of our nation.