Cartoon – No New Year’s Resolutions for me this year

As was the case in 2018, the healthcare industry saw several megamergers occur in 2019.
Healthcare leaders pointed to industry consolidation as the year’s top priority, according to a Definitive Healthcare survey, with different reasons for pursuing mergers.
Related: Top 5 Healthcare Mergers of 2018
Providers sought to achieve scale in order to address staffing shortages while insurers looked to respond to the increasing influence of consumerism in healthcare.
While some mergers fell through, many organizations announced or finalized deals during the course of the year.
Below are six major healthcare mergers that were announced or completed in 2019.
The nearly $70 billion megamerger received final judicial approval in September after an extended review by U.S. District Judge Richard J. Leon.
The merger originally received approval from the Department of Justice in October 2018 but was subject to questions and criticisms by numerous stakeholders.
The deal was marked by scrutiny over vertical mergers, with Leon noting that his approval shouldn’t be seen as a rubber stamp.
Centene Corp. announced a $17.3 billion merger with WellCare Health Plans in March, a move seen as doubling down on the marketplaces established by the Affordable Care Act.
The merged company will be based in St. Louis and encompass 22 million members, $97 billion in revenues, and $5 billion in EBITDA for 2019.
The pending transaction has already received regulatory approval from 25 states.
Earlier this month, Centene agreed to sell its subsidiary IlliniCare Health to CVS Health, including its Medicaid and Medicare Advantage plans in Illinois.
Dignity Health and Catholic Health Initiatives finalized a $29 billion megamerger between the two Catholic health systems in February.
Renamed as “CommonSpirit,” the Chicago–based health system has a footprint in 21 states, with more than 700 care sites and 142 hospitals.
In November, the system released its Q1 2020 financials highlighted by $7.1 billion in revenues and a net loss of $227 million.
Harvard Pilgrim Health Care and Tufts Health Plan announced an intention to merge in August, potentially serving nearly 2.4 million plan members across New England.
As part of the proposed deal, Tufts CEO Tom Croswell would serve as CEO of the merged company while Harvard Pilgrim CEO Michael Carson would serve as president.
The two Massachusetts-based insurers told The Boston Globe earlier this month that the merger would benefit consumers with more affordable health coverage.
Total Health Care and Priority Health received final regulatory approval from the Michigan Department of Insurance and Financial Services (DIFS) in late November.
The two Michigan-based healthcare organizations, which announced plans to merge in late August, plan to complete the deal by the end of 2019.
Prior to receiving approval from state regulators, Total Health Care members approved the merger earlier this fall.
As part of the merger, the two Michigan-based healthcare organizations will also be establishing a $25 million foundation to improve health outcomes in Detroit.
Two New Hampshire-based health systems agreed to merge nine months after signing a letter of intent to merge.
The new merged system will be renamed “Dartmouth-Hitchcock Health GraniteOne” and includes Catholic Medical Center in Manchester.
Both organizations will maintain their locations and local leadership as part of the deal.

19 rural hospitals closed in 2019, up from 15 closures in 2018, and continuing a steady double-digit trend in closures since 2013.
Most hospitals closed because of financial problem, and 38% of rural hospitals are unprofitable.
Patients in communities affected by closure travel 12.5 miles on average for care. However, 43% of the closed hospitals are more than 15 miles to the nearest hospital, and 15% are more than 20 miles.
Despite a booming national economy, 2019 was the worst year for hospital closings since at least 2005.
The North Carolina Rural Health Research Program says that 19 rural hospitals closed this year, up from 15 closures in 2018, and continuing a steady double-digit trend in closures since 2013.
Since 2005, the North Carolina researchers tracked 162 hospital closings, with 60% of the closures occurring in southern states that did not expand Medicaid enrollment.
Texas led the way, with 23 hospital closures since 2005, followed by Tennessee with 13, and North Carolina with 11.
The closures have been blamed on a number of factors, including: the older, sicker, poorer, and less-concentrated rural demographic; bypassing by local residents seeking care at regional hospitals; hospital consolidation; value-based care; referral patterns of larger hospitals; the transition to outpatient services; and mismanagement.
Among the findings highlighted by the North Carolina Rural Health Research Program:
https://www.healthleadersmedia.com/innovation/eight-more-hospitals-join-pas-rural-health-model
The Rural Health Model creates an alternative payment model that transitions hospitals from fee-for-service to global budget payments.
Instead of getting paid for admissions, hospitals in the model will get a preset amount of money to provide services in the community.
State officials say the new payment model allows hospitals time to transform care to better meet the health needs of the community.
Eight more hospitals and one payer have joined a Pennsylvania initiative to shore up the financial footing of the state’s rural hospitals.
“I am especially pleased to see more hospitals joining this important initiative to improve their financial viability so that every Pennsylvanian has access to quality health care within a reasonable distance from home,” Gov. Tom Wolf said in a media release.
State officials the program is needed because nearly half of all rural hospitals in Pennsylvania are operating with negative margins and are at risk of closure. Four rural hospitals in Pennsylvania have shuttered since 2006, according to the North Carolina Rural Health Research Program.
So far this year, 19 rural hospitals across the nation have closed, making 2019 the worst year for rural hospital closures since at least 2005.
The Rural Health Model, the first of its kind, creates an alternative payment model that transitions hospitals from fee-for-service to global budget payments. Those global payments come from several payers, including private and public insurers.
Instead of getting paid for admissions, hospitals in the model will get a preset amount of money to provide services in the community.
State officials say the new payment model allows hospitals time to transform care to better meet the health needs of the community. This includes providing nontraditional roles, such as providing transportation and broadband internet access.
The eight hospitals are:
• Armstrong County Memorial Hospital in Kittanning.
• Chan Soon-Shiong Medical Center at Windber in Somerset County.
• Fulton County Medical Center in McConnellsburg.
• Greene Hospital in Waynesburg, Greene County.
• Monongahela Valley Hospital in Monongahela, Washington County.
• Punxsutawney Area Hospital in Punxsutawney, Jefferson County.
• Tyrone Hospital in Tyrone, Blair County.
• Washington Hospital in Washington, Washington County
A total of 67 hospitals are eligible for model based and nearly 20% of them will participate in in 2020, state officials said.
In addition, Aetna will join five other private payers – Gateway, Geisinger, Highmark, Medicare and UPMC – which combine make up nearly half of the individual and small group market insurance population in the state.
The program is funded and administered by the newly created Rural Health Redesign Center Authority and the Pennsylvania Rural Health Redesign Center Fund.
In addition to providing access to care for rural communities, state officials say the model will ensure that, by remaining open, rural hospitals continue to be a vital economic driver for their communities.
“The Rural Health Model is a transformative step that changes the financial model for hospitals in rural areas,” said Pennsylvania Secretary of Health Rachel Levine, MD. “This is a step that will help achieve financial stability for these facilities and aims to improve the overall health of the community.”
https://fee.org/articles/the-chart-that-could-undo-the-us-healthcare-system/
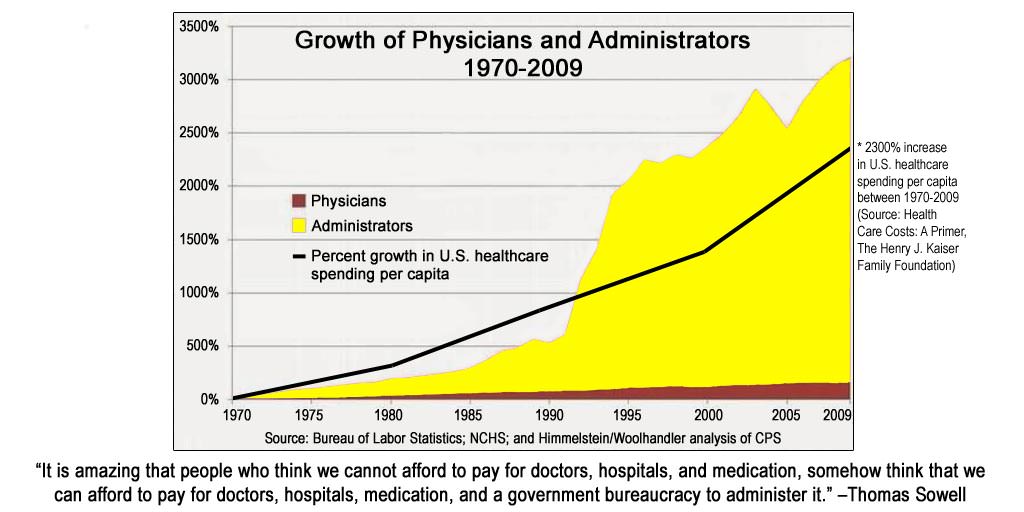
Skyrocketing costs are being driven by bureaucracy.
This chart looks remarkably similar to a chart that tracks the growth of the administrative class in higher education. And that’s no accident. As the physician who shared the chart writes:
[The chart] outlines the growth of administrators in healthcare compared to physicians over the last forty years. And, it includes an overlay of America’s healthcare spending over that same time. Take a look at the yellow color. A picture is worth a thousand words, isn’t it?
You see, when you have that much administration, what you really have is a bunch of meetings. Lots of folks carrying their coffee from place to place. They are meeting about more policies, more protocols to satisfy government-created nonsense. But, this type of thing in healthcare isn’t fixing things. It’s not moving the needle.
What moves things is innovation.
Innovation, indeed. But it’s not easy to innovate in stagnant, hyper-regulated, captured sectors.
In Tyler Cowen’s 2011 book the Great Stagnation, he argued that the areas that were stagnating the most are education, healthcare, and government. Writing about Cowen’s book in his Wall Street Journal blog, Kelly Evans says:
A particular challenge we confront is that our progress as a society — chiefly, in extending and improving lives — is now at a point in which it appears to be undercutting our potential for further advancement. Part of this, Mr. Cowen observes, stems from well-meaning efforts to do more with education, government, and health care that instead seem to have backfired and left us with noncompetitive institutions closer to failing us than to serving us well.
With respect to healthcare, this chart gives us an indication of why these efforts are backfiring: The more an industry becomes like a regulated utility, the more administrators are required to enforce the regulations and administer the programs. And they, as well as the programs they administer, are expensive. All manner of distortions follow, and the costs of healthcare go up proportionally.
There also seems to be perverse incentives associated with subsidy: The more resources you dump in, the more expensive that industry becomes. You might shift the costs around on unsuspecting groups (like taxpayers), but in almost every case we see premium hikes and tuition increases in both of these industries, despite (or rather because of) the truckloads of federal largesse.
But they will have to stop at some point — one way or the other.
The US healthcare system has become something of a Frankenstein monster, with pieces stitched together ad hoc by regulators and special interests. The ACA seems to have ignored most of what really needed fixing and doubled down on the worst aspects of our system. Price transparency, affordability, innovation and competitive entrepreneurship have all gotten worse, not better. And the beast has grown to take over more than 17 percent of GDP.
(And if you think 17 percent is about right, consider that in Singapore healthcare takes up less than 3 percent of GDP.)
The trouble with any further healthcare reform is that a massive coalition of special interests in multiple sectors has formed as a husk around the entire industry — a care-tel, if you will — and they will be very difficult to dislodge.
https://suneeldhand.com/2017/11/28/when-a-chart-speaks-a-thousand-words/

I happened to stumble across the above chart online the other day. It’s not new data, and was actually quoted in this major publication. I can write articles and parse the challenges we face till the cows come home, but nothing can really sum up what’s wrong with American healthcare more than this chart. It says everything and is quite obnoxious. What’s worse, it’s from 2009—and the curve has probably considerably diverged since then.
So that’s it, my blog post for the week. Just stare at this chart and take it all in. Feel free to comment below. I was going to write a long article on what these curves mean for healthcare. Then I thought to myself: absolutely nothing I write can possibly say more than the chart itself. It speaks not just a thousand words, but a million…..
Watched, for the hundredth time, “It’s a Wonderful Life” last night. Movie ends with George’s guardian angel writing this inside his Tom Sawyer book.