In the era of great awakening, leaders have to step up and be conscious about building trust with people they work with.
The old rules and hierarchies, that were already becoming obsolete, have now been thrown out of the window. People look for integration of work and well-being knowing that work is what you do, not a place you go to.
Opportunities are abound and excellent people have ample choices (they always had). It is high time that organizations and leaders think this through carefully to first align their own mindset to this new reality and then take conscious actions to build teams, practices and processes that are not just high-performing but also have a strong fabric of trust woven in.
Employees, after all, are volunteers who exercise their choice of working with you. Effective leadership is about making it worth for them.
Building high-trust environment means putting the human back at the center of how a business functions and building everything – purpose, culture, processes, structures, rituals, systems, tools and mindsets – around it.
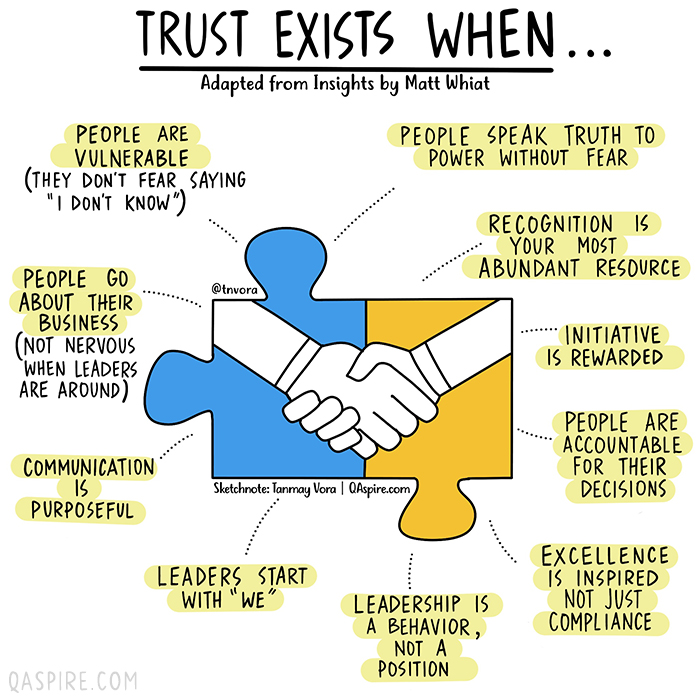
How would we know if we are working in an environment where we can trust others and that we are trusted? We can always answer this based on our intrinsic feeling but if you are a leader who is working hard to build trust, here are a few vital signs that you need to look for.
How much should we pay for drugs? That’s the question at the center of American Hospital Association v. Becerra, a sleeper of a case involving billions of dollars in federal spending and a chance to reshape two doctrines at the heart of administrative law.
Drugs, money, and the law: Sounds sexy, right? Still, you could be forgiven for never having heard of the case, which will be argued on Tuesday. It arises out of a technical dispute over how Medicare, the federal program that insures 63 million elderly and disabled people, pays for some of the drugs that hospitals dispense to patients in outpatient departments — in particular, chemotherapy drugs and other expensive anti-cancer medications.
The case centers on part of a 2003 law that gives Medicare two options for how to pay for those drugs. Under the first option, Medicare would survey hospitals about what it cost them to acquire the drugs. Medicare would then draw on the survey data and reimburse hospitals for their “average acquisition costs,” subject to variations for different types of hospitals. It’s a rough-cut way to make hospitals whole without requiring them to submit receipts for every drug purchase.
But Medicare immediately encountered a problem: It just wasn’t practical to survey hospitals about their acquisition costs. Fortunately, the law anticipated that possibility and gave Medicare a second option. In the absence of survey data, Medicare could pay the “average price” for the drug, “as calculated and adjusted by the Secretary [of Health and Human Services] as necessary for purposes of this [option].”
This approach turned out to be costly. A drug’s “average price” is fixed elsewhere in the Medicare statute, typically at 106% of the drug’s sale price. As a policy matter, this “average sales price plus 6%” approach is hard to defend. Because 6% of a large number is bigger than 6% of a small number, hospitals have an incentive to dispense more expensive drugs, even when there are cheaper and equally effective therapies.
Other developments soon made the payment policy look even more dubious. Back in 1992, Congress created something called the 340B program to support health-care providers that serve poor and disadvantaged communities. Eligible providers get steep discounts on the drugs that they purchase — anywhere between 20% and 50% of the normal price.
Initially, few hospitals qualified for the 340B program. Today, more than two-thirds of nonprofit hospitals participate. (For-profits are excluded from the program.) For years, Medicare kept paying those 340B hospitals 106% of the average sales price of their outpatient drugs. The upshot was that hospitals were buying highly discounted drugs and then charging the federal government full price. That heightened the incentive to prescribe very expensive medications — which is partly why Medicare spending on outpatient drugs has ballooned, growing an average of 8.1% per year from 2006 through 2017.
Federal regulators were troubled by the gap between hospital costs and Medicare payments. In their view, the point of the 2003 statute was to cover hospitals’ costs, not to subsidize 340B hospitals. That jibes with the Medicare statute more generally: Its “overriding purpose” is to provide “reasonable (not excessive or unwarranted) cost-based reimbursement.”
So Medicare adopted a rule that, starting in 2018, slashed the reimbursement rate for 340B hospitals’ outpatient drugs (or, more precisely, a subset of them) to 22.5% less than the average sales price. That was still generous, since on average the 340B discount is about one-third of a drug’s price. But it was much less generous than before, and Medicare estimated that the change would save taxpayers $1.6 billion every year.
The American Hospital Association, together with two hospital trade groups and three hospitals, filed suit. Had Medicare chosen option one, the plaintiffs argued, it could have focused on acquisition costs and even distinguished among hospital groups in setting payment rates. Instead, it chose option two, which says that Medicare must pay a drug’s “average price” — not its acquisition price — and doesn’t provide for discriminating between hospitals. While the plaintiffs acknowledged that Medicare could “adjust” the average price, they argued that a cut from 106% to 77.5% of the average sales price was not really an adjustment. It was a wholesale revision of the statutory scheme.
The plaintiffs encountered an obstacle right out of the gate. To prevent courts from second-guessing Medicare’s choices about how much to pay for outpatient care, the Medicare statute says that “[t]here shall be no administrative or judicial review” of those choices. In the government’s telling, Congress precluded review because Medicare has a fixed annual budget for outpatient care. Increasing payments for one type of care thus requires cutting payments for other types of care.
That linkage means that, if the plaintiffs win, it’s not just that they should have been paid more for certain drugs. It’s that all hospitals should have been paid less for other services. (That helps explains why coalitions representing rural and for-profit hospitals have filed amicus briefs in support of Medicare.) Unwinding that decision would be an administrative nightmare — which is why Congress precluded review in the first place.
As the plaintiffs see it, however, the government simply misreads the scope of the preclusion language. Though it generally precludes review of reimbursement decisions relating to outpatient care, it doesn’t cross-reference the subsection relating to outpatient drugs. Both the district court and the U.S. Court of Appeals for the District of Columbia Circuit agreed, invoking the strong presumption favoring judicial review of agency action.
On the merits, the plaintiffs fared less well. Though they won in the district court, the D.C. Circuit held that Medicare reasonably read the 2003 law to allow it to align hospital reimbursement with hospital acquisition costs. Medicare’s interpretation — and the scope of its authority to “adjust” payment rates — was thus owed deference under Chevron U.S.A. Inc. v. Natural Resources Defense Council, a 1984 decision holding that courts generally should defer to agencies’ reasonable interpretations of ambiguous statutes. Judge Cornelia Pillard dissented, arguing that the statute unambiguously foreclosed Medicare’s interpretation.
The plaintiffs asked the Supreme Court to review a single question: whether Medicare should receive Chevron deference for interpreting the 2003 law in the manner that it did. Tantalizingly, the plaintiffs noted that “[i]t is no secret that members of this Court have raised concerns about whether Chevron deference, particularly when applied as indiscriminately as it was in this case, violates the separation of powers.”
The Supreme Court bit. In its order granting certiorari, however, the court instructed the parties to brief an additional question: whether the Medicare statute precludes the lawsuit. What that means is that — in addition to resolving whether hospitals are entitled to billions of taxpayer dollars — the court will have the chance to address two foundational doctrines of administrative law: the presumption of reviewability and Chevron deference.
Arguably, AHA v. Becerraoffers an unusually vivid example of the costs of a strong presumption of reviewability. If the plaintiffs win, what’s the remedy? Is Medicare supposed to reopen every outpatient payment decision that it’s made since 2018, given that paying more for 340B drugs means it should have paid less for other services? The plaintiffs say no, arguing that Medicare wouldn’t be required to make any retroactive adjustments. But the government fears otherwise and the answer is not at all clear. Isn’t that the kind of mess that preclusion is meant to avoid?
I’ve called in my academic work for abandoning the presumption of reviewability precisely because it disrespects Congress’ reasonable desire to shield some administrative decisions from judicial review. In recent years, however, the Supreme Court has evinced no interest in doing so — the presumption of reviewability remains “strong.” We may soon find out just how strong it is.
But the big question about the case is whether the court will use it as a vehicle to reconsider Chevron deference. In the plaintiffs’ view, it is galling — “an affront to the separation of powers” — that the courts would defer when Medicare has exploited a purported ambiguity to sidestep Congress’ clear instructions about how much to pay hospitals. Several of the conservative justices, including in particular Justices Clarence Thomas and Neil Gorsuch, may be receptive to the argument. If so, the right wing of the court could use the case to narrow or even overturn Chevron, with potentially dramatic implications for the scope of executive-branch power.
Whether the court will do so is anyone’s guess. The justices could easily resolve the case on narrower grounds. Maybe the statute unambiguously forecloses Medicare’s interpretation of the law, as the plaintiffs argue. Or maybe, as the government claims, Medicare properly exercised its explicit authority to “adjust” prices for outpatient drugs.
Neither of those holdings would be the sexiest decision that the Supreme Court has ever issued. It would be technical, arcane — even boring. Given the financial stakes, however, it would be significant nonetheless.
The healthcare industry’s staffing shortage crisis has had clear consequences for care delivery and efficiency, forcing some health systems to pause nonemergency surgeries or temporarily close facilities. Less understood is how these shortages are affecting care quality and patient safety.
A mix of high COVID-19 patient volume and staff departures amid the pandemic has put hospitals at the heart of a national staffing shortage, but there is little national data available to quantify the shortages’ effects on patient care.
The first hint came last month from a CDC report that found healthcare-associated infections increased significantly in 2020 after years of steady decline. Researchers attributed the increase to challenges related to the pandemic, including staffing shortages and high patient volumes, which limited hospitals’ ability to follow standard infection control practices.
“That’s probably one of the first real pieces of data — from a large scale dataset — that we’ve seen that gives us some sense of direction of where we’ve been headed with the impact of patient outcomes as a result of the pandemic,” Patricia McGaffigan, RN, vice president of safety programs for the Institute for Healthcare Improvement, told Becker’s. “I think we’re still trying to absorb much of what’s really happening with the impact on patients and families.”
An opaque view into national safety trends
Because of lags in data reporting and analysis, the healthcare industry lacks clear insights into the pandemic’s effect on national safety trends.
National data on safety and quality — such as surveys of patient safety culture from the Agency for Healthcare Research and Quality — can often lag by several quarters to a year, according to Ms. McGaffigan.
“There [have been] some declines in some of those scores more recently, but it does take a little while to be able to capture those changes and be able to put those changes in perspective,” she said. “One number higher or lower doesn’t necessarily indicate a trend, but it is worth really evaluating really closely.”
For example, 569 sentinel events were reported to the Joint Commission in the first six months of 2021, compared to 437 for the first six months of 2020. However, meaningful conclusions about the events’ frequency and long-term trends cannot be drawn from the dataset, as fewer than 2 percent of all sentinel events are reported to the Joint Commission, the organization estimates.
“We may never have as much data as we want,” said Leah Binder, president and CEO of the Leapfrog Group. She said a main area of concern is CMS withholding certain data amid the pandemic. Previously, the agency has suppressed data for individual hospitals during local crises, but never on such a wide scale, according to Ms. Binder.
CMS collects and publishes quality data for more than 4,000 hospitals nationwide. The data is refreshed quarterly, with the next update scheduled for October. This update will include additional data for the fourth quarter of 2020.
“It is important to note that CMS provided a blanket extraordinary circumstances exception for Q1 and Q2 2020 data due to the COVID-19 pandemic where data was not required nor reported,” a CMS spokesperson told Becker’s. “In addition, some current hospital data will not be publicly available until about July 2022, while other data will not be available until January 2023 due to data exceptions, different measure reporting periods and the way in which CMS posts data.”
Hospitals that closely monitor their own datasets in more near-term windows may have a better grasp of patient safety trends at a local level. However, their ability to monitor, analyze and interpret that data largely depends on the resources available, Ms. McGaffigan said. The pandemic may have sidelined some of that work for hospitals, as clinical or safety leaders had to shift their priorities and day-to-day activities.
“There are many other things besides COVID-19 that can harm patients,” Ms. Binder told Becker’s. “Health systems know this well, but given the pandemic, have taken their attention off these issues. Infection control and quality issues are not attended to at the level of seriousness we need them to be.”
What health systems should keep an eye on
While the industry is still waiting for definitive answers on how staffing shortages have affected patient safety, Ms. Binder and Ms. McGaffigan highlighted a few areas of concern they are watching closely.
The first is the effect limited visitation policies have had on families — and more than just the emotional toll. Family members and caregivers are a critical player missing in healthcare safety, according to Ms. Binder.
When hospitals don’t allow visitors, loved ones aren’t able to contribute to care, such as ensuring proper medication administration or communication. Many nurses have said they previously relied a lot on family support and vigilance. The lack of extra monitoring may contribute to the increasing stress healthcare providers are facing and open the door for more medical errors.
Which leads Ms. Binder to her second concern — a culture that doesn’t always respect and prioritize nurses. The pandemic has underscored how vital nurses are, as they are present at every step of the care journey, she continued.
To promote optimal care, hospitals “need a vibrant, engaged and safe nurse workforce,” Ms. Binder said. “We don’t have that. We don’t have a culture that respects nurses.”
Diagnostic accuracy is another important area to watch, Ms. McGaffigan said. Diagnostic errors — such as missed or delayed diagnoses, or diagnoses that are not effectively communicated to the patient — were already one of the most sizable care quality challenges hospitals were facing prior to the pandemic.
“It’s a little bit hard to play out what that crystal ball is going to show, but it is in particular an area that I think would be very, very important to watch,” she said.
Another area to monitor closely is delayed care and its potential consequences for patient outcomes, according to Ms. McGaffigan. Many Americans haven’t kept up with preventive care or have had delays in accessing care. Such delays could not only worsen patients’ health conditions, but also disengage them and prevent them from seeking care when it is available.
Reinvigorating safety work: Where to start
Ms. McGaffigan suggests healthcare organizations looking to reinvigorate their safety work go back to the basics. Leaders should ensure they have a clear understanding of what their organization’s baseline safety metrics are and how their safety reports have been trending over the past year and a half.
“Look at the foundational aspects of what makes care safe and high-quality,” she said. “Those are very much linked to a lot of the systems, behaviors and practices that need to be prioritized by leaders and effectively translated within and across organizations and care teams.”
She recommended healthcare organizations take a total systems approach to their safety work, by focusing on the following four, interconnected pillars:
Culture, leadership and governance
Patient and family engagement
Learning systems
Workforce safety
For example, evidence shows workforce safety is an integral part of patient safety, but it’s not an area that’s systematically measured or evaluated, according to Ms. McGaffigan. Leaders should be aware of this connection and consider whether their patient safety reporting systems address workforce safety concerns or, instead, add on extra work and stress for their staff.
Safety performance can slip when team members get busy or burdensome work is added to their plates, according to Ms. McGaffigan. She said leaders should be able to identify and prioritize the essential value-added work that must go on at an organization to ensure patients and families will have safe passage through the healthcare system and that care teams are able to operate in the safest and healthiest work environments.
In short, leaders should ask themselves: “What is the burdensome work people are being asked to absorb and what are the essential elements that are associated with safety that you want and need people to be able to stay on top of,” she said.
To improve both staffing shortages and quality of care, health systems must bring nurses higher up in leadership and into C-suite roles, Ms. Binder said. Giving nurses more authority in hospital decisions will make everything safer. Seattle-based Virginia Mason Hospital recently redesigned its operations around nurse priorities and subsequently saw its quality and safety scores go up, according to Ms. Binder.
“If it’s a good place for a nurse to go, it’s a good place for a patient to go,” Ms. Binder said, noting that the national nursing shortage isn’t just a numbers game; it requires a large culture shift.
Hospitals need to double down on quality improvement efforts, Ms. Binder said. “Many have done the opposite, for good reason, because they are so focused on COVID-19. Because of that, quality improvement efforts have been reduced.”
Ms. Binder urged hospitals not to cut quality improvement staff, noting that this is an extraordinarily dangerous time for patients, and hospitals need all the help they can get monitoring safety. Hospitals shouldn’t start to believe the notion that somehow withdrawing focus on quality will save money or effort.
“It’s important that the American public knows that we are fighting for healthcare quality and safety — and we have to fight for it, we all do,” Ms. Binder concluded. “We all have to be vigilant.”
Conclusion
The true consequences of healthcare’s labor shortage on patient safety and care quality will become clear once more national data is available. If the CDC’s report on rising HAI rates is any harbinger of what’s to come, it’s clear that health systems must place renewed focus and energy on safety work — even during something as unprecedented as a pandemic.
The irony isn’t lost on Ms. Binder: Amid a crisis driven by infectious disease, U.S. hospitals are seeing higher rates of other infections.
“A patient dies once,” she concluded. “They can die from COVID-19 or C. diff. It isn’t enough to prevent one.”
The $1.7 trillion “social infrastructure” legislation passed by the House and now before the Senate would spur growth, expand employment and boost productivity with limited inflationary impact, according to Moody’s Investors Service.
The spending “would occur over 10 years, include significant revenue-raising offsets and would likely only start to flow into the economy later in 2022 at a time when inflationary pressures from disruptions to global supply chains and U.S. labor supply will likely have diminished,” Moody’s Vice President-Senior Analyst Rebecca Karnovitz said.
“Investments in childcare, education and workforce development have the potential to boost labor force participation and increase productivity over the medium and longer term,” she said. While the Senate will likely insist on amendments, the Build Back Better (BBB) bill currently would invest $555 billion in clean energy and “climate resilience” and $585 billion in childcare, universal prekindergarten and paid family leave.
Dive Insight:
CFOs concerned about rising prices and the risk of a wage-price spiral have found sympathy from some lawmakers who warn that the $5.7 trillion in spending Congress has already approved during the pandemic will further stoke inflation.
“Inflation is hammering working families across America,” Senate Minority Leader Mitch McConnell told the chamber last week. The Kentucky Republican called BBB a “socialist wish list” and an inflationary “taxing and spending spree.”
Some Democrats — including Sens. Kyrsten Sinema of Arizona and Joe Manchin of West Virginia — have cautioned that excessive spending could push up prices and worsen the fiscal outlook.
Sinema and Manchin have said that they want less costly legislation. With Democrats holding the smallest possible Senate majority, support from the two senators is essential for final passage of the bill.
“I have been concerned about high levels of spending that are not targeted or are not efficient and effective,” Sinema told the Washington Post on Nov. 18 while noting rising inflation.
“The threat posed by record inflation to the American people is not ‘transitory’ and is instead getting worse,” Manchin said on Twitter this month after the Labor Department reported that consumer prices rose 6.2% in October on an annual basis.
CFOs face even higher price gains for wholesale goods. The producer price index for final demand, a measure of what suppliers charge, soared 8.6% in October from the prior year, according to the Labor Department. That was a record jump in a series of data first published in 2010.
The Moody’s analysis suggests that concerns about the impact of BBB on inflation and the U.S. fiscal outlook may be overblown.
“We expect the spending package to have a limited impact on inflation,” Moody’s said.
Referring to the U.S. credit outlook, Moody’s said, “we expect the legislation to have only a small effect on the sovereign’s fiscal position, given that the spending would be spread over a decade and the revenue-raising measures would help offset the impact on federal budget deficits.”
The Congressional Budget Office estimates that the House version of BBB would push up fiscal deficits by $367 billion over a 10-year period.
Yet the estimate excludes about $200 billion in revenue that would come from a provision in the bill funding tougher tax enforcement and collection, Moody’s said.
“Estimates of the bill’s impact on the deficit are likely to shift in accordance with provisions that may be stripped from the Senate’s final version of the legislation,” according to Moody’s.