Medicaid is critical to our nation’s healthcare system, providing necessary care for more than 72 million Americans – including our neighbors and friends.
Who it Affects
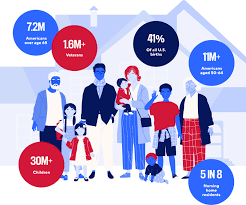
Medicaid covers children, seniors in nursing homes, veterans, people with long-term chronic illnesses, those with mental health issues and working families.
The program helps keep Americans healthy at all stages of life, providing healthcare to families in need — especially as the country continues to recover from record-high inflation.
The Problem
Some policymakers are considering Medicaid cuts that would undermine coverage for countless patients and threaten Americans’ access to comprehensive, 24/7 hospital care.
Medicaid covers health services for patients who otherwise wouldn’t be able to pay for care. Coverage of services is essential for hospitals, and helps ensure all Americans have access to high-quality, 24/7 care, no matter where they live.
Who Medicaid covers
Providing Lifesaving Healthcare Services
Medicaid covers patients with complex and chronic illnesses in need of long-term care, as well as emergency services and prescription coverage.
As the nation faces a growing mental health crisis, Medicaid also ensures millions of Americans — including veterans — have access to mental healthcare and substance abuse services.
Without access to affordable mental healthcare through Medicaid, veterans often lack the long-term support they deserve, and are left to deal with complex health issues years after their service.
In these areas, where primary care providers are few and far between, hospitals become even more vital sites of care — and in some cases, the only sites of care available.
Rural hospitals, already more likely to be at risk of closure, rely on Medicaid funding to stay open and to continue providing lifesaving care to their patients. Nearly 150 rural hospitals have closed or converted since 2010 alone. Further cuts to care would eliminate a lifeline for Americans across the country — with devastating consequences for rural communities.
The Solution
Cuts to Medicaid funding will create irreparable harm for our nation’s most vulnerable communities, including millions of children, veterans, those with chronic illnesses, seniors in nursing homes, and working families. Medicaid helps provide security to these Americans, keeping them healthy at every stage of life.
Congress should vote against efforts to reduce Medicaid funding and instead focus on policies that strengthen access to 24/7 care, rather than take it away.
Assaults against health care workers are costing hospitals upward of $18 billion a year in added security, training, workers compensation and other expenses, including treating victims, according to a new industry report.
Why it matters:
Attacks by patients and visitors in hospitals and clinics already were a problem before the pandemic and got worse with backlash against public health measures.
The American Hospital Association says there’s a human toll beyond the financial burden, with burnout, staff turnover, legal concerns and negative public perceptions all plaguing health systems.
By the numbers:
The University of Washington report for the trade group found prevention measures like active shooter training, hiring more security and reinforcing entry points and creating designated safe areas cost health systems $3.6 billion a year.
The cost of care for fatal and nonfatal injuries, lost productivity and replacing damaged equipment and infrastructure total about $14.6 billion a year. Health expenses for treating injuries alone account for more than $13 billion of that amount.
Between the lines:
Violent incidents most often occur in psychiatric units, emergency departments, waiting rooms and geriatric units, with rural areas having higher prevalence than urban areas, the report found.
Registered nurses, nursing assistants and patient care assistants experience particularly high rates of workplace violence. A 2024 American Hospital Association poll found half of U.S. nurses reported being either verbally abused, physically assaulted or both by a patient or a patient’s family member within the previous two years.
What we’re watching:
Congress is again considering legislation that would make assaulting hospital staff a federal crime, similar to protections for flight crews and airport workers.
The CBO projects that 10.9 million more people would be uninsured under President Trump’s sweeping budget bill — mostly from the way it would overhaul Medicaid, including new work requirements.
Why it matters:
That would amount to major coverage losses that are certain to fuel Democratic attacks on the measure, and put new pressure on vulnerable Republicans heading into the midterm election cycle, Peter Sullivan wrote first on Pro.
By the numbers:
The CBO on Wednesday projected that 7.8 million more people would be uninsured due to the Medicaid changes, with the rest likely due to Affordable Care Act marketplace changes, including new barriers to signing up that are aimed at fighting fraud.
The estimate includes 1.4 million people without verified citizenship “or satisfactory immigration status,” a reference to undocumented immigrants that some states opt to cover with non-federal dollars in their Medicaid programs.
The CBO was responding to a request from congressional Democrats about the number of uninsured people stemming from the package the House passed last month.
Republicans say the changes would ensure that Medicaid is targeted at beneficiaries deserving of coverage, and that taxpayer money should not be spent on healthy adults who are choosing not to work.
Opponents say people who are working will be caught up in the red tape from the changes and could still lose coverage.
The CBO also said another 5.1 million would become uninsured if Congress opts to let Affordable Care Act premium tax credit subsidies expire next year.
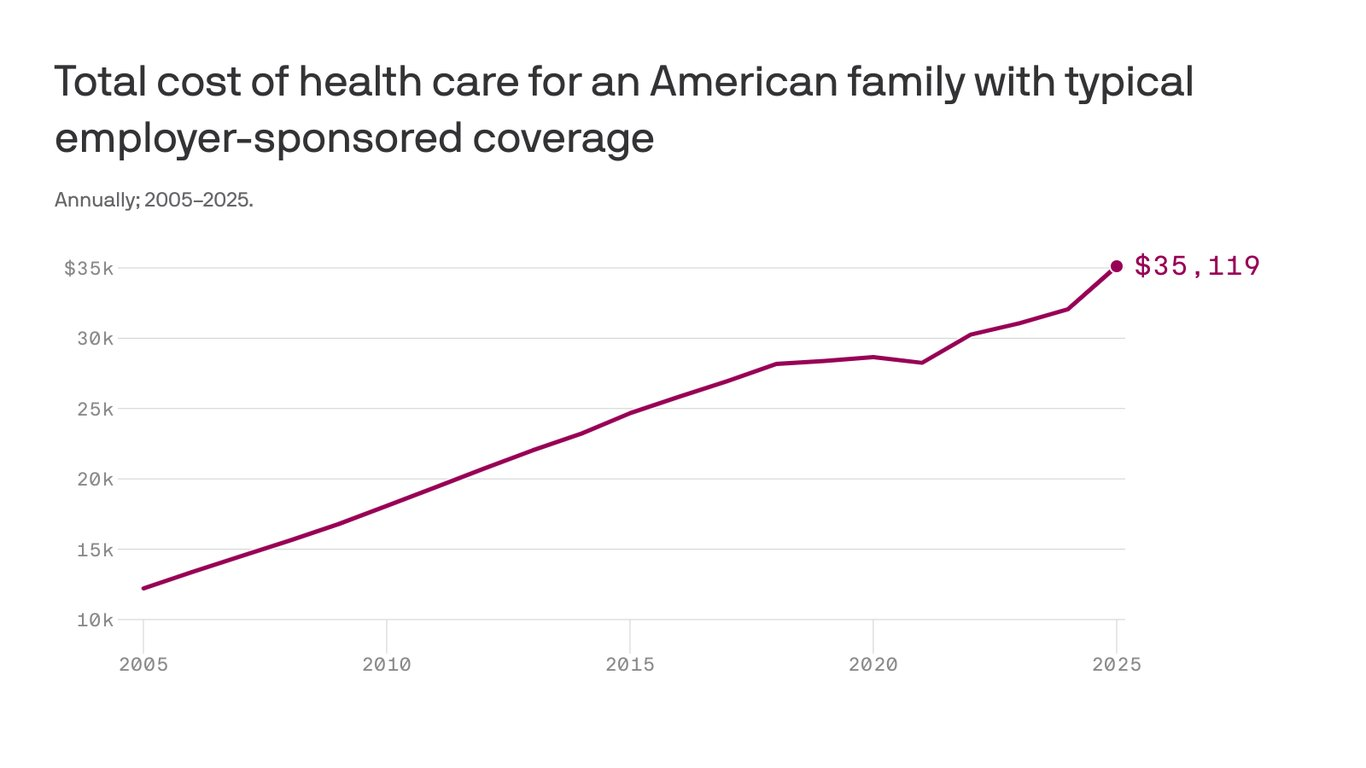
The cost to cover a family of four through workplace insurance now exceeds $35,000, nearly triple what it cost 20 years ago as annual growth in health costs have far outpaced wages.
The big picture:
Growing pharmacy and outpatient facility costs drove most of the increase, which includes employee and employer shares,according to the 2025 Milliman Medical Index.
Employers have been wary of passing health cost hikes to workers in a tight labor market, but the rising demand for costly care may force a reckoning.
State of play:
The $35,119 annual cost to cover a hypothetical family of four this year factors in drug costs, inpatient and outpatient care, and professional services, along with an “other” category that includes home health, ambulance transport, medical equipment and prosthetics.
A year of health care cost a family of four $12,214 in 2005, the year Milliman launched the index. The 20-year cumulative gain of 188% outpaced the 84% growth in wages over the same time.
Health costs have increased about 6% per year on average over the past two decades, according to Milliman, compared with an average inflation rate of 2.5% over that time.
Between the lines:
Employers in 2025 still shoulder 58% of employee health care costs, but their share has shrunk since 2005, when it was more than 60%.
Reality check:
Health care costs vary significantly by age, geography and pharmacy rebate arrangements.
Milliman calculates family cost based on a family with a 47-year-old male, 37-year-old female, and children ages 4 and under 1.
This was a “mathematically average” family in 2005, and Milliman continues to use that formula to keep data comparable year-to-year.
The firm has an online tool that allows readers to input other family configurations to see their estimated 2025 health care costs.
The analysis is based on Milliman’s proprietary research tools and analyzes commercialclaims data. The family cost figure reflects nationwide average negotiated provider fees and average PPO benefit levels.
The GOP’s reconciliation bill, the “One Big Beautiful Bill Act” (yes, it’s actually called that), is a cruel exercise in slashing benefits for the poor, the elderly, and the sick to free up fiscal space for yet more tax cuts for the rich. Compounding the harm, these benefit cuts are nowhere near enough to pay for the bill’s tax cuts for the wealthy.
Central to this effort are massive cuts to Medicaid and the Affordable Care Act (ACA) marketplaces that, as I argued in my recent paper, will exacerbate our ongoing medical debt crisis.
The GOP reconciliation package that the Senate and House recently agreed to instructed the House Energy and Commerce Committee, which oversees spending on health-care programs including Medicaid and the Children’s Health Insurance Program (CHIP), to identify up to $880 billion in savings over the next 10 years.
Under the rules of the budget reconciliation process, Republicans need to offset any tax cuts they wish to make permanent with an equal dollar value in cuts to spending so as to remain deficit neutral. Trillions of dollars in tax cuts for the wealthier therefore necessitate trillions of dollars in cuts to spending that fall mostly on the social safety net.
Although they did not quite reach that target, the committee still returned a proposed package of deep cuts and changes to Medicaid and to the ACA marketplaces that would reduce federal medical spending by at least $715 billion over 10 years, with about $625 billion in reduced Medicaid spending.1
After public backlash, Republicans seem to have backed off some of their most radical plans for Medicaid (at least for now—one of the challenges of taking health care from people is that it’s terrible politics, so the precise details of the cuts are likely to remain a moving target until the bill passes).
But all options they are close to settling on would still do horrific damage to the well-being of working-class families.
This includes requiring all Medicaid recipients above the federal poverty line to “cost share” by paying (larger) premiums and copayments,2 cutting federal matching to states that provide public health insurance coverage to undocumented and perhaps documented immigrants (on their own dime), and imposing harsh work requirements on “able-bodied adults without dependent children.” This latter provision will cut federal Medicaid spending by roughly $300 billion over 10 years even though the vast majority (92 percent) of nondisabled, non-elderly adult Medicaid recipients are already working, studying full time, or serving as caregivers. This is because work requirements create burdensome reporting requirements to demonstrate compliance that will cause Medicaid recipients who are already employed to lose their insurance as well—blaming the victim for losing their health care, in essence.
The Congressional Budget Office estimates that the reconciliation bill would decrease Medicaid enrollment by 10.3 million in 2034(the end of the reconciliation bill budget window).
According to this same analysis, most of these individuals would not obtain other insurance (e.g., through an employer) and would thus become uninsured.
When combined with the bill’s changes to the ACA marketplace and the expiration of the enhanced premium tax credits—a wildly successful policy that was introduced as part of the American Rescue Plan Act (ARPA) and one that Republicans have shown no inclination to extend—this would result in an additional 13.7 million uninsured individuals in 2034, a 30 percent increase, according to KFF estimates.
Republicans seem hell-bent on undoing the remarkable progress made in the 15 years since the passage of the ACA in reducing the non-elderly uninsured rate from 17.8 percent in 2010 to roughly 9.5 percent today (plus ça change).
But we’ve seen less focus on how this will affect the problem of underinsurance.
Republicans’ Medicaid cost-sharing requirements, the changes they have proposed to the ACA marketplaces, and their determination to let the ARPA premium tax credit enhancements expire will also worsen the problem of underinsurance, an area where we have made considerably less progress.
Taken together, this will worsen the ongoing medical crisis because medical debt is driven by uninsurance and underinsurance.
Medical debt is, unlike in most other countries, and despite the successes of the ACA, a major problem in the United States. KFF found that 20 million adults (almost 1 in 12) owed “significant” medical debt to a health-care provider.3 This number rises when we consider a more expansive definition of medical debt including credit card balances and bank loans used to pay medical providers. Under that definition, an estimated 41 percent of American adults (~107 million people) carried some form of medical debt and 24 percent of American adults (~62 million people) had medical debt that was past due or that they were unable to pay. Among those with medical debt using this more expansive definition, nearly half (44 percent) reported owing at least $2,500, and about one in eight (12 percent) said they owe $10,000 or more. The poor, the sick, the middle-aged, and Black and Hispanic individuals disproportionately bear the brunt of this problem.
The crisis of medical debt and underinsurance is so widely recognized by Americans that a state attorney general candidate can go viral just by talking about the reality of a GoFundMe health-care system millions of Americans face.
The consequences of all this debt are dire—and reflect a health-care system that heals people physically but leaves many permanently scared financially. In 2022, medical debt (using the narrow definition) made up an estimated 58 percent of all debts that had gone to collections, and 62 percent of bankruptcies were attributed in part to medical debt. Medical debt also damages credit scores, leading to a wide variety of negative impacts on financial well-being that can follow families for years.
A poor credit score means that families may be unable to obtain a mortgage or a car loan or may end up paying much higher interest rates.
Credit scores are commonly used by landlords to screen tenants and by employers as part of a background check during the hiring process. Even for those who manage to maintain their credit after taking on medical debt, there are real costs. For those with limited income and assets, debt service may displace spending on food, clothing, and other essentials, leading to material hardship. It can make savings impossible and limit economic mobility.
Medical debt is a problem largely generated by poor policy decisions including, as I argue in my paper, prioritizing and incentivizing health insurance coverage through the private market rather than through Medicaid and Medicare, which offer comprehensive coverage more cheaply. The problem would rapidly disappear if we could extend comprehensive health insurance coverage to the millions of uninsured and underinsured people who live with the constant risk that a sudden medical event could ruin their finances and constrain their futures.
But rather than fix the problem, the GOP plans to throw millions off Medicaid and saddle those who remain with higher costs and more limited coverage. The results of these poor policy decisions will be more sickness, more debt, and higher costs for everyone in exchange for on-paper “savings.” And all this in service of tax cuts for the wealthy they haven’t even bothered to justify.
If you ask Eleanor
“If the old people cannot afford their medical care under their own Social Security allowances, then the burden is going to fall on their children who are in their earning years. This will mean that just at the time when these children who may be having young children of their own and needing medical care, a young couple will also have to consider shouldering the burden for parents as well. This is not fair, and leads to both the children and the older people not getting full coverage, since both will try to shave a little off their needs in order not to make the burden impossible to carry.”
In chaos theory, there’s a concept known as the butterfly effect—the idea that a seemingly small action, occurring at just the right moment, can trigger ripple effects that grow across time and space. A butterfly flaps its wings in Brazil, the saying goes, and a tornado forms weeks later in Texas.
Presidential decisions can carry the same weight, especially those made in the first 100 days of a new administration. Time and again, these early choices unleash far-reaching consequences that reshape a nation.
As Donald Trump wraps up the opening stretch of his second term, his healthcare-focused executive actions underscore the consequentiality of this early window. And when compared with Barack Obama’s approach in 2009 (the last time a president pursued major healthcare reforms right out of the gate), the contrast becomes even more striking.
Two presidents. Two defining moments. And one fundamental question that both men had to answer in the first 100 days: Where should healthcare reform begin — by expanding coverage, improving quality or cutting costs?
Crisis, Control And A Key Healthcare Choice
The idea that a president’s first 100 days matter dates back to Franklin D. Roosevelt. In 1933, during the depths of the Great Depression, FDR passed a wave of New Deal reforms that redefined the role of government in American life.
Ever since, the opening months of a new presidency have served as both proving ground and preview. They reveal how a president intends to govern and what he values most.
For both presidents Obama and Trump, their answer to the healthcare question — where to begin? — would shape what followed. Obama chose to expand coverage. Trump has chosen to cut costs. Those decisions set them on opposing paths. And with every subsequent policy decision, the gap between their contrasting approaches only grows.
’09 Obama: Health Coverage And Congressional Action
In the quiet calculus of early governance, President Obama concluded that without health insurance coverage, access to high-quality medical care would remain out of reach for tens of millions of Americans.
Confronting a system that left 60 million uninsured, he believed that expanding access to coverage was a vital first step — not only to improve individual health outcomes, but to create a healthier nation that ultimately would require less medical care (and spending) overall.
That belief was grounded in lived experience: his mother’s battle with cancer and the insurance disputes that followed, as well as his years as a community organizer working with families who couldn’t afford medical care.
He also understood that only Congressional legislation — rather than executive action — would make those gains durable. So, in his first 100 days, he pursued a strategy grounded in consensus-building. He convened healthcare stakeholders, hosted public healthcare summits, expanded the Children’s Health Insurance Program (CHIP) and proposed a federal budget that included a $634 billion “down payment” on healthcare reform.
’25 Trump: Cost Cutting And Executive Control
Donald Trump didn’t ease into his second term. He charged in, pen in hand. His priorities for the country were clear: cut taxes, impose tariffs and reduce federal spending.
For Trump, speed was of the essence. So, he bypassed Congress in favor of executive orders, downsizing healthcare agencies and dismantling regulatory oversight wherever possible.
At the center of Trump’s domestic agenda is an ambitious income tax overhaul, dubbed the “big beautiful bill.” But passing it will require support from fiscal conservatives in his own party. To offset the steep drop in tax revenue, Trump has signaled a willingness to slash federal spending, starting with healthcare programs.
What Comes Next: Mapping Health Policy Consequences
Presidents make thousands of decisions over the course of a four-year term, but those made in the first few months typically matter most. Both Obama and Trump had to decide whether to prioritize expanding coverage or cutting costs, and that choice would shape the steps that follow.
For Obama, the consequences of his choice were sweeping. His early focus on increasing health insurance coverage laid the foundation for the Affordable Care Act, the most ambitious healthcare reform since Medicare and Medicaid in the 1960s. The ACA provided affordable insurance to more than 30 million Americans, offered subsidies to low- and middle-income families, cut the uninsured rate in half and guaranteed protections for those with preexisting conditions. The law survived political opposition, legal challenges and subsequent presidencies.
Trump’s early decisions are reshaping healthcare, too, but in ways that reflect a very different set of priorities and a sharply contrasting vision for the federal government’s role.
1. Cost-Driven Actions: Reducing Government Healthcare Spending
Guided by a business-oriented focus on cost containment, Trump has sought to reduce the federal government’s role in healthcare through sweeping budget and staffing changes. Among the most significant:
Agency layoffs: The Department of Health and Human Services has initiated mass layoffs across the CDC, NIH and FDA, reducing staff capacity by 20,000 and cutting critical programs, including HIV research grants and initiatives targeting autism, chronic disease, teen pregnancy and substance abuse.
ACA support rollbacks: The administration slashed funding for ACA navigators and rescinded extended enrollment periods, making it more difficult for individuals (especially low-income Americans) to obtain coverage.
Planned Parenthood and family planning cuts: Freezing Title X funds has reduced access to reproductive healthcare in multiple states.
Medicaid at risk: A proposed $880 billion reduction over 10 years could eliminate expanded Medicaid coverage in many states. Additional moves (like work requirements or application hurdles) would likely reduce enrollment further.
2. Cultural And Executive Power Moves: Redefining Government’s Role In Health
While cutting costs has been the central goal, many of Trump’s actions reflect a broader ideological stance. He’s using executive authority to reshape the values, norms and institutions that have defined American healthcare. These include:
Withdrawal from the World Health Organization (WHO): The administration formally ended U.S. participation, citing concerns about funding and governance.
Restructuring USAID’s health portfolio: Multiple contracts and programs related to maternal health, infectious disease prevention and international public health have been ended or scaled back.
Policy changes on federal language and research topics: Executive directives have modified how agencies are allowed to address topics related to gender and sexuality, leading to the removal of LGBTQ+ content from health resources and websites.
Reorganization of DEI programs: Diversity, equity and inclusion initiatives have been rolled back or eliminated across several federal departments.
The Likely Consequences Of Trump’s First 100 Days
President Trump’s early actions reveal two defining trends: cutting government healthcare spending and reshaping federal priorities through executive authority. Both are already changing how care is accessed, funded and delivered. And both are likely to produce lasting consequences.
The most immediate impact will come from efforts to reduce healthcare spending. Cuts to Medicaid, ACA enrollment support and family planning programs are expected to lower insurance enrollment, particularly among low-income families, young adults and people with chronic illness.
As coverage declines, care becomes harder to access and more expensive when it’s needed. The results: delayed diagnoses, avoidable complications and rising levels of uncompensated care.
His second set of actions — including reduced investment in federal science agencies — will slow drug development and weaken the infrastructure needed to respond to future public health threats.
Meanwhile, a more constrained and domestically focused healthcare agenda is likely to diminish trust in federal health agencies, limit access to culturally competent care and produce a loss of global leadership in health innovation.
The U.S. Constitution gives presidents broad power to chart the nation’s course. And the decisions made in their first 100 days shape the trajectory of an entire presidency.
One president decided to prioritize coverage, while a second chose cost-cutting. And like the flap of a butterfly’s wings, these early actions generate ripples — expanding in size over time and radically altering American healthcare, for better or worse.