In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
Artificial intelligence has long been heralded as a transformative force in medicine. Yet, until recently, its potential has remained largely unfulfilled.
Consider the story of MYCIN, a “rule-based” AI system developed in the 1970s at Stanford University to help diagnose infections and recommend antibiotics. Though MYCIN showed early promise, it relied on rigid, predetermined rules and lacked the flexibility to handle unexpected or complex cases that arise in real-world medicine. Ultimately, the technology of the time couldn’t match the nuanced judgment of skilled clinicians, and MYCIN never achieved widespread clinical use.
Fast forward to 2011, when IBM’s Watson gained global notoriety by besting renowned Jeopardy! champions Ken Jennings and Brad Rutter. Soon after, IBM applied Watson’s vast computing power to healthcare, envisioning it as a gamechanger in oncology. Tasked with synthesizing data from medical literature and patient records at Memorial Sloan Kettering, Watson aimed to recommend tailored cancer treatments.
However, the AI struggled to provide reliable, relevant recommendations—not because of any computational shortcoming but due to inconsistent, often incomplete, data sources. These included imprecise electronic health record entries and research articles that leaned too heavily toward favorable conclusions, failing to hold up in real-world clinical settings. IBM shut down the project in 2020.
Today, healthcare and tech leaders question whether the latest wave of AI tools—including much-heralded generative artificial intelligence models—will deliver on their promise in medicine or become footnotes in history like MYCIN and Watson.
Anthropic CEO Dario Amodei is among the AI optimists. Last month, in a sprawling 15,000-word essay, he predicted that AI would soon reshape humanity’s future. He claimed that by 2026, AI tools (presumably including Anthropic’s Claude) will become “smarter than a Nobel Prize winner.”
Specific to human health, Amodei touted AI’s ability to eliminate infectious diseases, prevent genetic disorders and double life expectancy to 150 years—all within the next decade.
When people ask me how to separate AI hype from reality in medicine, I suggest starting with three critical questions:
Question 1: Will the AI solution speed up a process or task that humans could eventually complete on their own?
Sometimes, scientists have the knowledge and expertise to solve complex medical problems but are limited by time and cost. In these situations, AI tools can deliver remarkable breakthroughs.
Consider AlphaFold2, a system developed by Google DeepMind to predict how proteins fold into their three-dimensional structures. For decades, researchers struggled to map these large, intricate molecules—the exact shape of each protein requiring years and millions of dollars to decipher. Yet, understanding these structures is invaluable, as they reveal how proteins function, interact and contribute to diseases.
With deep learning and massive datasets, AlphaFold2 accomplished in days what would have taken labs decades, predicting hundreds of proteins’ structures. Within four years, it mapped all known proteins—a feat that won DeepMind researchers a Nobel Prize in Chemistry and is now accelerating drug discovery and medical research.
Another example is a collaborative project between the University of Pittsburgh and Carnegie Mellon, where AI analyzed electronic health records to identify adverse drug interactions. Traditionally, this process took months of manual review to uncover just a few risks. With AI, researchers were able to examine thousands of medications in days, drastically improving speed and accuracy.
These achievements show that when science has a clear path but lacks the speed, tools and scale for execution, AI can bridge the gap. In fact, if today’s generative AI technology existed in the 1990s, ChatGPT estimates it could have sequenced the entire human genome in less than a year—a project that originally took 13 years and $2.7 billion.
Applying this criterion to Amodei’s assertion that AI will soon eliminate most infectious diseases, I believe this goal is realistic. Today’s AI technology already analyzes vast amounts of data on drug efficacy and side effects, discovering new uses for existing medications. AI is also proving effective in guiding the development of new drugs and may help address the growing issue of antibiotic resistance. I agree with Amodei that AI will be able to accomplish in a few years what otherwise would have taken scientists decades, offering fresh hope in the fight against human pathogens.
Question 2: Does the complexity of human genetics make the problem unsolvable, no matter how smart the technology?
Imagine searching for a needle in a giant haystack. When a single answer is hidden within mountains of data, AI can find it much faster than humans alone. But if that “needle” is metallic dust, scattered across multiple haystacks, the challenge becomes insurmountable, even for AI.
This analogy captures why certain medical problems remain beyond AI’s reach. In his essay, Amodei predicts that generative AI will eliminate most genetic disorders, cure cancer and prevent Alzheimer’s within a decade.
While AI will undoubtedly deepen our understanding of the human genome, many of the diseases Amodei highlights as curable are “multifactorial,” meaning they result from the combined impact of dozens of genes, plus environmental and lifestyle factors. To better understand why this complexity limits AI’s reach, let’s first examine simpler, single-gene disorders, where the potential for AI-driven treatment is more promising.
For certain genetic disorders, like BRCA-linked cancers or sickle cell disease that result from a single-gene abnormality, AI can play a valuable role by helping researchers identify and potentially use CRISPR, an advanced gene-editing tool, to directly edit these mutations to reduce disease risk.
Yet even with single-gene conditions, treatment is complex.CRISPR-based therapies for sickle cell, for example, require harvesting stem cells, editing them in a lab and reinfusing them after risky conditioning treatments that pose significant health threats to patients.
Knowing this, it’s evident that the complications would only multiply when editing multifactorial congenital diseases like cleft lip and palate—or complex diseases that manifest later in life, including cardiovascular disease and cancer.
Put simply, editing dozens of genes simultaneously would introduce severe threats to health, most likely exceeding the benefits. Whereas generative AI’s capabilities are accelerating at an exponential rate, gene-editing technologies like CRISPR face strict limitations in human biology. Our bodies have intricate, interdependent functions. This means correcting multiple genetic issues in tandem would disrupt essential biological functions in unpredictable, probably fatal ways.
No matter how advanced an AI tool may become in identifying genetic patterns, inherent biological constraints mean that multifactorial diseases will remain unsolvable. In this respect, Amodei’s prediction about curing genetic diseases will prove only partially correct.
Question 3: Will the AI’s success depend on people changing their behaviors?
One of the greatest challenges for AI applications in medicine isn’t technological but psychological: it’s about navigating human behavior and our tendency toward illogical or biased decisions. While we might assume that people will do everything they can to prolong their lives, human emotions and habits tell a different story.
Consider the management of chronic diseases like hypertension and diabetes. In this battle, technology can be a strong ally. Advanced home monitoring and wearable devices currently track blood pressure, glucose and oxygen levels with impressive accuracy. Soon, AI systems will analyze these readings, recommend diet and exercise adjustments and alert patients and clinicians when medication changes are needed.
But even the most sophisticated AI tools can’t force patients to reliably follow medical advice—or ensure that doctors will respond to every alert.
Humans are flawed, forgetful and fallible. Patients skip doses, ignore dietary recommendations and abandon exercise goals. On the clinician side, busy schedules, burnout and competing priorities often lead to missed opportunities for timely interventions. These behavioral factors add layers of unpredictability and unresponsiveness that even the most accurate AI systems cannot overcome.
And in addition to behavioral challenges, there are biological issues that limit the human lifespan. As we grow older, the protective caps on our chromosomes wear down, causing cells to stop functioning. Our cells’ energy sources, called mitochondria, gradually fail, weakening our bodies until vital organs cease to function. Short of replacing every cell and tissue in our bodies, our organs will eventually give out. And even if generative AI could tell us exactly what we needed to do to prevent these failings, it is unlikely people would consistently follow the recommendations.
For these reasons, Amodei’s boldest prediction—that longevity will double to 150 years within a decade—won’t happen. AI offers remarkable tools and intelligence. It will expand our knowledge far beyond anything we can imagine today. But ultimately, it cannot override the natural and complex limitations of human life: aging parts and illogical behaviors.
In the end, you should embrace AI promises when they build on scientific research. But when they violate biological or psychological principles, don’t believe the hype.
Last week, the Food and Drug Administration (FDA) approved two gene therapy treatments for sickle cell disease, Casgevy and Lyfgenia.
Casgevy, jointly developed by Boston, MA-based Vertex Pharmaceuticals and Switzerland-based CRISPR Therapeutics, is the first approved treatment of any kind available to US patients that uses CRISPR’s gene-editing capabilities.
Lyfgenia, made by Somerville, MA-based Bluebird Bio, uses a more common retrovirus technique for genetic modification. The FDA estimates that about 20K Americans with sickle cell disease will be eligible for the therapies, limited to those patients 12 and older who have had episodes of debilitating pain.
Both treatments will only be available at a small number of facilities nationwide, priced between $2-3M, and require a patient to endure months of hospitalization as well as intensive chemotherapy. Around 100K mostly Black Americans suffer from sickle cell disease, which causes intense pain, organ damage, and reduced life expectancy. Previously, the only curative treatment was a bone marrow transplant.
The Gist: The approval of these drugs represents a milestone moment for those suffering from sickle cell disease, while Casgevy also fulfills the revolutionary promise scientists have seen in CRISPR since it first received broad attention in 2005.
However, now that gene-editing therapies have graduated from the domain of scientific possibility into the realities of our healthcare delivery system, the new challenge becomes ensuring accessibility and equity, as many Americans who most stand to benefit from it also experience barriers in access to care and insurance coverage. (We’d expect insurer pushback similar to that seen when the first highly effective, but extremely costly, hepatitis C treatments like Solvaldi hit the market a decade ago this month.)
While the clinical trial patients who received Casgevy reporthaving “a new lease on life”, sky–high costs, questions of insurance coverage, and the arduous, time-intensive nature of the procedure stand in the way of a population-wide cure for sickle cell disease.
Two pioneers of mRNA research — the technology that helped the world tame the virus behind the Covid-19 pandemic — won the 2023 Nobel Prize in medicine or physiology on Monday.
Overcoming a lack of broader interest in their work and scientific challenges, Katalin Karikó and Drew Weissman made key discoveries about messenger RNA that enabled scientific teams to start developing the tool into therapies, immunizations, and — as the pandemic spread in 2020 — vaccines targeting the SARS-CoV-2 coronavirus. Moderna and the Pfizer-BioNTech partnership unveiled their mRNA-based Covid-19 shots in record time thanks to the foundational work of Karikó and Weissman, helping save millions of lives.
Karikó, a biochemist, and Weissman, an immunologist, performed their world-changing research on the interaction between mRNA and the immune system at the University of Pennsylvania, where Weissman, 64, remains a professor in vaccine research. Karikó, 68, who later went to work at BioNTech, is now a professor at Szeged University in her native Hungary, and is an adjunct professor at Penn’s Perelman School of Medicine.
The duo will receive 11 million Swedish kronor, or just over $1 million. Their names are added to a list of medicine or physiology Nobel winners that prior to this year included 213 men and 12 women.
The award was announced by Thomas Perlmann, secretary general of Nobel Assembly, in Stockholm. Perlmann said he had spoken to both laureates, describing them as grateful and surprised even though the pair has won numerous awards seen as precursors and had been tipped as likely Nobel recipients at some point.
Every year, the committee considers hundreds of nominations from former Nobel laureates, medical school deans, and prominent scientists from fields including microbiology, immunology, and oncology. Members try to identify a discovery that has altered scientists’ understanding of a subject. And according to the criteria laid out in Alfred Nobel’s will, that paradigm-shifting discovery also has to have benefited humankind.
The Nobel committee framed Karikó and Weissman’s work as a prime example of complementary expertise, with Karikó focused on RNA-based therapies and Weissman bringing a deep knowledge about immune responses to vaccines.
But it was not an easy road for the scientists. Karikó encountered rejection after rejection in the 1990s while applying for grants. She was even demoted while working at Penn, as she toiled away on the lower rungs of academia.
But the scientists persisted, and made a monumental discovery published in 2005 based on simply swapping out some of the components of mRNA.
With instructions from DNA, our cells make strands of mRNA that are then “read” to make proteins. The idea underlying an mRNA vaccine then is to take a piece of mRNA from a pathogen and slip it into our bodies. The mRNA will lead to the production of a protein from the virus, which our bodies learn to recognize and fight should we encounter it again in the form of the actual virus.
It’s an idea that goes back to the 1980s, as scientific advances allowed researchers to make mRNA easily in their labs. But there was a problem: The synthetic mRNA not only produced smaller amounts of protein than the natural version in our cells, it also elicited a potentially dangerous inflammatory immune response, and was often destroyed before it could reach target cells.
Karikó and Weissman’s breakthrough focused on how to overcome that problem. mRNA is made up of four nucleosides, or “letters”: A, U, G, and C. But the version our bodies make includes some nucleosides that are chemically modified — something the synthetic version didn’t, at least until Karikó and Weissman came along. They showed that subbing out some of the building blocks for modified versions allowed their strands of mRNA to sneak past the body’s immune defenses.
While the research did not gain wide attention at the time, it did catch the attention of scientists who would go on to found Moderna and BioNTech. And now, nearly 20 years later, billions of doses of mRNA vaccines have been administered.
For now, the only authorized mRNA products are the Covid-19 shots. But academic researchers and companies are exploring the technology as a potential therapeutic platform for an array of diseases and are using it to develop cancer vaccines as well as immunizations against other infectious diseases, from flu to mpox to HIV. An mRNA vaccine is highly adaptable compared to earlier methods, which makes it easier to alter the underlying recipe of the shot to keep up with viral evolution.
As she gained global fame, Karikó has been open about the barriers she encountered in her scientific career, which raised broader issues about the challenges women and immigrants can face in academia. But she’s said she always believed in the potential of her RNA research.
“I thought of going somewhere else, or doing something else,” Karikó told STAT in 2020, recalling the moment she was demoted. “I also thought maybe I’m not good enough, not smart enough. I tried to imagine: Everything is here, and I just have to do better experiments.”
Albert Einstein determined that time is relative. And when it comes to healthcare, five years can be both a long and a short amount of time.
In August 2018, I launched the Fixing Healthcare podcast. At the time, the medium felt like the perfect auditory companion to the books and articles I’d been writing. By bringing on world-renowned guests and engaging in difficult but meaningful discussions, I hoped the show would have a positive impact on American medicine. After five years and 100 episodes, now is an opportune time to look back and examine how healthcare has improved and in what ways American medicine has become more problematic.
Here’s a look at the good, the bad and the ugly since episode one of Fixing Healthcare:
The Good
Drug breakthroughs and government actions headline medicine’s biggest wins over the past five years.
At first, health experts expressed doubts that Pfizer, Moderna and others could create a safe and effective Covid-19 vaccine with messenger RNA (mRNA) technology. After all, no one had succeeded in more than two decades of trying.
Thanks in part to Operation Warp Speed, the government-funded springboard for research, our nation produced multiple vaccines within less than a year. Previously, the quickest vaccine took four years to develop (mumps). All others required a minimum of five years.
The vaccines were pivotal in ending the coronavirus pandemic, and their success has opened the door to other life-saving drugs, including those that might prevent or fight cancer. And, of course, our world is now better prepared for when the next viral pandemic strikes.
Weight-Loss Drugs
Originally designed to help patients manage Type 2 diabetes, drugs like Ozempic have been helping people reverse obesity—a condition closely correlated with diabetes, heart disease and cancer.
For decades, America’s $150 billion a year diet industry has failed to curb the nation’s continued weight gain. So too have calls for increased exercise and proper nutrition, including restrictions on sugary sodas and fast foods.
In contrast, these GLP-1 medications are highly effective. They help overweight and obese people lose 15 to 25 pounds on average with side effects that are manageable for nearly all users.
The biggest stumbling block to their widespread use is the drug’s exorbitant price (upwards of $16,000 for a year’s supply).
Drug-Pricing Laws
With the Inflation Reduction Act of 2022, Congress took meaningful action to lower drug prices, a move the CBO estimates would reduce the federal deficit by $237 billion over 10 years.
It’s a good start. Americans today pay twice as much for the same medications as people in Europe largely because of Congressional legislation passed in 2003.
That law, the Medicare Prescription Drug Price Negotiation Act, made it illegal for Health and Human Services (HHS) to negotiate drug prices with manufacturers—even for the individuals publicly insured through Medicare and Medicaid.
Now, under provisions of the new Inflation Reduction Act, the government will be able to negotiate the prices of 10 widely prescribed medications based on how much Medicare’s Part D program spends. The lineup is expected to include prescription treatments for arthritis, cancer, asthma and cardiovascular disease. Unfortunately, the program won’t take effect until 2026. And as of now, several legal challenges from both drug manufacturers and the U.S. Chamber of Commerce are pending.
The Bad
Spiking costs, ongoing racial inequalities and millions of Americans without health insurance make up three disappointing healthcare failures of the past five years.
Cost And Quality
The U.S. spends nearly twice as much on healthcare per citizen as other countries, yet our nation lags 10 of the wealthiest countries in medical performance and clinical outcomes. As a result, Americans die younger and experience more complications from chronic diseases than people in peer nations.
As prices climb ever-higher, at least half of Americans can’t afford to pay their out-of-pocket medical bills, which remain the leading cause of U.S. bankruptcy. And with rising insurance premiums alongside growing out-of-pocket expenses, more people are delaying their medical care and rationing their medications, including life-essential drugs like insulin. This creates a vicious cycle that will likely prolong today’s healthcare problems well into the future.
Health Disparities
Inequalities in American medicine persist along racial lines—despite action-oriented words from health officials that date back decades.
Today, patients in minority populations receive unequal and inequitable medical treatment when compared to white patients. That’s true even when adjusting for differences in geography, insurance status and socioeconomics.
Racism in medical care has been well-documented throughout history. But the early days of the Covid-19 pandemic provided several recent and deadly examples. From testing to treatment, Black and Latino patients received both poorer quality and less medical care, doubling and even tripling their chances of dying from the disease.
The problems can be observed across the medical spectrum. Studies show Black women are still less likely to be offered breast reconstruction after mastectomy than white women. Research also finds that Black patients are 40% less likely to receive pain medication after surgery. Although technology could have helped to mitigate health disparities, our nation’s unwillingness to acknowledge the severity of the problem has made the problem worse.
Uninsurance
Although there are now more than 90 million Americans enrolled in Medicaid, there are still 30 million people without any health insurance. This disturbing reality comes a full decade after the passage of the Affordable Care Act.
On Capitol Hill, there is no plan in place to reduce the number of uninsured.
Moreover, many states are looking to significantly rollback their Medicaid enrollment in the post-Covid era. Kaiser Family Foundation estimates that between 8 million and 24 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provisions implemented during the pandemic. Without coverage, people have a harder time obtaining the preventive services they need and, as a result, they suffer more chronic diseases and die younger.
The Ugly
An overall decrease in longevity, along with higher maternal mortality and a worsening mental-health crisis, comprise the greatest failures of U.S. healthcare over the past five years.
Life Expectancy
Despite radical advances in medical science over the past five years, American life expectancy is back to where it was at the turn of the 20th century, according to CDC data.
Alongside environmental and social factors are a number of medical causes for the nation’s dip in longevity. Research demonstrated that many of the 1 million-plus Covid-19 deaths were preventable. So, too, was the nation’s rise in opioid deaths and teen suicides.
Regardless of exact causation, Americans are living two years less on average than when we started the Fixing Healthcare podcast five years ago.
Maternal Mortality
Compared to peer nations, the United States is the only country with a growing rate of mothers dying from childbirth. The U.S. experiences 17.4 maternal deaths per 100,000 live births. In contrast, Norway is at 1.8 and the Netherlands at 3.0.
The risk of dying during delivery or in the post-partum period is dramatically higher for Black women in the United States. Even when controlling for economic factors, Black mothers still suffer twice as many deaths from childbirth as white women.
And with growing restrictions on a woman’s right to choose, the maternal mortality rate will likely continue to rise in the United States going forward.
Mental Health
Finally, the mental health of our country is in decline with rates of anxiety, depression and suicide on the rise.
These problems were bad prior to Covid-19, but years of isolation and social distancing only aggravated the problem. Suicide is now a leading cause of death for teenagers. Now, more than 1 in every 1,000 youths take their own lives each year. The newest data show that suicides across the U.S. have reached an all-time high and now exceed homicides.
Even with the expanded use of telemedicine, mental health in our nation is likely to become worse as Americans struggle to access and afford the services they require.
The Future
In looking at the three lists, I’m reminded of a baseball slugger who can occasionally hit awe-inspiring home runs but strikes out most of the time. The crowd may love the big hitter and celebrate the long ball, but in both baseball and healthcare, failing at the basics consistently results in more losses than wins.
Over the past five years, American medicine has produced a losing record. New drugs and surgical breakthroughs have made headlines, but the deeper, more systemic failures of American healthcare have rarely penetrated the news cycle.
If our nation wants to make the next five years better and healthier than the last five, elected officials and healthcare leaders will need to make major improvements. The steps required to do so will be the focus of my next article.
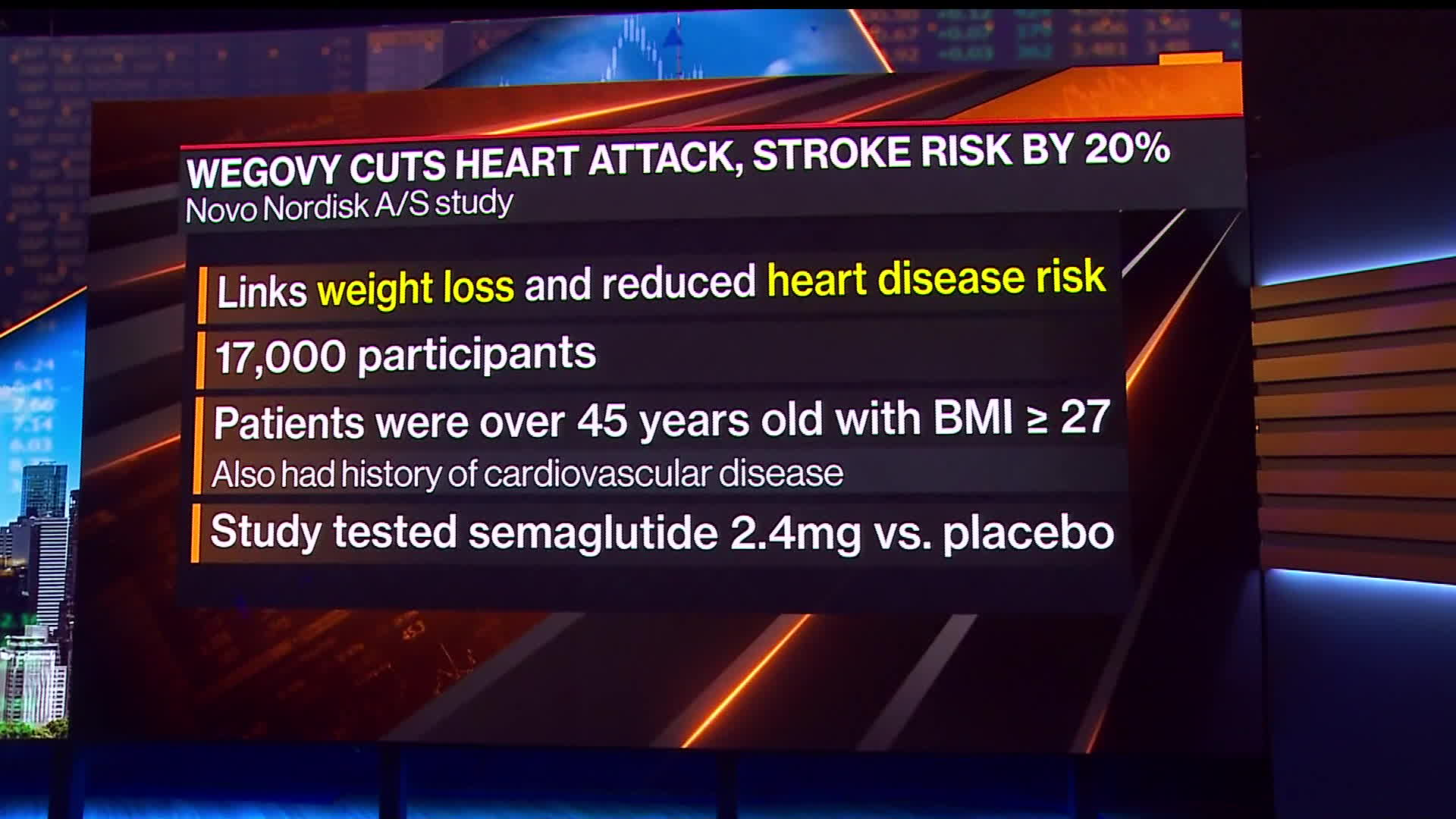
On Tuesday, Novo Nordisk released the headline results of a large clinical trial demonstrating that its popular GLP-1 inhibitor Wegovy reduced the risk of heart attacks, strokes, and cardiovascular deaths by 20 percent. The SELECT trial enrolled roughly 17,600 non-diabetic adults aged 45 and older who were overweight or obese with established cardiovascular disease. It compared people in this population treated with the drug to those given a placebo, and tracked them for up to five years. The drugmaker said it plans to release the full trial results at a conference later this year. These results are similar to a previous study that found Wegovy sister drug Ozempic, also made by Novo Nordisk, reduced the risk of adverse cardiac events by 26 percent in adults with type 2 diabetes.
The Gist: The cardioprotective effects demonstrated in this study far exceeded researchers’ expectations. Though concerns still abound about the high costs of Wegovy (nearly $1,350 per month) and similar drugs, these results will certainly put pressure on Medicare and other insurers to provide coverage.
Questions remain around how the drug actually improves cardiovascular outcomes, and whether patients with cardiac disease who are not overweight or obese might also benefit from taking it.
Despite the fact that the data are still preliminary, the argument that obesity medications are solely “lifestyle” or “vanity drugs”—which some insurers and employers have been using to deny coverage—will now be much harder to defend.
Headlines recently blared about the new review that looked at how effective masks are at preventing the transmission of flu-like disease. Cochrane reviews are well respected, and the media coverage about the recent review has been hard to parse. So is that it, end of story on masks? Not if you skip the media headlines and read the actual review!
Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
Can bivalent boosters prevent another surge of infections?
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
How much additional protection do updated shots provide?
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Will we see an increase in vaccine uptake?
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”
In a randomized controlled trial (RCT) study of 85K Europeans, published this week in the New England Journal of Medicine, colonoscopies were found to reduce incidence of colorectal cancer by only 18 percent—much less than earlier large studies—and have no impact on ten-year colorectal cancer mortality rates. This is the first study to directly compare individuals invited to receive colonoscopies with a control group receiving no cancer screening.
While the study’s findings surprised many researchers, an important caveat to the headline takeaways is that a secondary analysis of study participants who actually completed their colonoscopies found a 50 percent reduction in death, though the decision to accept the invitation likely correlates with other factors that improve mortality outcomes.
The Gist: We were surprised to learn this was the first RCT to assess the effectiveness of colonoscopies—15M of which are performed in the US each year—and which comprise a $36B market. While the study’s results need careful interpretation, it reminds us that much of established medical consensus has yet to be “proven” by rigorous scientific research.
While we don’t expect this study’s results to significantly change colonoscopy recommendations, it does place greater emphasis on the question of value generated by widespread preventative screenings. Colonoscopy will almost certainly remain the gold standard for colon cancer screening in the US, but if these results bear out, other less invasive types of screening, like home-based fecal immunochemical testing, could be viewed as equivalent options and receive more traction.