A Florida taxi driver and his wife had seen enough conspiracy theories online to believe the virus was overblown, maybe even a hoax. So no masks for them. Then they got sick. She died. A college lecturer had trouble refilling her lupus drug after the president promoted it as a treatment for the new disease. A hospital nurse broke down when an ICU patient insisted his illness was nothing worse than the flu, oblivious to the silence in beds next door.
Lies infected America in 2020. The very worst were not just damaging, but deadly.
President Donald J. Trump fueled confusion and conspiracies from the earliest days of the coronavirus pandemic. He embraced theories that COVID-19 accounted for only a small fraction of the thousands upon thousands of deaths. He undermined public health guidance for wearing masks and cast Dr. Anthony Fauci as an unreliable flip-flopper.
But the infodemic was not the work of a single person.
Anonymous bad actors offered up junk science. Online skeptics made bogus accusations that hospitals padded their coronavirus case numbers to generate bonus payments. Influential TV and radio opinion hosts told millions of viewers that social distancing was a joke and that states had all of the personal protective equipment they needed (when they didn’t).
It was a symphony of counter narrative, and Trump was the conductor, if not the composer. The message: The threat to your health was overhyped to hurt the political fortunes of the president.
Every year, PolitiFact editors review the year’s most inaccurate statements to elevate one as the Lie of the Year. The “award” goes to a statement, or a collection of claims, that prove to be of substantive consequence in undermining reality.
It has become harder and harder to choose when cynical pundits and politicians don’t pay much of a price for saying things that aren’t true. For the past month, unproven claims of massive election fraud have tested democratic institutions and certainly qualify as historic and dangerously bald-faced. Fortunately, the constitutional foundations that undergird American democracy are holding.
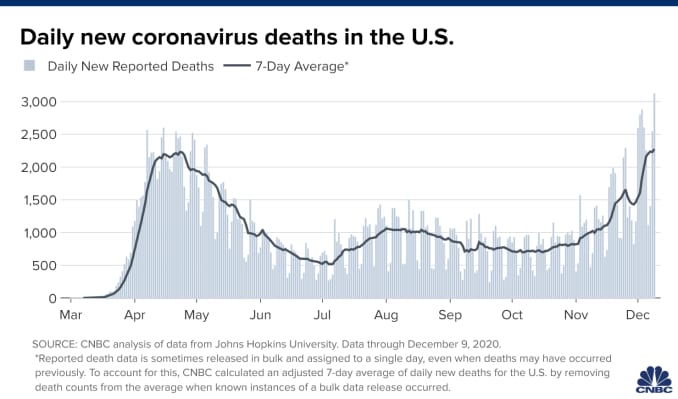
Meanwhile, the coronavirus has killed more than 300,000 in the United States, a crisis exacerbated by the reckless spread of falsehoods.
PolitiFact’s 2020 Lie of the Year: claims that deny, downplay or disinform about COVID-19.
‘I always wanted to play it down’
On Feb. 7, Trump leveled with book author Bob Woodward about the dangers of the new virus that was spreading across the world, originating in central China. He told the legendary reporter that the virus was airborne, tricky and “more deadly than even your strenuous flus.”
Trump told the public something else. On Feb. 26, the president appeared with his coronavirus task force in the crowded White House briefing room. A reporter asked if he was telling healthy Americans not to change their behavior.
“Wash your hands, stay clean. You don’t have to necessarily grab every handrail unless you have to,” he said, the room chuckling. “I mean, view this the same as the flu.”
Three weeks later, March 19, he acknowledged to Woodward: “To be honest with you, I wanted to always play it down. I still like playing it down. Because I don’t want to create a panic.”
His acolytes in politics and the media were on the same page. Rush Limbaugh told his audience of about 15 million on Feb. 24 that coronavirus was being weaponized against Trump when it was just “the common cold, folks.” That’s wrong — even in the early weeks, it was clear the virus had a higher fatality rate than the common cold, with worse potential side effects, too.
As the virus was spreading, so was the message to downplay it.
“There are lots of sources of misinformation, and there are lots of elected officials besides Trump that have not taken the virus seriously or promoted misinformation,” said Brendan Nyhan, a government professor at Dartmouth College. “It’s not solely a Trump story — and it’s important to not take everyone else’s role out of the narrative.”
Hijacking the numbers
In August, there was a growing movement on Twitter to question the disproportionately high U.S. COVID-19 death toll.
The skeptics cited Centers for Disease Control and Prevention data to claim that only 6% of COVID-19 deaths could actually be attributed to the virus. On Aug. 24, BlazeTV host Steve Deace amplified it on Facebook.
“Here’s the percentage of people who died OF or FROM Covid with no underlying comorbidity,” he said to his 120,000 followers. “According to CDC, that is just 6% of the deaths WITH Covid so far.”
That misrepresented the reality of coronavirus deaths. The CDC had always said people with underlying health problems — comorbidities — were most vulnerable if they caught COVID-19. The report was noting that 6% died even without being at obvious risk.
But for those skeptical of COVID-19, the narrative confirmed their beliefs. Facebook users copied and pasted language from influencers like Amiri King, who had 2.2 million Facebook followers before he was banned. The Gateway Pundit called it a “SHOCK REPORT.”
“I saw a statistic come out the other day, talking about only 6% of the people actually died from COVID, which is very interesting — that they died from other reasons,” Trump told Fox News host Laura Ingraham on Sept. 1.
Fauci, director of the National Institute of Allergy and Infectious Diseases, addressed the claim on “Good Morning America” the same day.
“The point that the CDC was trying to make was that a certain percentage of them had nothing else but just COVID,” he said. “That does not mean that someone who has hypertension or diabetes who dies of COVID didn’t die of COVID-19 — they did.”
Trump retweeted the message from an account that sported the slogans and symbols of QAnon, a conspiracy movement that claims Democrats and Hollywood elites are members of an underground pedophilia ring.
False information moved between social media, Trump and TV, creating its own feedback loop.
“It’s an echo effect of sorts, where Donald Trump is certainly looking for information that resonates with his audiences and that supports his political objectives. And his audiences are looking to be amplified, so they’re incentivized to get him their information,” said Kate Starbird, an associate professor and misinformation expert at the University of Washington.Weakening the armor: misleading on masks
At the start of the pandemic, the CDC told healthy people not to wear masks, saying they were needed for health care providers on the frontlines. But on April 3 the agency changed its guidelines, saying every American should wear non-medical cloth masks in public.
Trump announced the CDC’s guidance, then gutted it.
“So it’s voluntary. You don’t have to do it. They suggested for a period of time, but this is voluntary,” Trump said at a press briefing. “I don’t think I’m going to be doing it.”
Rather than an advance in best practices on coronavirus prevention, face masks turned into a dividing line between Trump’s political calculations and his decision-making as president. Americans didn’t see Trump wearing a mask until a July visit to Walter Reed National Military Medical Center.
Meanwhile, disinformers flooded the internet with wild claims: Masks reduced oxygen. Masks trapped fungus. Masks trapped coronavirus. Masks just didn’t work.
In September, the CDC reported a correlation between people who went to bars and restaurants, where masks can’t consistently be worn, and positive COVID-19 test results. Bloggers and skeptical news outlets countered with a misleading report about masks.
On Oct. 13, the story landed on Fox News’ flagship show, “Tucker Carlson Tonight.” During the show, Carlson claimed “almost everyone — 85% — who got the coronavirus in July was wearing a mask.”
“So clearly (wearing a mask) doesn’t work the way they tell us it works,” Carlson said.
That’s wrong, and it misrepresented a small sample of people who tested positive. Public health officials and infectious disease experts have been consistent since April in saying that face masks are among the best ways to prevent the spread of COVID-19.
But two days later, Trump repeated the 85% stat during a rally and at a town hall with NBC’s Savannah Guthrie.
“I tell people, wear masks,” he said at the town hall. “But just the other day, they came out with a statement that 85% of the people that wear masks catch it.”
The assault on hospitals
On March 24, registered nurse Melissa Steiner worked her first shift in the new COVID-19 ICU of her southeast Michigan hospital. After her 13-hour day caring for two critically ill patients on ventilators, she posted a tearful video.
“Honestly, guys, it felt like I was working in a war zone,” Steiner said. “(I was) completely isolated from my team members, limited resources, limited supplies, limited responses from physicians because they’re just as overwhelmed.”
“I’m already breaking, so for f—’s sake, people, please take this seriously. This is so bad.”
Steiner’s post was one of many emotional pleas offered by overwhelmed hospital workers last spring urging people to take the threat seriously. The denialists mounted a counter offensive.
On March 28, Todd Starnes, a conservative radio host and commentator, tweeted a video from outside Brooklyn Hospital Center. There were few people or cars in sight.
“This is the ‘war zone’ outside the hospital in my Brooklyn neighborhood,” Starnes said sarcastically. The video racked up more than 1.5 million views.
Starnes’ video was one of the first examples of #FilmYourHospital, a conspiratorial social media trend that pushed back on the idea that hospitals had been strained by a rapid influx of coronavirus patients.

Several internet personalities asked people to go out and shoot their own videos. The result: a series of user-generated clips taken outside hospitals, where the response to the pandemic was not easily seen. Over the course of a week, #FilmYourHospital videos were uploaded to YouTube and posted tens of thousands of times on Twitter and Facebook.
Nearly two weeks and more than 10,000 deaths later, Fox News featured a guest who opened a new misinformation assault on hospitals.
Dr. Scott Jensen, a Minnesota physician and Republican state senator, told Ingraham that, because hospitals were receiving more money for COVID-19 patients on Medicare — a result of a coronavirus stimulus bill — they were overcounting COVID-19 cases. He had no proof of fraud, but the cynical story took off.
Trump used the false report on the campaign trail to continue to minimize the death toll.
“Our doctors get more money if somebody dies from COVID,” Trump told supporters at a rally in Waterford, Mich., Oct. 30. “You know that, right? I mean, our doctors are very smart people. So what they do is they say, ‘I’m sorry, but, you know, everybody dies of COVID.’”
The real fake news: The Plandemic
The most viral disinformation of the pandemic was styled to look like it had the blessing of people Americans trust: scientists and doctors.
In a 26-minute video called “Plandemic: The Hidden Agenda Behind COVID-19,” a former scientist at the National Cancer Institute claimed that the virus was manipulated in a lab, hydroxychloroquine is effective against coronaviruses, and face masks make people sick.
Judy Mikovits’ conspiracies received more than 8 million views in May thanks in part to the online outrage machine — anti-vaccine activists, anti-lockdown groups and QAnon supporters — that push disinformation into the mainstream. The video was circulated in a coordinated effort to promote Mikovits’ book release.
A couple of months later, a similar effort propelled another video of fact-averse doctors to millions of people in only a few hours.
On July 27, Breitbart published a clip of a press conference hosted by a group called America’s Frontline Doctors in front of the U.S. Supreme Court. Looking authoritative in white lab coats, these doctors discouraged mask wearing and falsely said there was already a cure in hydroxychloroquine, a drug used to treat rheumatoid arthritis and lupus.
Trump, who had been talking up the drug since March and claimed to be taking it himself as a preventive measure in May, retweeted clips of the event before Twitter removed them as misinformation about COVID-19. He defended the “very respected doctors” in a July 28 press conference.
When Olga Lucia Torres, a lecturer at Columbia University, heard Trump touting the drug in March, she knew it didn’t bode well for her own prescription. Sure enough, the misinformation led to a run on hydroxychloroquine, creating a shortage for Americans like her who needed the drug for chronic conditions.
A lupus patient, she went to her local pharmacy to request a 90-day supply of the medication. But she was told they were only granting partial refills. It took her three weeks to get her medication through the mail.
“What about all the people who were silenced and just lost access to their staple medication because people ran to their doctors and begged to take it?” Torres said.No sickbed conversion
On Sept. 26, Trump hosted a Rose Garden ceremony to announce his nominee to replace the late Ruth Bader Ginsburg on the U.S. Supreme Court. More than 150 people attended the event introducing Amy Coney Barrett. Few wore masks, and the chairs weren’t spaced out.
In the weeks after, more than two dozen people close to Trump and the White House became infected with COVID-19. Early Oct. 2, Trump announced his positive test.
Those hoping the experience and Trump’s successful treatment at Walter Reed might inform his view of the coronavirus were disappointed.
Trump snapped back into minimizing the threat during his first moments back at the White House. He yanked off his mask and recorded a video.
“Don’t let it dominate you. Don’t be afraid of it,” he said, describing experimental and out-of-reach therapies he received. “You’re going to beat it.”
In Trump’s telling, his hospitalization was not the product of poor judgment about large gatherings like the Rose Garden event, but the consequence of leading with bravery. Plus, now, he claimed, he was immune from the virus.
On the morning after he returned from Walter Reed, Trump tweeted a seasonal flu death count of 100,000 lives and added that COVID-19 was “far less lethal” for most populations. More false claims at odds with data — the U.S. average for flu deaths over the past decade is 36,000, and experts said COVID-19 is more deadly for each age group over 30.
When Trump left the hospital, the U.S. death toll from COVID-19 was more than 200,000. Today it is more than 300,000. Meanwhile, this month the president has gone ahead with a series of indoor holiday parties.
The vaccine war
The vaccine disinformation campaign started in the spring but is still underway.
In April, blogs and social media users falsely claimed Democrats and powerful figures like Bill Gates wanted to use microchips to track which Americans had been vaccinated for the coronavirus. Now, false claims are taking aim at vaccines developed by Pfizer and BioNTech and other companies.
- A blogger claimed Pfizer’s head of research said the coronavirus vaccine could cause female infertility. That’s false.
- An alternative health website wrote that the vaccine could cause an array of life-threatening side effects, and that the FDA knew about it. The list included all possible — not confirmed— side effects.
- Social media users speculated that the federal government would force Americans to receive the vaccine. Neither Trump nor President-elect Joe Biden has advocated for that, and the federal government doesn’t have the power to mandate vaccines, anyway.
As is often the case with disinformation, the strategy is to deliver it with a charade of certainty.
“People are anxious and scared right now,” said Dr. Seema Yasmin, director of research and education programs at the Stanford Health Communication Initiative. “They’re looking for a whole picture.”
Most polls have shown far from universal acceptance of vaccines, with only 50% to 70% of respondents willing to take the vaccine. Black and Hispanic Americans are even less likely to take it so far.
Meanwhile, the future course of the coronavirus in the U.S. depends on whether Americans take public health guidance to heart. The Institute for Health Metrics and Evaluation projected that, without mask mandates or a rapid vaccine rollout, the death toll could rise to more than 500,000 by April 2021.
“How can we come to terms with all that when people are living in separate informational realities?” Starbird said.