The showdown between the Biden administration and the state of Texas over Medicaid expansion continued to escalate this week. Sen. John Cornyn (R-TX) said he planned to place a hold on the confirmation of Chiquita Brooks-LaSure to become Administrator of the Centers for Medicare & Medicaid Services (CMS), until his concerns over the agency’s move last week to rescind a waiver extension previously granted by the Trump administration were addressed.
The so-called “1115 waiver”—worth more than $11B annually—would have extended by a decade Texas’ ability to use Medicaid funds to cover hospital costs for uninsured residents, rather than expanding Medicaid coverage under the Affordable Care Act (ACA). In rescinding the waiver extension, the Biden administration cited the lack of a public notice process before the waiver was granted, and said that the state’s existing waiver would instead expire next year, as previously scheduled.
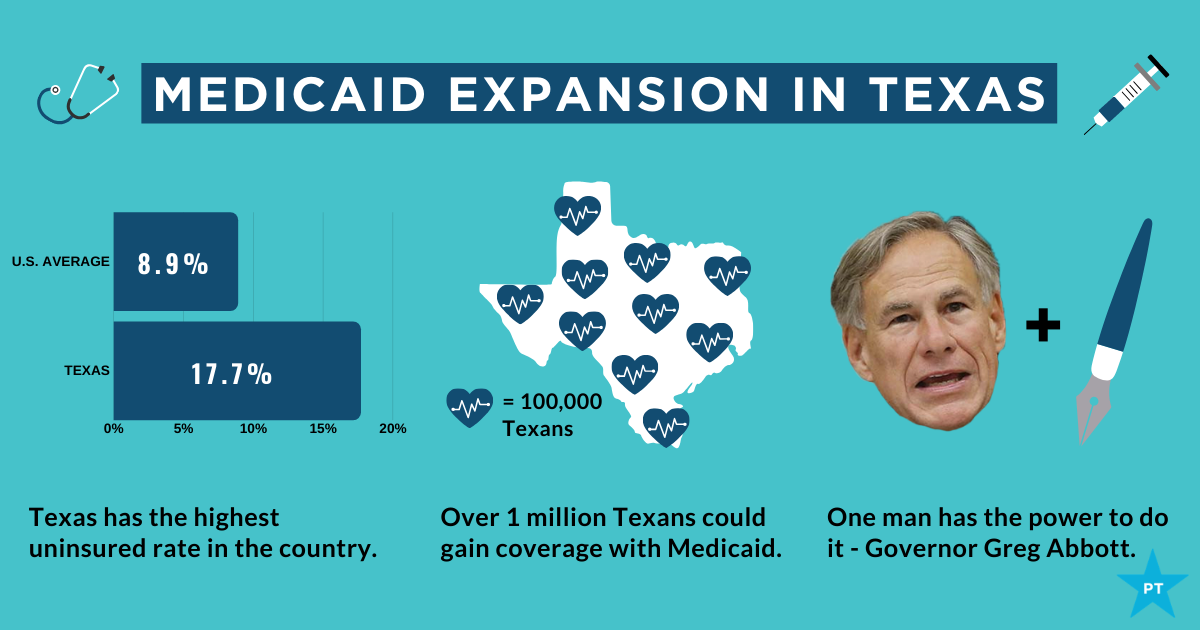
Sources inside the administration told the Washington Post last week thatthe move was intended to force Texas’ hand on Medicaid expansion; the state is one of 12 that have not expanded Medicaid, leaving it with the largest share of uninsured residents of any state, with eligibility currently limited to pregnant women, children, people with disabilities, and families with monthly incomes under $300 per month, or 13.6 percent of the federal poverty level.
Enticing the dozen remaining holdout states to expand Medicaid is an important policy priority for the new administration.A key component of the recently passed American Rescue Plan Act is a package of enhanced incentives for those states to expand eligibility, offering an extended 90 percent federal match, in addition to increased funding for existing Medicaid populations.
Although none of the non-expansion states have budged yet, there has been renewed focus among state lawmakers on Medicaid expansion, including in Texas, where the idea had garnered bipartisan support. However, on Thursday, the Texas legislature voted down a proposal aimed at pushing the state toward expanding coverage for the uninsured, by an 80-68 margin. Meanwhile, the rescission of Texas’ waiver has angered the state’s Republican leadership, along with the Texas Hospital Association, whose members have benefited from the waiver’s use of funds to reimburse them for delivering uncompensated care.
While Cornyn’s hold will not ultimately stop the confirmation of the new CMS leader, the escalation on both sides over the past several days surely makes finding a compromise solution less likely. The Biden health policy team is said to be developing a new proposal, as part of an upcoming legislative package, to use the ACA marketplace to offer coverage to people in non-expansion states who might otherwise be eligible for Medicaid—yet another attempt to address one of the longest-standing points of contention stemming from the 2010 health reform law.
President Biden promised on the campaign trail to expand the Affordable Care Act to cover more of the roughly 29 million nonelderly Americans (about 11 percent of that population) who remain uninsured. He also said he’d strengthen the law by, for instance, providing an accessible and affordable public option and increasing tax credits to make it easier for people who buy insurance on their own to afford monthly premiums. Once in office, Biden immediately moved to reopen the period when people could enroll in the ACA marketplaces.
Unfortunately, the administration is paying little heed to a problem that is in many ways just as insidious as lack of insurance: underinsurance. That’s when people get too little from the insurance plans that they do have.
After passage of the ACA, the number of Americans lacking any insurance fell by 20 million, dropping to 26.7 million in 2016 — a historic low as a percentage of population. The figure began to creep up again during the Trump administration, reaching 28.9 million in 2019. That’s the problem that the current administration wants to address, and it certainly needs attention.
But according to research by the Commonwealth Fund, a foundation focused on health care, 21.3 percent of Americans have insurance so skimpy that they count as underinsured: Their out-of-pocket health-care expenses, excluding premiums, amount to at least 5 to 10 percent of household income. The limits in coverage mean their plans might provide little financial protection in a health-care crisis.
High-deductible plans offered by employers are one part of the problem. Among people covered by the companies they work for, enrollment in high-deductible health plans rose from 4 percent in 2006 to 30 percent in 2019, according to a report from the Kaiser Family Foundation. The average annual deductibles in such plans are $2,583 for an individual and $5,335 for families.
In theory, high-deductible plans, which make people spend lots of their own money before insurance kicks in, turn people into careful consumers. But research finds that people covered by such plans skip care, both unnecessary (elective cosmetic surgery, for instance) and necessary (cancer screenings and treatment, and prescriptions).Black Americans in these plans disproportionately avoid treatment, widening racial health inequities.
Health savings accountsare designed to blunt the harmful effects of high-deductible plans: Contributions by employers, and pretax contributions by individuals, help to cover costs until the deductible is reached. But not all high-deductible health plans offer such accounts, and many people in lower-wage jobs don’t have them. In the rare cases that they do, they often don’t have extra money to deposit in them.
In a November 2020 article in the journal Health Affairs, scholars affiliated with Brown University and Boston University found that enrollment in high-deductible plans had increased across all racial, ethnic and income groups from 2007 to 2018; they also found that low-income, Black and Hispanic enrollees were significantly less likely than other groups to have a health savings account — and the disparities had grown over time.
The short-term health-care plans — a.k.a. “junk” plans — that the Trump administration expanded also contribute to the problem of underinsurance. They often have low premiums but do not cover preexisting conditions or basic services like emergency health care.
Fortunately, proposals like Biden’s that make health care more accessible also tend to address the problem of underinsurance, at least in part. For example, to make individual-market insurance more affordable, Biden proposes expanding the tax credits established under the ACA. His plan calls for removing the cap on financial assistance, now set at 400 percent of the federal poverty level, in the insurance marketplaces and lowering the statutory limit on premiums to 8.5 percent of income (from nearly 10 percent).
The president also proposes to peg the size of the tax credits that subsidize premiums to the best plans on the marketplaces, the “gold” plans, rather than “silver” plans. This would increase the size of these credits, thereby making it easier for Americans to afford more-generous plans with lower deductibles.
The most ambitious Biden proposal is a public option, which would create a Medicare-like offering on marketplaces, available to anyone.Pairing this with allowing any American to opt out of their employer plan if they found a better deal on HealthCare.gov or their state marketplace — which they can’t now — would help some people escape high-deductible plans. The public option would also eliminate premiums and involve minimal to no cost-sharing for low-income enrollees — especially helpful for uninsured (and underinsured) people in states yet to expand Medicaid.
Given political realities, however, this policy may not see the light of day. So it would be best to target underinsurance directly. Most people with high-deductible plans get them through an employer. Yet unlike in the marketplace plans, the degree of cost sharing in these employer plans is the same for low-income as well as high-income employees. To deal with that problem, the government could offer incentives for employers to expand the scope of health services they cover — even in high-deductible plans. Already, many such plans exempt from the deductible some primary-care visits and generic-drug prescriptions. The list could grow to include follow-up visits and certain specialist care.
Instead of encouraging health savings accounts, the government could offer greater pretax incentives that encourage employers to absorb some of the costs that they have shifted onto their lower-income employees; that would help to prevent the insurance equity gap from widening further. The government could compensate employers that cover co-pays or other costs for their low-income employees. It could also subsidize employers that move away from high-deductible plans, at least for lower-income people.
Health insurance is complicated: More-affordable premiums are good only if they don’t bring stingy coverage. Greater investment in well-trained (and racially diverse) “navigators” — the people who help Americans enroll in plans on the federal marketplace, for example — would make it less likely that consumers would choose high-deductible plans without grasping their downsides. But it’s also important that people have options beyond risky high-deductible coverage.
The ACA expanded coverage dramatically — but the government needs to make sure that coverage amounts to more than an unused insurance card.
The American Rescue Plan stimulus package just sweetened the deal for the twelve holdout states that haven’t yet expanded Medicaid.In exchange for expanding eligibility to the roughly four million adults with incomes up to 133 percent of the federal poverty level, new expansion states will also be eligible for afive percent increase in the federal matching rate for their entire traditional Medicaid population for a two-year period.
The graphic above shows the cumulative fiscal impact for holdout states, should all Medicaid-eligible individuals enroll. Since the traditional Medicaid population is so much larger than the expansion population, the temporary increase more than offsets states’ cost to cover their share of the expansion, resulting in an estimated net fiscal benefit of almost $10B. While the net benefit would vary from state to state, a Kaiser Family Foundation analysis found the two most populous non-expansion states, Texas and Florida, could net up to $1.9B and $1.8B respectively across the two-year period.
Medicaid expansion has had a significant positive financial impact on hospitals, reducing uncompensated care and increasing overall operating margin by an average of 1.7 percent.
A recent analysis by the Center on Budget and Policy Priorities founduncompensated care costs as a share of hospital expenses fell an average of 45 percent in Medicaid expansion statesbetween 2013 and 2017. So far, only two states eligible for the enhanced expansion, Alabama and Wyoming, have signaled interest in taking advantage of the new deal. Convincing the remaining ten to follow suit will require intense and coordinated advocacy efforts from the healthcare and business communities. Making the financial case for expansion should prove straightforward, compared to overcoming long-entrenched political opposition.
The Democratic bill has $410 billion in stimulus checks and $360 billion in aid to state and local governments.
Expanded unemployment benefits cost $242 billion.
School spending is nearly $170 billion spread out over 10 years.
There are a few big chunks of money in the American Rescue Plan Act that have generated a lot of news coverage and are pretty well known. In response to a reader’s request, we present the whopping $1.86 trillion spending plan in pie chart form.
There are the $1,400 checks (or more likely deposits) to many citizens or permanent legal residents and their dependents. That comes to about $410 billion.
Aid to state, local, territorial and tribal governments costs about $360 billion.
The bill boosts and extends unemployment benefits. Add another $242 billion.
Over the next 10 years, the law spends nearly $170 billion on education. That includes $129 billion for K-12 schools — both public and private — and about $40 billion for higher education.
The money for vaccines and corralling the coronavirus became a political talking point. Democrats touted the $20-25 billion they included for vaccine supplies and research. Republicans argued that the bill spent less than 10% of its total cost on COVID-19.
People will parse the numbers in different ways. Some only count money spent directly on vaccine production. Some look more broadly at the economic damage wrought by the virus. We looked for money that went towards health care, whether that meant improving treatment on tribal lands, adding health care workers at clinics, or anything that reduced the health impacts of the pandemic.
We put the bill’s total public health spending at $143 billion.
Within that, the single biggest line item is $47.8 billion for mitigating the disease, a broad description that includes testing and surveillance. There is also $15 billion for COVID-related health care for veterans, $7.6 billion to help community health centers distribute vaccines, and about the same amount to the Centers for Disease Control and Prevention for roughly the same purpose.
The chart above lays out how the money breaks down.
All of the amounts so far come to $1.3 trillion over 10 years.The bill’s total cost is $1.86 trillion, which leaves about $500 billion dollars to flesh out.
The law has over $40 billion for child care. Money to keep people in their homes and to house the homeless comes to about $44 billion. There is $10 billion to put food on people’s tables. The expected cost of temporarily boosting the child tax credit is $109 billion.
In our chart, we fold all of that, plus subsidies for pensions and health insurance premiums, into the category of support for families. Our total is $352 billion.
Our last distinct category is transportation. Under that umbrella, we put $30 billion for mass transit, $15 billion for the airline industry, $8 billion for airports, and other related activities. That came to $58 billion.
The catch-all bucket of other spending includes items such as $66 billion for businesses, $50 billion for disaster relief at the Federal Emergency Management Agency, and $7 billion to expand broadband internet.
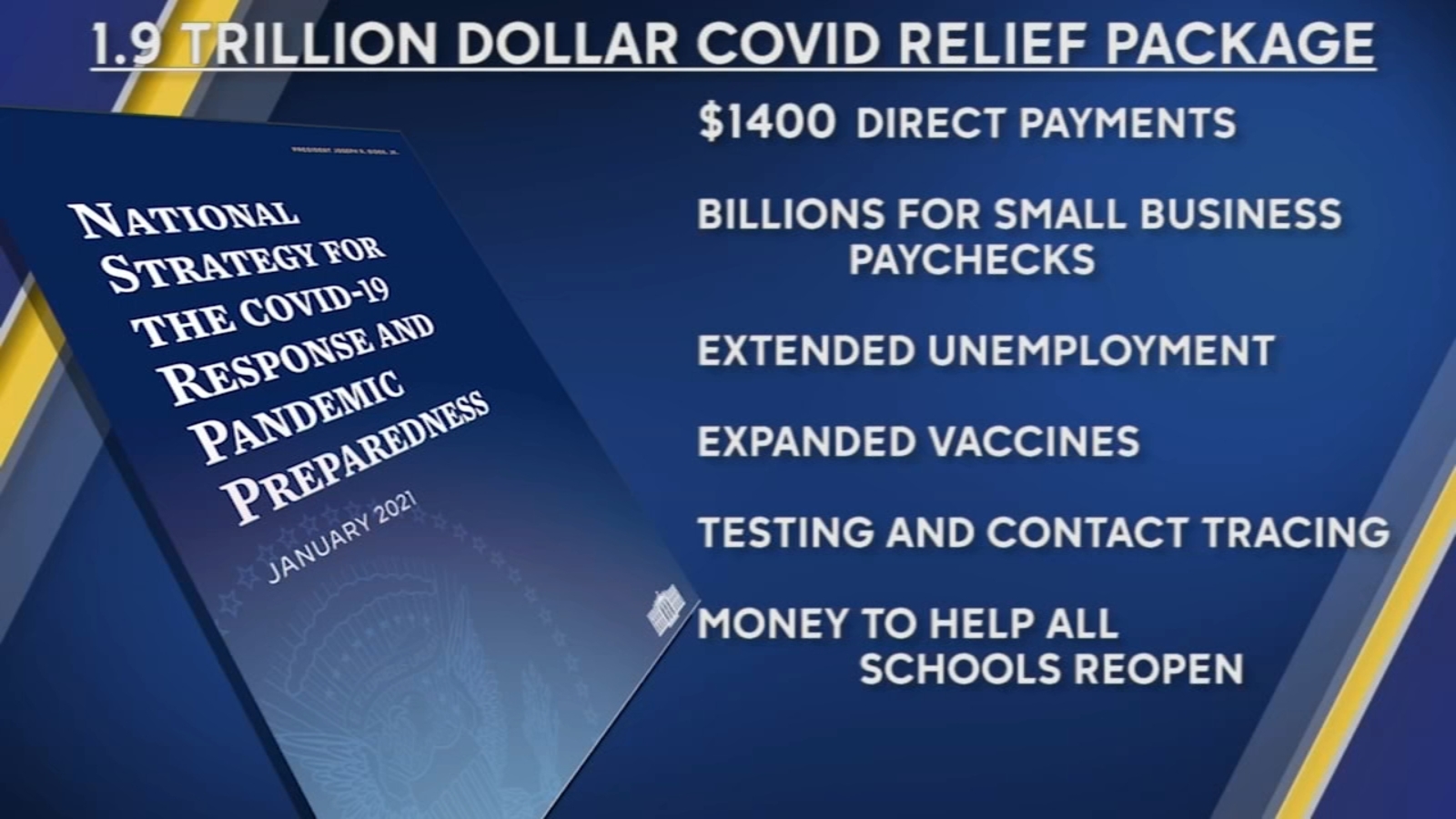
On Thursday, President Biden signed the American Rescue Plan (ARP) Act of 2021 into law, committing nearly$1.9T of federal spending to boost the nation’s recovery from the coronavirus pandemic. In addition to direct payments to American families, extension of unemployment benefits, several anti-poverty measures, and aid to state and local governments, the plan also contains several key healthcare measures.
Approved by Congress on a near party-line vote using the budget reconciliation process, the law includes thebroadest expansion of the 2010 Affordable Care Act (ACA) to date. It extends subsidies for upper-middle income individuals to purchase coverage on the Obamacare exchanges, caps premiumsfor those higher earners at a substantially lower level, and boosts subsidies for those at the lower end of the income scale.
The Congressional Budget Office (CBO) estimates that expanded ACA subsidies in the ARPwill result in 2.5M more Americans gaining coverage in the next two years. Fully subsidized COBRA coverage for workers who lost their jobs due to COVID is also extended through the end of September, which the CBO estimates will benefit an additional 2M unemployed Americans.
The ARP also puts in place new support for Medicaid, enhancing coverage for home-based care, maternity services, and COVID testing and vaccination, and providing new incentives for the 12 states which haven’t yet expanded Medicaid eligibility under the ACA to do so. In addition to the ACA’s 90 percent match for those states’ Medicaid expansion populations, the lucky dozen will also receive a 5 percent bump to federal matching for the rest of their Medicaid populations should they choose to expand.
Three policy changes of keen interest to providers were left out of the final version of the bill. First, while a special relief fund of $8.5B was created for rural providers, there was no additional allocation of relief funds for hospitals and other providers, similar to the $178B allocated by the CARES Act, despite initial proposals of up to $35B in additional funding. (Around $25B of the initial round of provider relief is still unspent.) Second, the ARPdid not extend or alter the repayment schedule for advance payments to providers made last year, in spite of industry pressure to implement more favorable repayment conditions. Finally, the new law does not extend last year’s pause on sequester-related cuts to Medicare reimbursement, although the House is expected to consider a separate measure to address that issue next week.
Notably, the coverage-related provisions of the ARP are only temporary, lasting through September of next year. That sets up the 2022 midterm elections as yet another campaign cycle dominated by promises to uphold and protect the Affordable Care Act—by then a 12-year-old law bolstered by this week’s COVID recovery legislation.
The House on Wednesday passed the mammoth $1.9 trillion COVID-19 relief package, which President Biden is expected to sign Friday.
The House approved the relief package in a starkly partisan 220-211 vote, sending the legislation to the White House and clinching Democrats’ first big legislative victory in the Biden era. No Republicans voted for the package and all but one House Democrat—Rep. Jared Golden of Maine—supported it. The Hill’s Cristina Marcos has more here.
The political split: Unlike the previous relief measures enacted last year, Democrats barely bothered to negotiate with Republicans and pushed the relief package through Congress along party lines using the budget reconciliation process. That allowed them to go as big as they wanted to go without running into a Senate GOP filibuster.
Republicans argue the use of a process dodging the filibuster shows Biden wasn’t serious about bringing unity, and House GOP lawmakers on Wednesday warned of the bill’s total cost.
But Democrats think Republicans will pay for their opposition to the popular bill and argued that they would oppose anything Biden proposed.
What’s in the $1.9T COVID-19 relief package: Along with $1,400 direct payments to households, an extension of expanded unemployment benefits, and aid for state and local governments, the package is loaded with other provisions intended to speed up the recovery from the recession and help struggling families fight the impact of COVID-19.
Tax credits: The bill increases the child tax credit for households below certain income thresholds for 2021 and makes it fully refundable, and also expands the earned income tax credit for the year.
Child care: $15 billion for grants to help low-income families afford child care and increases the child and dependent care tax credit for one year.
Pensions: $86 billion to bailout struggling union pension funds.
Transportation: $30 billion to bolster local subway and bus systems, $8 billion for airports, $1.5 billion for furloughed Amtrak workers, and $3 billion for wages at aerospace companies.
Housing: $27.4 billion in emergency rental assistance, another $10 billion to help homeowners avoid foreclosure, $5 billion in vouchers for public housing, $5 billion to tackle homelessness and $5 billion more to help households cover utility bills.
Small businesses: The American Rescue Plan broadens eligibility guidelines for the Paycheck Protection Program, allowing more nonprofit entities to be eligible, adds $15 billion in emergency grants and also sets aside more than $28 billion in funding for restaurants.
ObamaCare subsidies and Medicaid expansion: The bill increases ObamaCare subsidies through 2022 to make them more generous, a longtime goal for Democrats, and opens up more fully subsidized plans to individuals. It also would provide extra Medicaid funding to states that expand the program and have yet to do so.