

Cartoon – Unpleasant Truths vs. Comforting Lies

Nations fighting in World War I were reluctant to report their flu outbreaks.
“Spanish flu” has been used to describe the flu pandemic of 1918 and 1919 and the name suggests the outbreak started in Spain. But the term is actually a misnomer and points to a key fact: nations involved in World War I didn’t accurately report their flu outbreaks.
Spain remained neutral throughout World War I and its press freely reported its flu cases, including when the Spanish king Alfonso XIII contracted it in the spring of 1918. This led to the misperception that the flu had originated or was at its worst in Spain.
“Basically, it gets called the ‘Spanish flu’ because the Spanish media did their job,” says Lora Vogt, curator of education at the National WWI Museum and Memorial in Kansas City, Missouri. In Great Britain and the United States—which has a long history of blaming other countries for disease—the outbreak was also known as the “Spanish grip” or “Spanish Lady.”
Historians aren’t actually sure where the 1918 flu strain began, but the first recorded cases were at a U.S. Army camp in Kansas in March 1918. By the end of 1919, it had infected up to a third of the world’s population and killed some 50 million people. It was the worst flu pandemic in recorded history, and it was likely exacerbated by a combination of censorship, skepticism and denial among warring nations.
“The viruses don’t care where they come from, they just love taking advantage of wartime censorship,” says Carol R. Byerly, author of Fever of War: The Influenza Epidemic in the U.S. Army during World War I. “Censorship is very dangerous during a pandemic.”

Patients lie in an influenza ward at the U.S. Army Camp Hospital No. 45 in Aix-les-Baines, France, during World War I.
Corbis/Getty Images
When the flu broke out in 1918, wartime press censorship was more entrenched in European countries because Europe had been fighting since 1914, while the United States had only entered the war in 1917. It’s hard to know the scope of this censorship, since the most effective way to cover something up is to not leave publicly-accessible records of its suppression. Discovering the impact of censorship is also complicated by the fact that when governments pass censorship laws, people often censor themselves out of fear of breaking the law.
In Great Britain, which fought for the Allied Powers, “the Defense of the Realm Act was used to a certain extent to suppress…news stories that might be a threat to national morale,” says Catharine Arnold, author of Pandemic 1918: Eyewitness Accounts from the Greatest Medical Holocaust in Modern History. “The government can slam what’s called a D-Notice on [a news story]—‘D’ for Defense—and it means it can’t be published because it’s not in the national interest.”
Both newspapers and public officials claimed during the flu’s first wave in the spring and early summer of 1918 that it wasn’t a serious threat. The Illustrated London News wrote that the 1918 flu was “so mild as to show that the original virus is becoming attenuated by frequent transmission.” Sir Arthur Newsholme, chief medical officer of the British Local Government Board, suggested it was unpatriotic to be concerned with the flu rather than the war, Arnold says.
The flu’s second wave, which began in late summer and worsened that fall, was far deadlier. Even so, warring nations continued to try to hide it. In August, the interior minister of Italy—another Allied Power—denied reports of the flu’s spread. In September, British officials and newspaper barons suppressed news that the prime minister had caught the flu while on a morale-boosting trip to Manchester. Instead, the Manchester Guardian explained his extended stay in the city by claiming he’d caught a “severe chill” in a rainstorm.
Warring nations covered up the flu to protect morale among their own citizens and soldiers, but also because they didn’t want enemy nations to know they were suffering an outbreak. The flu devastated General Erich Ludendorff’s German troops so badly that he had to put off his last offensive. The general, whose empire fought for the Central Powers, was anxious to hide his troops’ flu outbreaks from the opposing Allied Powers.
“Ludendorff is famous for observing [flu outbreaks among soldiers] and saying, oh my god this is the end of the war,” Byerly says. “His soldiers are getting influenza and he doesn’t want anybody to know, because then the French could attack him.”

Patients at U. S. Army Hospital No. 30 at a movie wear masks because of an influenza epidemic.
The National Library of Medicine
The United States entered WWI as an Allied Power in April 1917. A little over a year later, it passed the 1918 Sedition Act, which made it a crime to say anything the government perceived as harming the country or the war effort. Again, it’s difficult to know the extent to which the government may have used this to silence reports of the flu, or the extent to which newspapers self-censored for fear of retribution. Whatever the motivation, some U.S. newspapers downplayed the risk of the flu or the extent of its spread.
In anticipation of Philadelphia’s “Liberty Loan March” in September, doctors tried to use the press to warn citizens that it was unsafe. Yet city newspaper editors refused to run articles or print doctors’ letters about their concerns. In addition to trying to warn the public through the press, doctors had also unsuccessfully tried to convince Philadelphia’s public health director to cancel the march.
The war bonds fundraiser drew several thousand people, creating the perfect place for the virus to spread. Over the next four weeks, the flu killed 12,191 people in Philadelphia.
Similarly, many U.S. military and government officials downplayed the flu or declined to implement health measures that would help slow its spread. Byerly says the Army’s medical department recognized the threat the flu posed to the troops and urged officials to stop troop transports, halt the draft and quarantine soldiers; but they faced resistance from the line command, the War Department and President Woodrow Wilson.
Wilson’s administration eventually responded to their pleas by suspending one draft and reducing the occupancy on troop ships by 15 percent, but other than that it didn’t take the extensive measures medical workers recommended. General Peyton March successfully convinced Wilson that the U.S. should not stop the transports, and as a result, soldiers continued to get sick. By the end of the year, about 45,000 U.S. Army soldiers had died from the flu.
The pandemic was so devastating among WWI nations that some historians have suggested the flu hastened the end of the war. The nations declared armistice on November 11 amid the pandemic’s worst wave.
In April 1919, the flu even disrupted the Paris Peace Conference when President Wilson came down with a debilitating case. As when the British prime minister had contracted the flu back in September, Wilson’s administration hid the news from the public. His personal doctor instead told the press the president had caught a cold from the Paris rain.

Each person who has died of COVID-19 was somebody’s everything. Even as we mourn for those we knew, cry for those we loved and consider those who have died uncounted, the full tragedy of the pandemic hinges on one question: How do we stop the next 100,000?
The United States has now recorded 100,000 deaths due to the coronavirus.
It’s a moment to collectively grieve and reflect.
Even as we mourn for those we knew, cry for those we loved and consider also those who have died uncounted, I hope that we can also resolve to learn more, test better, hold our leaders accountable and better protect our citizens so we do not have to reach another grim milestone.
Through public records requests and other reporting, ProPublica has found example after example of delays, mistakes and missed opportunities. The CDC took weeks to fix its faulty test. In Seattle, 33,000 fans attended a soccer match, even after the top local health official said he wanted to end mass gatherings. Houston went ahead with a livestock show and rodeo that typically draws 2.5 million people, until evidence of community spread shut it down after eight days. Nebraska kept a meatpacking plant open that health officials wanted to shut down, and cases from the plant subsequently skyrocketed. And in New York, the epicenter of the pandemic, political infighting between Gov. Andrew Cuomo and Mayor Bill de Blasio hampered communication and slowed decision making at a time when speed was critical to stop the virus’ exponential spread.
COVID-19 has also laid bare many long-standing inequities and failings in America’s health care system. It is devastating, but not surprising, to learn that many of those who have been most harmed by the virus are also Americans who have long suffered from historical social injustices that left them particularly susceptible to the disease.
This massive loss of life wasn’t inevitable. It wasn’t simply unfortunate and regrettable. Even without a vaccine or cure, better mitigation measures could have prevented infections from happening in the first place; more testing capacity could have allowed patients to be identified and treated earlier.
The COVID-19 pandemic is not over, far from it.
At this moment, the questions we need to ask are: How do we prevent the next 100,000 deaths from happening? How do we better protect our most vulnerable in the coming months? Even while we mourn, how can we take action, so we do not repeat this horror all over again?
Here’s what we’ve learned so far.
From the first weeks of the coronavirus outbreak in the United States, when the virus tore through the Life Care Center in Kirkland, Washington, nursing homes and long-term care facilities have emerged as one of the deadliest settings. As of May 21, there have been around 35,000 deaths of staff and residents in nursing homes and long-term care facilities, according to the nonprofit Kaiser Family Foundation.
Yet the facilities have continued to struggle with basic infection control. Federal inspectors have found homes with insufficient staff and a lack of personal protective equipment. Others have failed to maintain social distancing among residents, according to inspection reports ProPublica reviewed. Desperate family members have had to become detectives and activists, one even going as far as staging a midnight rescue of her loved one as the virus spread through a Queens, New York, assisted living facility.
What now? The risk to the elderly will not decrease as time goes by — more than any other population, they will need the highest levels of protection until the pandemic is over. The CEO of the industry’s trade group told my colleague Charles Ornstein: “Just like hospitals, we have called for help. In our case, nobody has listened.” More can be done to protect our nursing home and long term care population. This means regular testing of both staff and residents, adequate protective gear and a realistic way to isolate residents who test positive.
African Americans have contracted and died of the coronavirus at higher rates across the country. This is due to myriad factors, including more limited access to medical care as well as environmental, economic and political factors that put them at higher risk of chronic conditions. When ProPublica examined the first 100 recorded victims of the coronavirus in Chicago, we found that 70 were black. African Americans make up 30% of the city’s population.
What now? States should make sure that safety-net hospitals, which serve a large portion of low-income and uninsured patients regardless of their ability to pay, and hospitals in neighborhoods that serve predominantly black communities, are well-supplied and sufficiently staffed during the crisis. More can also be done to encourage African American patients to not delay seeking care, even when they have “innocent symptoms” like a cough or low-grade fever, especially when they suffer other health conditions like diabetes.
Racial disparities go beyond medicine, to other aspects of the pandemic. Data shows that black people are already being disproportionately arrested for social distancing violations, a measure that can undercut public health efforts and further raise the risk of infection, especially when enforcement includes time in a crowded jail.
We’ve known from the beginning there are some measures that help protect us from the virus, such as physical distancing. Yet millions of Americans haven’t been able to heed that advice, and have had no choice but to risk their health daily as they’ve gone to work shoulder-to-shoulder in meat-packing plants, rung up groceries while being forbidden to wear gloves, or delivered the mail. Those who are undocumented live with the additional fear of being caught by immigration authorities if they go to a hospital for testing or treatment.
What now? Research has shown that there’s a much higher risk of transmission in enclosed spaces than outdoors, so providing good ventilation, adequate physical distancing, and protective gear as appropriate for workers in indoor spaces is critical for safety. We also now know that patients are likely most infectious right before or at the time when symptoms start appearing, so if workplaces are generous about their sick leave policies, workers can err on the side of caution if they do feel unwell, and not have to choose between their livelihoods and their health. It’s also important to have adequate testing capacity, so infections can be caught before they turn into a large outbreak.
While health workers have not, thankfully, been dying at conspicuously higher rates, they continue to be susceptible to the virus due to their work. The national scramble for ventilators and personal protective equipment has exposed the just-in-time nature of hospitals’ inventories: Nurses across the country have had to work with expired N95 masks, or no masks at all. Health workers have been suspended, or put on unpaid leave, because they didn’t see eye to eye with their administrators on the amount of protective gear they needed to keep themselves safe while caring for patients.
First responders — EMTs, firefighters and paramedics — are often forgotten when it comes to funding, even though they are the first point of contact with sick patients. The lack of a coherent system nationwide meant that some first responders felt prepared, while others were begging for masks at local hospitals.
What now? As states reopen, it will be important to closely track hospital capacity, and if cases rise and threaten their medical systems’ ability to care for patients, governments will need to be ready to pause or even dial back reopening measures. It should go without saying that adequate protective gear is a must. I also hope that hospital administrators are thinking about mental health care for their staffs. Doctors and nurses have told us of the immense strain of caring for patients whom they don’t know how to save, while also worrying about getting sick themselves, or carrying the virus home to their loved ones. Even “heroes” need supplies and support.
There continue to be questions on which data is lacking, such as the effects of the coronavirus on pregnant women. Without evidence-based research, pregnant women have been left to make decisions on their own, sometimes trying to limit their exposure against their employer’s wishes.
Similarly, there’s a paucity of data on children’s risk level and their role in transmission. While we can confidently say that it’s rare for children to get very ill if they do get infected, there’s not as much information on whether children are as infectious as adults. Answering that question would not just help parents make decisions (Can I let my kid go to day care when we live with Grandma?) but also help officials make evidence-based decisions on how and when to reopen schools.
There’s some research I don’t want to rush. Experts say the bar for evidence should be extremely high when it comes to a vaccine’s safety and benefit. It makes sense that we might be willing to use a therapeutic with less evidence on critically ill patients, knowing that without any intervention, they would soon die. A vaccine, however, is intended to be given to vast numbers of healthy people. So yes, we have to move urgently, but we must still take the time to gather robust data.
Our nation’s leaders have many choices to make in the coming weeks and months. I hope they will heed the advice of scientists, doctors and public health officials, and prioritize the protection of everyone from essential workers to people in prisons and homeless shelters who does not have the privilege of staying home for the duration of the pandemic.
The coronavirus is a wily adversary. We may ultimately defeat it with a vaccine or effective therapeutics. But what we’ve learned from the first 100,000 deaths is that we can save lives with the oldest mitigation tactics in the public health arsenal — and that being slow to act comes with a terrible cost.
I refuse to succumb to fatalism, to just accepting the ever higher death toll as inevitable. I want us to make it harder for this virus to take each precious life from us. And I believe we can.

When President Trump took office in 2017, his team stopped work on new federal regulations that would have forced the health care industry to prepare for an airborne infectious disease pandemic such as COVID-19. That decision is documented in federal records reviewed by NPR.
“If that rule had gone into effect, then every hospital, every nursing home would essentially have to have a plan where they made sure they had enough respirators and they were prepared for this sort of pandemic,” said David Michaels, who was head of the Occupational Safety and Health Administration until January 2017.
There are still no specific federal regulations protecting health care workers from deadly airborne pathogens such as influenza, tuberculosis or the coronavirus. This fact hit home during the last respiratory pandemic, the H1N1 outbreak in 2009. Thousands of Americans died and dozens of health care workers got sick. At least four nurses died.
Studies conducted after the H1N1 crisis found voluntary federal safety guidelines designed to limit the spread of airborne pathogens in medical facilities often weren’t being followed. There were also shortages of personal protective equipment.
“H1N1 made it very clear OSHA did not have adequate standards for airborne transmission and contact transmission, and so we began writing a standard to do that,” Michaels said.
HIV/AIDS rule set the standard for protecting workers
OSHA experts were confident new airborne infectious disease regulations would make hospitals and nursing homes safer when future pandemics hit. That’s because similar rules had already been created for bloodborne pathogens such as Ebola and hepatitis.
Those rules, implemented during the HIV/AIDS epidemic, forced the health care industry to adopt safety plans and buy more equipment designed to protect staff and patients.
But making a new infectious disease regulation, affecting much of the American health care system, is time-consuming and contentious. It requires lengthy consultation with scientists, doctors and other state and federal regulatory agencies as well as the nursing home and hospital industries that would be forced to implement the standard.
Federal records reviewed by NPR show OSHA went step by step through that process for six years, and by early 2016 the new infectious disease rule was ready. The Obama White House formally added it to a list of regulations scheduled to be implemented in 2017.
Then came the presidential election.
An emphasis on deregulation
In the spring of 2017, the Trump team formally stripped OSHA’s airborne infectious disease rule from the regulatory agenda. NPR could find no indication the new administration had specific policy concerns about the infectious disease rules.
Instead, the decision appeared to be part of a wider effort to cut regulations and bureaucratic oversight.
“Earlier this year we set a target of adding zero new regulatory costs onto the American economy,” Trump said in December 2017. “As a result, the never-ending growth of red tape in America has come to a sudden, screeching and beautiful halt.”
The impact on the federal effort to protect health care workers from diseases such as COVID-19 was immediate.
“The infectious disease standard was put on the back burner. Work stopped,” said Michaels, now a professor at George Washington University.

A medical worker is assisted into personal protective equipment on May 8 before stepping into a patient’s room in the COVID-19 intensive care unit at Harborview Medical Center in Seattle.
Elaine Thompson/AP
A deadly escalation of the H1N1 crisis
This spring, hospitals and nursing homes found themselves facing much of the same crisis they experienced during the H1N1 outbreak, with many facilities unprepared and unequipped. Only this time the scale was larger and deadlier.
The federal government reports that at least 43,000 front-line health care workers have gotten sick, many infected, while caring for COVID-19 patients in facilities where personal protective equipment was being rationed.
“Even just a few months ago, I couldn’t have imagined that I would have been on a Zoom call reading out the names of registered nurses who have died on the front lines of a pandemic,” said Bonnie Castillo, who heads the National Nurses United union.
“The memorial was not only about grief. It was also about anger.”
OSHA’s infectious disease rule debated in Washington
Castillo said Congress should immediately implement the infectious disease regulations shelved by the Trump administration as an emergency rule before a second wave of the coronavirus hits.
“Which obviously would mandate that employers have the highest level of PPE, not the lowest,” she said.
Democrats in the House of Representatives passed a bill in mid-May that would do so, but the Republican-controlled Senate has blocked the measure, and the White House still opposes the rules.
The Trump administration hasn’t responded to NPR’s repeated inquiries about the infectious disease rule. But in a briefing call with lawmakers this month, the current head of OSHA, Loren Sweatt, argued enough rules are already in place to protect workers.
“We have mandatory standards related to personal protective equipment and bloodborne pathogens and sanitation standards,” Sweatt said in a recording provided to NPR. “We have existing standards that can address this area.”
The hospital industry also opposes the new safety rules. Nancy Foster with the American Hospital Association said voluntary guidelines for airborne pandemics are adequate.
“You’re right; they’re not regulations, but they are the guidance that we want to follow,” Foster said. “They set forth the expectation for infection control, so in a sense they’re just like regulations.”
But the infectious disease standard would have required the health care industry to do far more. It sets out specific standards for planning and training. It would also have forced facilities to stockpile personal protective equipment to handle “surges” of sick patients such as the ones seen with COVID-19.
NPR also found the lack of fixed regulations allowed the Trump administration to relax worker safety guidelines. Federal agencies did so repeatedly this spring as COVID-19 spread and shortages of personal protective equipment worsened.
As a consequence, hospitals could say they were meeting federal guidelines while requiring doctors and nurses to reuse masks and protective gowns after exposure to sick patients.

It’s amazing how many pandemic books there are, and how thoroughly the idea of a global pandemic had crept into our popular culture well before the current situation. My daughter and I watched the Tom Hanks movie Inferno over the weekend, mostly because we wanted to gaze at the city of Florence. It’s not a great movie, but it is visually stunning in several ways. The plot is not something I gave much attention to when I first saw the film a couple of years ago: a rich Ted-talking eccentric decides to kill off most of the people of the world to save the Earth from over-population and the ravages 16 billion people would mean for other species and the health of the biosphere.
When I first saw the film in 2016, I regarded the plotline (will the vial of lethal germs be released or not?) as nothing but the usual “James Bond” setup for whatever else happened in the film. This time I watched it with greater alertness.
The fact is, of course, that COVID-19 is a serious global nuisance that has disrupted the lives of all Americans in a way that almost nobody could have predicted (well, there is Bill Gates, of course), but it is not the Black Plague, which swept away somewhere between one-fourth and one-half of all Europeans between 1348-1352, or the Yellow Fever epidemic in Philadelphia, which killed one in 10 inhabitants of America’s largest city in 1793, or the Spanish Flu, which killed somewhere between 57 and 100 million people worldwide in 1918.
If the coronavirus eventually kills 5 million people worldwide, and a couple of hundred thousand Americans before the vaccines gallop in to save the day a year or 18 months hence, it will have been a comparatively minor event in the history of global pandemics. The moment when it appeared that the hospital and medical infrastructure of New York might collapse has now passed. And though the death toll continues to climb towards perhaps 150,000 American dead by Aug. 1, 2020, the national dread that created a sustained will-we-survive and how-will-we-cope conversation in virtually every household in the United States is mostly over. The question now is when and how (and if) the country can return to what the late John McCain called regular order.
In the past two months I have read more than a dozen pandemic books, from Daniel Defoe’s A Journal of the Plague Year (1721), to Stephen King’s endless The Stand (1978). They are all interesting. If you outline the takeaway insights from these books, written over the span of many hundreds of years, they all make essentially the same points:
https://www.governing.com/context/How-Jefferson-and-Franklin-Helped-End-Smallpox-in-America.html

The great scourge of Thomas Jefferson’s era (1743-1826) was smallpox. Historians have estimated that perhaps as many as 2 billion people have died of smallpox in recorded history. That’s a pretty arbitrary figure, but it certainly indicates how serious the problem was. Modern epidemiology has not only eliminated smallpox as a threat to civilization but has been engaged in a protracted debate about whether to snuff it out altogether once and for all, or to keep a tiny bit of it alive in a handful of tightly secured vials in case we need to study it in the face of other disease epidemics. It was officially declared eradicated in 1980.
For most of human history, you either got it or you didn’t and then you either survived it or you didn’t. George Washington was infected by smallpox in Barbados in 1751. He survived, and though he was slightly disfigured, he was thereafter immune to the disease. It is possible that this early brush with smallpox saved the American Revolution 20 years later. In 18th-century Europe, 400,000 people died annually of smallpox.
By the time Jefferson was born in 1743, there was an experimental inoculation procedure, but it was quite dangerous and therefore highly controversial. The idea was to give healthy individuals a very tiny amount of actual smallpox under quarantine and very carefully controlled conditions and simply hope that the person’s immune system would be able to fight it off. Survival would immunize that individual for life. The procedure required many weeks of quarantine, fasting, puking, and rest, followed by a very light diet through convalescence. John Adams wrote a fascinating account of his own inoculation in 1764. He was 28 years old.
Young Thomas Jefferson’s first journey out of his native Virginia was to Philadelphia in 1766 to be inoculated. He would have undertaken the procedure in Williamsburg or Norfolk had it been available. He made the long journey (eight to 10 days in either direction) because he wanted to protect himself from the disease and study the procedure at the same time for possible incorporation into his own community at Monticello. With his characteristic taciturnity about personal things, Jefferson did not leave us a detailed account of the medical procedure, which required prolonged isolation, personal discipline and a great deal of patience.
Inoculation was first introduced in Europe 40 years earlier. Lady Mary Wortley Montague (1689-1762) had spent time in Turkey as the wife of the British ambassador to the Ottoman Empire. There she had witnessed inoculation in the zenanas (segregated women’s quarters) she visited. She called the procedure “engrafting,” which she described in an important “Letter to a Friend” on April 1, 1717. Mrs. Montagu’s brother had died of smallpox four years earlier and she herself had survived a bout of smallpox in 1715, but with her famous beauty disfigured. She had her five-year-old son Edward inoculated in the British Embassy in Turkey.

When she returned with her family to Britain, she became an outspoken advocate for the procedure. The English medical establishment decried inoculation and denounced Mary Montagu. Still, in 1721 when a smallpox epidemic broke out in England, she had her daughter inoculated in London. This was the first recorded use of the procedure in England. The medical establishment was slow to accept the efficacy of inoculation, which it regarded as an “oriental folk remedy.” It seemed counter-intuitive and just wrong-headed to give a healthy person a dose of smallpox to try to prevent her or him from getting it by accident.
New England Puritan minister Cotton Mather (1663-1728) first promoted inoculation in America. In 1706, Reverend Mather purchased a black slave he named Onesimus (from the Epistle to Philemon). Ten years later, Onesimus told Mather he had been made immune to smallpox in Africa by having the pus of an infected person rubbed on an open wound on his arm. This is known as the variolation method. Mather interrogated other slaves to learn more, confirmed the story, and became an advocate for inoculation. He was subjected to the usual criticism and pushback. An explosive device was thrown through the window of his home. In this instance, racism joined fear as a means of discrediting the medical procedure. What possible wisdom could come from a slave?
The smallpox plague that disturbed Britain in 1721 found its way that same year to Boston. Now Mather and Dr. Zabdiel Boylston, the only physician in Boston who supported the technique, offered their inoculation services to anyone who would trust them. Of the 242 people Boylston inoculated, only six died, or one in 40. Of those who did not undergo the procedure, one in seven died.
America’s greatest exemplar of the Enlightenment, Benjamin Franklin, became a passionate advocate of the procedure after his first son Franky died of smallpox on Nov. 21, 1736, at the age of four. Because Franklin was known to be a friend to inoculation, rumors spread in Philadelphia that Franky had died from the procedure. To set the record straight, the grieving father wrote an article in the Pennsylvania Gazette on Dec. 30, 1736: He had “intended to get [Francis] inoculated as soon as he should have recovered sufficient strength from a flux with which he had been long afflicted.” Franklin assured the public that his son “received the distemper in the common way of infection.”
In 1774, Franklin, who was an indefatigable creator of associations, societies, clubs and public institutions, including volunteer fire departments and lending libraries, established the Society for Inoculating the Poor Gratis to help the poor people of Philadelphia have access to inoculation. In his famous autobiography, Franklin wrote: “In 1736 I lost one of my sons, a fine boy of four years old, by the smallpox taken in the common way. I long regretted bitterly and still regret that I had not given it to him by inoculation. This I mention for the sake of the parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it.”
As a young man, the future English physician Edward Jenner (1749-1823) overheard an English milkmaid say, “I shall never have smallpox for I have had cowpox. I shall never have an ugly pockmarked face.” Many years later, remembering the incident, Jenner, now a doctor, interrogated other milkmaids and then experienced one of the most important “eureka” moments in history. Without understanding how germs work, with no knowledge of anything called a virus, Dr. Jenner realized that cowpox (also known as kinepox) must be closely related to smallpox, and that surviving it seemed to make individuals immune to the more deadly disease. He reckoned that cowpox and smallpox must share some essential epidemiological element and since cowpox was neither lethal nor usually disfiguring, careful use of cowpox material would represent a superior protection against smallpox than variolation, which was a more dangerous procedure.
On May 14, 1796, Jenner inoculated an eight-year-old boy named James Phipps with kinepox pus. Phipps developed mild fever and discomfort. Ten days later he felt fine. Two months after that, Dr. Jenner inoculated the boy again, but this time with serum from a fresh smallpox sore. No disease developed. The smallpox vaccine had been born. Our term “vaccination” dates from this episode. Vaccination comes from the Latin word for cow, “vacca.” Jenner called the cowpox serum “vaccinia.” The terminology reminds us that all western vaccination stems from this moment in 1796.
No good deed goes unpunished, apparently, not even one that changes the history of the planet. In Britain, Edward Jenner was subjected to the usual harassment and ridicule. The paper he submitted to the Royal Society of England was rejected by none other than Sir Joseph Banks, one of Britain’s premier naturalists, botanists, and patrons of science. It took many years and the vaccination experiments of other physicians and scientists before Jenner’s work was vindicated.
Eventually, Jenner received worldwide recognition for his discovery. Devoted like Jefferson to the philanthropic principles of the Enlightenment, Dr. Jenner not only made no effort to enrich himself but devoted so much of his time and energy to promoting vaccination that he endured periods of real poverty. Finally, in 1802, the British Parliament voted him a reward of £10,000. Five years later he received £20,000 more from Parliament.
The true vaccine found its way to America thanks to Dr. John Haygarth of Bath. He sent some of Jenner’s material to Benjamin Waterhouse, a professor of physics at Harvard University. Waterhouse, in turn sent serum and reports of the vaccine’s efficacy to Thomas Jefferson, now the third president of the United States.

Dr. Edward Jenner discovered the true smallpox vaccine in 1796.
In the new world, inoculation had a very rough reception. When John Dalgleish and Archibald Campbell began inoculating individuals in Norfolk, Virginia, an angry mob burned down Campbell’s house. Similar incidents occurred in Salem and Marblehead, Mass. In Charleston, S.C., an inoculation control law of 1738 imposed a fine of £500 on anyone providing or receiving inoculation within two miles of the city. A similar law was passed in New York City in 1747.
The measures in New England were so draconian that Benjamin Waterhouse noted the paradox: “New England, the most democratical region on the face of the earth voluntarily submitted to more restrictions and abridgements of liberty, to secure themselves against that terrific scourge, than any absolute monarch could have enforced.” (This, strangely prescient, anticipates the current debate about liberty versus public health). It was in the middle colonies — Maryland, Pennsylvania, New Jersey — that inoculation was most tolerated in the second half of the 18th century. That’s why Jefferson made the long journey to Philadelphia to be inoculated in 1766.
Jefferson first became aware of the discovery of a true smallpox vaccine from the newspapers he read in Philadelphia and the new capitol in Washington, D.C. Then, on Dec. 1, 1800, just after Jefferson’s election to the presidency, Benjamin Waterhouse sent him his pamphlet on the vaccine with a lovely cover letter saying that he regarded Jefferson as “one of our most distinguished patriots and philosophers.” Jefferson responded immediately, thanking Waterhouse for the publication and declaring, with his usual grace, that “every friend of humanity must look with pleasure on this discovery, by which one evil the [more] is withdrawn from the condition of man: and contemplating the possibility that future improvements & discoveries, may still more & more lessen the catalogue of evils. in this line of proceeding you deserve well of your [country?] and I pray you to accept my portion of the tribute due you.”
The following June, Waterhouse sent Jefferson a long letter explaining how the vaccine must be administered, how the serum could be preserved over time, and how much the controversial procedure needed the public support of a man of Jefferson’s stature in the “republic of letters.” President Jefferson became known as a defender and promoter of vaccination. In fact, he even arranged for his protégé Meriwether Lewis to carry some of the serum with him up the Missouri River in 1804-05, instructing him to “carry with you some matter of the kine pox, inform those of them with whom you may be, of its efficacy as a preservative from the small pox; and instruct & encourage them in the use of it. This may be especially done wherever you may winter.” Unfortunately, by the time the Lewis and Clark Expedition reached their winter encampment in today’s North Dakota, the serum had become inert. Thus Jefferson’s philanthropic initiative to vaccinate the Native Americans of the American West was stillborn.
Then, on May 14, 1806, now in his second term, Jefferson wrote perhaps the greatest presidential fan letter of all time. He took time from his duties as president to write the following letter to Edward Jenner. I quote it in its entirety:
SIR,— I have received a copy of the evidence at large respecting the discovery of the vaccine inoculation which you have been pleased to send me, and for which I return you my thanks. Having been among the early converts, in this part of the globe, to its efficiency, I took an early part in recommending it to my countrymen. I avail myself of this occasion of rendering you a portion of the tribute of gratitude due to you from the whole human family. Medicine has never before produced any single improvement of such utility. Harvey’s discovery of the circulation of the blood was a beautiful addition to our knowledge of the animal economy, but on a review of the practice of medicine before and since that epoch, I do not see any great amelioration which has been derived from that discovery. You have erased from the calendar of human afflictions one of its greatest. Yours is the comfortable reflection that mankind can never forget that you have lived. Future nations will know by history only that the loathsome small-pox has existed and by you has been extirpated. Accept my fervent wishes for your health and happiness and assurances of the greatest respect and consideration.
Who would not have wished to receive this magnificent, selfless, public-spirited, and enlightened letter? Unfortunately, we do not know how or even if Dr. Jenner responded. Except in medical circles, Edward Jenner has been largely forgotten.


I have a Ph.D. from Harvard and a 20-month-old child.
Without child care, life revolves around the toddler.
I am a political science professor and researcher, but lacking child care, I count myself lucky to work a few hours each day.
I am increasingly aware there is no such thing as the so-called work/family conflict. This is not only a personal observation. Scholars have found that good jobs – full-time, with benefits – and family, without help, are simply incompatible.
The concept is also wrong. If three-quarters of American women become mothers, and also most women do paid work, then doing both is, well, life; it’s not some existential, context-free choice.
Work and family are both full-time pursuits. If the problem is framed as a choice between them, the battle is lost, since family will usually win. Telecommuting and “workplace flexibility” are important but do not make up for a lack of time and space to think and work.
Those who need care, especially little children, are needy and adorable, and mothers are evolutionarily disposed to focus on them.
(Whoops, excuse me, the toddler is trying to kill herself again … OK, child saved, with minimal screaming on both of our parts. Now what was I thinking? Did I reorder all our prescriptions? Hold on, I’ll be back.)
The national shift to home-based work and schooling has had challenging consequences for parents, especially mothers. Sometimes these effects are lovely, like giving us more time with family, but if your goal is getting work done, good luck to you.

Working at home these days without child care is incredibly difficult unless I can escape to another room and close a door. This inevitably triggers screaming, but oh well.
She’s worse than a cat; she climbs on me, presses things on the computer, sucks its edges and screams for attention, in addition to the normal baby bodily functions that comprise a disproportionate section of my thinking – when did she last poop? Is that a rash?
It’s not just me.
Submissions from women to academic journals have plummeted since COVID-19 hit.
One geography professor tweeted, “It’s hard enough to keep my head barely above the water with the kids at home and interruptions every 2 min … I can’t imagine writing a paper now.”
Another scholar said the data on diminished submissions from women made her cry because it wasn’t just her.
It turns out that someone has to supervise – and sometimes force – children’s learning, even if online, and this takes actual work. With parks, museums, sports, pools and movie theaters closed, and with kids mostly unable to hang out with friends, someone also has to do the physical and emotional labor of keeping children busy, engaged and upbeat. This too is work.
Then there is the simple fact that family members are eating, working and playing in houses most of the time, which means more cooking, more cleaning, more grocery shopping and, yes, more toilet paper.
(OMG the baby took a two-hour nap. I got to exercise and even shower. No time for leg-shaving but I’m still a new woman. Now what was I thinking…)
Because it is not just time, you see. Sometimes the child is playing quietly, and theoretically I could sit down and bang out a research article, but my brain is fuzzy as hell.
I used to wonder what cows thought, standing there chewing their cud in a field. Now I know. They are thinking nothing. Especially with the nursing, I have great sympathy with cows lately.
Before the baby, and before COVID-19, I had great plans for composing scholarly articles in my head during all that nursing downtime. But I forgot that hormones can change your brain and behavior.

Feminist theory and research finds that much of what people think of as “biological sex” – female or male – is socially constructed, as in, strongly based on culturally contingent assumptions about women and men as groups. I firmly believe, and teach, this as evidence-based truth.
Hormones, though, have undeniable physical and mental effects. If they are turning your body into a milk-production and child-protection facility, there can be some side effects on brain function. Many of these changes (increased empathy and vigilance) are useful evolutionarily, and the physical alterations appear to be short-lived. But there can also be negative effects on memory and focus. If your brain is your job, as mine is, this can cause some serious work disruption.
Pat Schroeder had two young children when first elected to Congress as a Democrat from Colorado in the 1970s. When asked how she could do both jobs, she famously replied, “I have a brain and a uterus, and I use them both.”
I try to live up to Schroeder’s standard, but lately I’ve found I have to qualify it; I tell myself she meant sequentially, not simultaneously.
Sequential is fine, as long as I have time and space to switch gears – I’m a first-time mom at 40 and the gears sometimes stick or stall out – and the peace of mind to focus beyond the child and the never-ending housework. We don’t call this “women’s work” anymore, and men do more than they used to, but it’s essential work and still mostly done by women.
With luck and science, COVID-19 will recede soon, and we can trickle back to offices, for which I have a newfound respect.
Will the U.S. take something positive from this crisis by learning an enduring lesson about the power of child care?
Americans tend to think of having children as an expensive, private choice. The alternative is to think of it as a public good.
Other countries offer far more generous parental leave and low-cost, high-quality daycare, knowing that “work versus family” is a false formulation. The U.S. is losing serious talent and promoting gender inequality by continuing to misunderstand the problem.
There are many potential options when child care is made a priority in a society.
Government subsidies for child care centers would help low-income workers have access to good care. The U.S. almost managed this in 1971, when Congress passed, on a bipartisan vote, a bill to establish child care centers across the country, funded in part by the federal government. President Richard Nixon vetoed the bill.
Universal pre-K starting at age 3, as in New York City, is another option to advance the interests of working parents and children.
And because working parents are drowning in high child-care costs, the government could offer subsidies and tax relief for curriculum-based care – which encourages child development and learning as well as safety – for those early years. I make a pretty good salary, but still, an extra US$1,000 a month or more to ensure my child is safe and well cared for while I work is painful.
It’s not a work-family conflict; it is a lack of high-quality, low-cost child care. Framing the problem otherwise damages the ability to enact good solutions.
It also makes a lot of good, hardworking parents feel enduring guilt over a problem that isn’t theirs alone to solve.

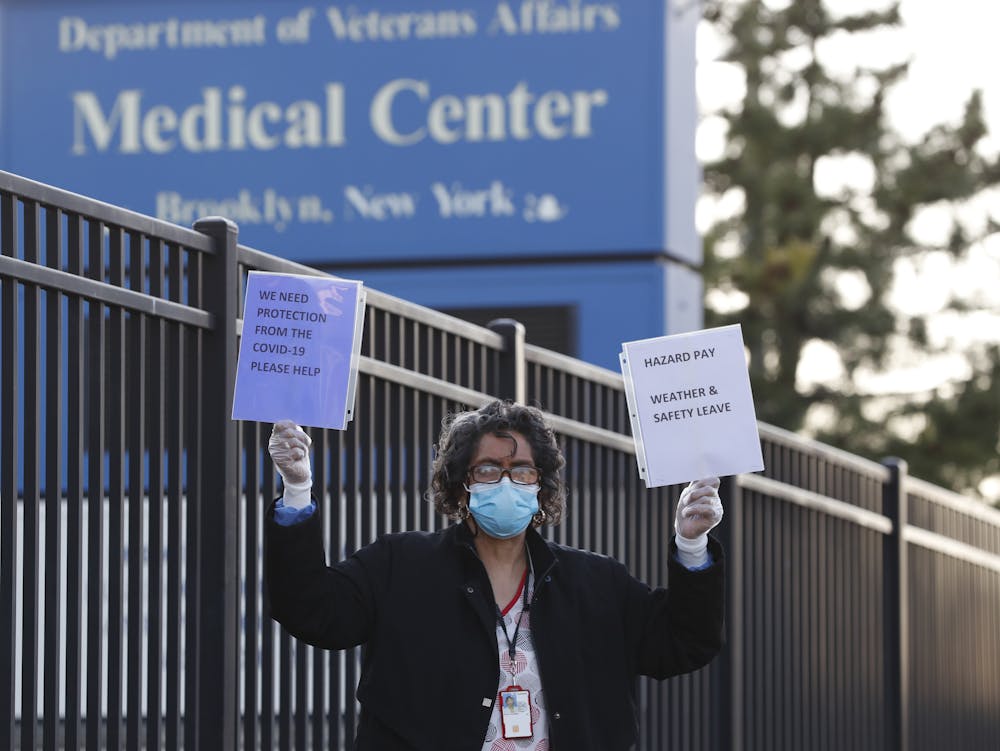
As the nation takes a day to memorialize its military dead, those who are living are facing a deadly risk that has nothing to do with war or conflict: the coronavirus.
Different groups face different degrees of danger from the pandemic, from the elderly who are experiencing deadly outbreaks in nursing homes to communities of color with higher infection and death rates. Veterans are among the most hard-hit, with heightened health and economic threats from the pandemic. These veterans face homelessness, lack of health care, delays in receiving financial support and even death.
I have spent the past four years studying veterans with substance use and mental health disorders who are in the criminal justice system. This work revealed gaps in health care and financial support for veterans, even though they have the best publicly funded benefits in the country.
Here are eight ways the pandemic threatens veterans:
In 2017, veterans’ median age was 64, their average age was 58 and 91% were male. The largest group served in the Vietnam era, where 2.8 million veterans were exposed to Agent Orange, a chemical defoliant linked to cancer.
Younger veterans deployed to Iraq and Afghanistan were exposed to dust storms, oil fires and burn pits with numerous toxins, and perhaps as a consequence have high rates of asthma and other respiratory illnesses.
Age and respiratory illnesses are both risk factors for COVID-19 mortality. As of May 22, there have been 12,979 people under Veterans Administration care with COVID-19, of whom 1,100 have died.
Veterans needing end-of-life care, those with cognitive disabilities or those needing substance use treatment often live in crowded VA or state-funded residential facilities.
State-funded “soldiers’ homes” are notoriously starved for money and staff. The horrific situation at the soldiers’ home in Holyoke, Massachusetts, where more than 79 veteran residents have died from a COVID-19 outbreak, illustrates the risk facing the veterans in residential homes.
When a person transitions from active military service to become a veteran, they receive a Certificate of Discharge or Release. This certificate provides information about the circumstances of the discharge or release. It includes characterizations such as “honorable,” “other than honorable,” “bad conduct” or “dishonorable.” These are crucial distinctions, because that status determines whether the Veterans Administration will give them benefits.
Research shows that some veterans with discharges that limit their benefits have PTSD symptoms, military sexual trauma or other behaviors related to military stress. Veterans from Iraq and Afghanistan have disproportionately more of these negative discharges than veterans from other eras, for reasons still unclear.
The Veterans Administration frequently and perhaps unlawfully denies benefits to veterans with “other than honorable” discharges.
Many veterans have requested upgrades to their discharge status. There is a significant backlog of these upgrade requests, and the pandemic will add to it, further delaying access to health care and other benefits.
Dental surgery, routine visits and elective surgeries at Veterans Administration medical centers have been postponed since mid-March. VA hospitals are understaffed – just before the pandemic, the VA reported 43,000 staff vacancies out of more than 400,000 health care staff positions. Access to health care will be even more difficult when those medical centers finally reopen because they may have far fewer workers than they need.
As of May 4, 2020, 2,250 VA health care workers have tested positive for COVID-19, and thousands of health care workers are under quarantine. The VA is asking doctors and nurses to come out of retirement to help already understaffed hospitals.
An average of 20 veterans die by suicide every day. A national task force is currently addressing this scourge.
But many outpatient mental health programs are on hold or being held virtually. Some residential mental health facilities have closed.
Under these conditions, the suicide rate for veterans may grow. Suicide hotline calls by veterans were up by 12% on March 22, just a few weeks into the crisis.
An estimated 45,000 veterans are homeless on any given night, and 181,500 veterans are in prison or jail. Thousands more are under court-supervised substance use and mental health treatment in veterans treatment courts. More than half of veterans involved with the justice system have either mental health problems or substance use disorders.
As residential facilities close to new participants, many veterans eligible to leave prison or jail have nowhere to go. They may stay incarcerated or become homeless.
Courts have moved online or ceased formal operations altogether, meaning no veteran charged with a crime can be referred to a treatment court. It is unclear whether those who were already participating in a treatment program will face delays graduating from court-supervised treatments.
Further, some veterans treatment courts still require participants to take drug tests. With COVID-19 circulating, those participants must put their health at risk to travel to licensed testing facilities.

In the pandemic’s epicenter in New York, tens of thousands of veterans should have access to VA benefits because of their low income – but don’t, so far.
The pandemic has exacerbated existing delays in finding veterans in need, filing their paperwork and waiting for decisions. Ryan Foley, an attorney in New York’s Legal Assistance Group, a nonprofit legal services organization, noted in a personal communication that these benefits are worth “tens of millions of dollars to veterans and their families” in the midst of a health and economic disaster.
All 56 regional Veterans Administration offices are closed to encourage social distancing. Compensation and disability evaluations, which determine how much money veterans can get, are usually done in person. Now, they must be done electronically, via telehealth services in which the veteran communicates with a health care provider via computer.
But getting telehealth up and running is taking time, adding to the longstanding VA backlog. Currently, more than 100,000 veterans wait more than 125 days for a decision. (That is what the VA defines as a backlog – anything less than 125 days is not considered a delay on benefit claims.)
There are 1.2 million veteran employees in the five industries most severely affected by the economic fallout of the coronavirus.
A disproportionately high number of post-9/11 veterans live in some of the hardest-hit communities that depend on these industries. Veterans returning from overseas will face a dire economic landscape, with far fewer opportunities to integrate into civilian life with financial security.
In addition, severely disabled veterans living off of VA benefits were initially required to file a tax return to get stimulus checks. This initial filing requirement delayed benefits for severely disabled veterans by at least a month. The IRS finally changed the requirements after public outcry, given that many older and severely disabled veterans do not have access to computers or the technological skills to file electronically.
There are many social groups to pay attention to, all with their own problems to face during the pandemic. With veterans, many of the problems they face now existed long before the coronavirus arrived on U.S. shores.
But with the challenges posed by the situation today, veterans who were already lacking adequate benefits and resources are now in deeper trouble, and it will be harder to answer their needs.
