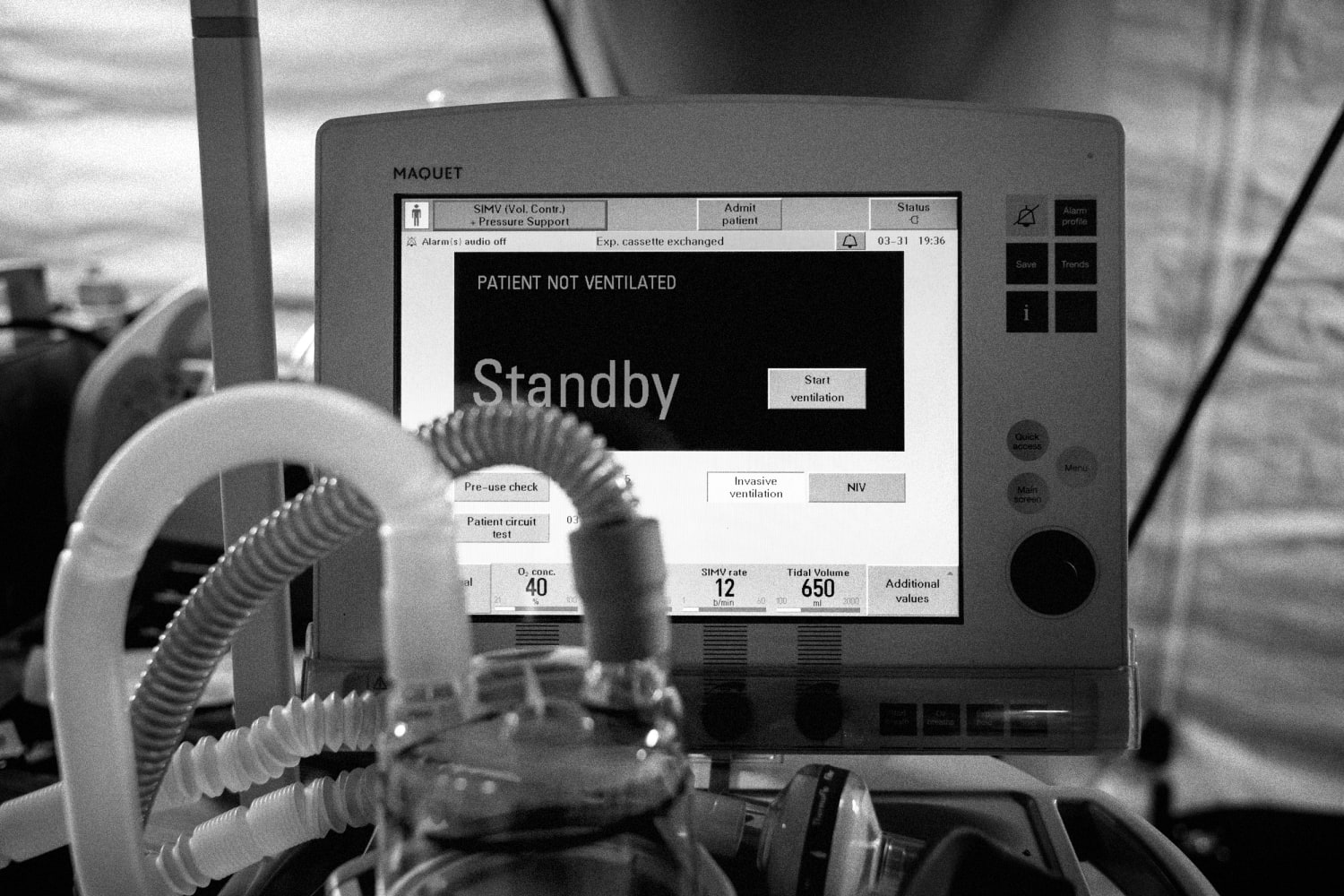
Hospital executives in California are sounding alarms on their inpatient capacity as COVID-19 hospitalizations surge in the state, according to ABC News.
As of Dec. 23, California is among the eight states where the virus is spreading quickest. On Dec. 22, the state saw one of its biggest jumps in one-day COVID-19 hospitalizations, with an additional 653 patients admitted to hospitals.
Officials from Oakland-based Kaiser Permanente, San Francisco-based Dignity Health and Sacramento-based Sutter Health said during a Dec. 22 news conference that they are facing capacity issues. In some cases, COVID-19 patients are being treated in hallways, gift shops and conference rooms.
Greg Adams, the chairman and CEO of Kaiser Permanente, said during the conference, “We simply will not be able to keep up if the COVID surge continues to increase. We’re at or near capacity everywhere.”
Many hospital officials said Thanksgiving gatherings contributed to the surge. The executives urged Californians to not gather for Christmas and New Year’s.
An estimated 803,000 people applied for unemployment aid for the first time last week, the Labor Department said Wednesday, showing the economy’s persistent weakness as new drama swirls over Washington’s response to the crisis. The figure was a slight decrease from the previous week but still much higher than normal.
The new Labor Department data show how weak the economy is, particularly the labor market. The surge in new coronavirus cases and deaths in the past few months has cooled the partial economic recovery from the summer.
Retail sales have weakened, and hiring has slowed markedly. The travel and tourism industries have not recovered much of the business lost since March, and thousands of companies — particularly restaurants and bars — have closed. U.S. household spending slipped in November, marking the first drop since April.
After months of stop-and-start negotiations, the bipartisan stimulus package finally offered some hope for households and businesses fighting to make it through the winter.
If Trump does not sign the bill, up to 14 million Americans would lose unemployment aid after Christmas. An eviction moratorium will expire at the end of the year, and $25 billion in emergency rental assistance will not get out the door. Billions of dollars for nutrition assistance, aid for small businesses, child care, transportation services and more will be in jeopardy, and the government will shut down on Dec. 29.
Trump did not play much of a role in the economic relief talks that resulted in Congress passing the $900 billion stimulus package. In the video Trump posted Tuesday night, his main complaint was that he wanted the $600 stimulus checks in the package to be increased to $2,000. This would add $370 billion to the measure.
Democrats quickly rallied around Trump’s demand, and House Speaker Nancy Pelosi (D-Calif.) plans to try to hold a vote on it as soon as Thursday. But it could be virtually impossible to pass such a measure through Congress with unanimous support, leaving the entire bill’s future uncertain.
The stimulus package would extend unemployment benefits of up to $300 per week, beginning as soon as Dec. 27 and run at least through mid-March. The measure also would extend Pandemic Unemployment Assistance — which targets part-time and gig workers who did not qualify for state unemployment insurance benefits — for 11 weeks.
Wednesday’s data showed nearly 400,000 new claims for the Pandemic Unemployment Assistance program.
Rare words from an incoming president: “Our darkest days in the battle against COVID are ahead of us, not behind us,” President-elect Biden warned this afternoon during remarks in Wilmington.
Why it matters:Biden is promising to tell America the truth, which includes the reality of many more horrific months, no matter who is in charge.
If we’re lucky, vaccinations will provide enough herd immunity to allow some normality by this summer or fall.
Another blunt reality: Most of the benefits in the $900 billion coronavirus rescue package expire months before America has any hope of being back to normal.
The $300 boost for unemployment benefits expires in March.
The new $284 billion round of the Paycheck Protection Program (PPP) is meant to last 3 months.
There’s no new funding earmarked for state and local governments.
The other side:There’s funding for schools and childcare and mass transit and vaccination distribution, which helps bail out the above from those obligations.
The entertainment sector got $15 billion, helping out theaters and museums and live entertainment venues.
$600 checks will start showing up next week for individuals making under $75,000 (phases out for incomes above that), with an extra $600 per child.
The bottom line: Georgia’s Jan. 5 Senate runoffs could be the difference between a big stimulus under Biden, or more trouble for parts of the U.S. hospitality sector.
An investment firm has bought more than 20 nursing homes during the coronavirus pandemic, leading to disruptions at multiple facilities that weakened care for vulnerable residents amid the worst health crisis in generations, interviews and documents show.
From April through July, the New Jersey-based Portopiccolo Group — which buys troubled nursing homes and tries to make them profitable — paid hundreds of millions of dollars to acquire facilities in Maryland, Virginia and elsewhere.
The purchases drew scant scrutiny from regulators despite poor safety records at dozens of the company’s other nursing homes, including hefty fines for infection-control lapses and shortages of staff.
Many of Portopiccolo’s existing facilities were struggling to contain outbreaks of the coronavirus when its leaders went seeking new properties, state health records show. At a Virginia nursing home, staff hosted a hallway dance party for residents in April, weeks after federal guidelines had cautioned against such events. Conditions were so bad at one North Carolina facility that it was placed on a federal watch list even after the Centers for Disease Control and Prevention dispatched a strike team to help.
At its new nursing homes in Maryland, Portopiccolo’s operating companies made major changes to insurance and time-off benefits, failed to buy enough supplies and protective equipment and asked some employees to keep working after testing positive for coronavirus, said 14 current and former employees from four of the eight facilities.
Many veteran staffers quit as a result of the changes, said the employees, most of whom spoke on the condition of anonymity because they feared reprisals. Those who remained found themselves tending to dozens of residents at a time, the employees said.
“It was hair on fire,” said Katrina Pearthree, a former social worker at two facilities purchased by Portopiccolo over the last 15 months. She resigned from her job after losing health insurance coverage and disagreeing with new managers on patient care.
Portopiccolo spokesman John Collins denied that caregiving suffered and said that while benefits changed, they remained competitive within the industry. The firm, he said, wants to fill the gap left by nursing home owners exiting the industry because of the pandemic.
“Our company was founded by people who share a passion for caring for the sick, elderly and forgotten,” Collins said in a statement. “Any attempts to characterize our work or the work of our teams differently is flat out wrong.”
Elder-care advocates say Portopiccolo’s record of fines at other facilities, and the timing of its acquisitions, should have raised red flags for regulators, especially as the virus decimated the country’s nursing home population.
But the Centers for Medicare and Medicaid Services (CMS), the main federal agency regulating nursing homes, said the only way it tracks ownership changes is when facilities report the information for Medicare enrollment.
President-elect Joe Biden has said he wants to increase federal oversight through mandatory audits of nursing home cost reports and ownership data. Typically, such monitoring has fallen to state regulators, said Charlene Harrington, a professor emerita of sociology and nursing at the University of California at San Francisco. But even before the coronavirus crisis, she said, most states did a poor job.
In Maryland, the commission that oversees changes in nursing home ownership said the sale of a facility requires little more than “timely notification.” Virginia officials said they don’t closely monitor such sales, either.
“Your history indicates what you’re going to do in the future,” said Richard Mollot, executive director of a national advocacy group called the Long Term Care Community Coalition. “There needs to be more oversight of these purchases.”
‘From bad to worse’
Portopiccolo founders Simcha Hyman, 31, and Naftali Zanziper, 38, bought their first nursing home in 2016 after selling their medical supplies company to a private equity firm. They have since purchased more than 70 facilities in nine states, including 18 in Virginia. The nursing homes are run by operating companies set up and financed by the firm, including Peak Healthcare, Accordius Health and Pelican Health — a trend first reported by the business magazine Barron’s.
For years, Hyman and Zanziper described Portopiccolo as a private equity firm. But that description, along with the group’s promise to swiftly turn “distressed assets” profitable, was removed from the Portopiccolo website in early December after inquiries from The Washington Post about the firm’s nursing home acquisitions.
Collins said the label “private equity” — which typically describes groups that raise funding from private investors — is inaccurate. He declined to explain why the group described itself that way for months, including in news releases, and still does on its LinkedIn page.
Atul Gupta, a professor of health-care management at the Wharton School at the University of Pennsylvania, said it is possible Portopiccolo is trying to rebrand itself because of the increasingly negative stigma tied to private equity groups — which have been criticized for slashing costs at nursing homes, then selling them off to new owners.Studies, by Gupta and others, show that private equity ownership correlates with declines in staffing and quality of care.
Collins declined to say how many facilities Portopiccolo owns, how many it has sold or how much the firm has profited. Neither Peak Healthcare nor Accordius Health responded to multiple requests for comment.
An analysis of federal data shows that nearly 70 percent of facilities Portopiccolo owned before the pandemic have Medicare ratings of one or two stars out of five — based on patient-care metrics such as staffing ratios and infection control.
Two Portopiccolo facilities last month were placed in a federal monitoring program for having “a history of serious quality issues”; two others were listed as candidates because of severe deficiencies. Prior to the pandemic, the firm’s facilities in North Carolina were fined more than $480,000 for violating state and federal rules, federal data shows.
One facility placed in the monitoring program was the Citadel Salisbury, a one-star nursing home in Salisbury, N.C., where more than 150 staff and residents have contracted the virus, according to state data. Employees and residents alleged in a lawsuit filed in Rowan County Superior Court that Portopiccolo, which bought the facility from Genesis HealthCare on Feb. 1, left the nursing home woefully unprepared for the pandemic.
Employees testified in sworn affidavits that managers from Accordius, the operating group, prohibited staff from wearing masks in March, saying that doing so would scare residents. Nurses sometimes had to care for more than 50 residents at a time, employees alleged.
The lawsuit asks that the facility be required to improve conditions or be closed or put under new ownership. But lawyers for Portopiccolo asserted that staffing and equipment have been adequate. Hyman, Zanziper and Accordius executives sought to downplay their role at the Citadel, claiming in a motion to dismiss that daily operations were the responsibility of staff on site.
At the same time, Portopiccolo sued the families in federal court, arguing that they had signed agreements that preclude litigation against the nursing home.
Such arbitration clauses have become increasingly common at for-profit nursing homes,studies show, and have been criticized by consumer advocates as well as lawmakers as a way for facilities to avoid accountability. Biden said he wants to restore an Obama-era ban on the practice that was overturned by the Trump administration.
In June, North Carolina officials identified a slew of violations at the Citadel that they said placed residents in “immediate jeopardy,” including a systemic failure to control infection and failing to inform the families of those who tested positive. Some found out their relatives had the virus from an emergency room physician. One man said he learned his aunt had died only when a funeral director called, asking what to do with her body.
Two hundred miles away in Virginia, staff shortages at Accordius Health in Harrisonburg were so dire before the pandemic that residents sometimes went days without showers, inspection records show.
“This place has gone from bad to worse,” one resident told an inspector. “They cut costs at our expense.”
After Accordius took over the facility in 2019, Ruth Simmers-Domzalski said, she noticed fewer staff members tending to her mother-in-law, Mary Domzalski, whose family twice found her lying on soiled bedsheets. On April 6, the facility held a hallway dance party where residents interacted without masks.
Domzalski, 88, attended. Three weeks later, she died of covid-19.
When asked about the event, Collins said the dance party did not conflict with federal guidelines at the time. CMS said on April 2 that all nursing home residents should cover their noses and mouths while interacting with staff; nearly a month before, it told facilities to cancel all group activities.
Tumultuous takeovers
Portopiccolo declined to say how many nursing homes it has bought during the pandemic, but The Post used CMS records to identify at least 22 facilities — eight in Maryland — that reported that Hyman and Zanziper had become owners since April.
Three of the Maryland facilities were bought from Genesis HealthCare, one of the largest skilled-nursing operators in the country. Amid plummeting occupancy rates and ballooning expenses, Genesis told stockholders this year that the firm would “improve its liquidity position” by selling off nearly two dozen of its roughly 400 nursing homes.
One was the Sligo Creek Center in Takoma Park, Md., where Pearthree, 59, worked part time as a social worker.
She had spent 18 years full time at another Genesis nursing home, the Fox Chase Rehabilitation Center in Silver Spring, leaving months after Portopiccolo bought it in 2019.
That sale was a “nightmare,” said Pearthree, recalling that new managers failed to secure local suppliers, leaving employees scrambling for medication and food. One afternoon, she said, staff members were unable to access digital patient records because Peak Healthcare had not put a new software system in place.
Less than a year after she left Fox Chase, Pearthree found herself facing another Portopiccolo takeover — this time amid a pandemic.
Again, the transition was chaotic. Peak did not actively recruit employees or offer them competitive packages prior to the takeover, leading to the departure of longtime staffers, including the administrator and director of nursing, said Pearthree and a senior Sligo Creek employee who spoke on the condition of anonymity because she feared reprisals. The former administrator and director of nursing did not respond to requests for comment.
Pearthree, a graduate student who worked 30 hours a week, was told she would have to increase her hours to keep her health insurance, she and Collins said.
Pearthree and the current employee also said Peak stopped providing hazard pay for contract employees and laid off a group of nonmedical staff Genesis had assembled to take temperatures and wipe down surfaces at the onset of the pandemic.
The facility has been cited twice by Maryand regulators since Peak took over, state inspection records show — in June for failing to test all residents and staff, and in August for failing to consistently inform family members of viral outbreaks.
Collins said staffing gaps were part of a nationwide shortage of nursing home workers and disputed the accounts from Pearthree and the current employee, saying supplies at both Sligo and Fox Chase were adequate and benefits were fair.
Eleven workers at three other Maryland nursing homes acquired by Portopiccolo during the pandemic said they lost paid time off and were offered more limited insurance packages. One worker who has asthma and high blood pressure said her bimonthly health insurance co-pay increased from $67 to $113 when Peak took over.
At Peak Healthcare Chestertown, on Maryland’s Eastern Shore, employees said the company offered a more limited benefits package than the facility’s previous owners, Autumn Lake, including less paid time off for new employees and no paid time off on major holidays.
The company scrimped on supplies, including cutlery, cleaning materials and clothing for residents, said employees at three facilities, who also spoke on the condition of anonymity out of fear of retribution.
Three employees at another facility said nurses have had to use hand soap to clean residents and rip up towels or bedsheets to dry them off.
“We risk our lives every day, and we don’t have proper supplies,” said one geriatric nursing assistant who brings her own gloves to work. “At what point do we put the patients first?”
Collins denied there were shortages, adding that at Chestertown, the budget for supplies had actually increased. He also denied that employees lost time off to which they were entitled, but said he could not address specific claims without knowing the names of the employees.
Reducing operating costs appears to be part of Portopiccolo’s business strategy, according to documents reviewed by The Post. In 2019, while acquiring three nursing homes in North Carolina, the group said it expected to save $360,000 by lowering expenses associated with employee benefits and insurance and $410,000 by cutting equipment and transportation costs. These measures, outlined in a mortgage loan contract, had allowed Portopiccolo to save more than $50 million across 37 facilities.
Collins said Portopiccolo has invested more than $6.7 million to purchase cleaning supplies and protective equipment since the start of this year. In comparison, Genesis, which operates about three times as many nursing homes, said that as of September, it had spent about $40 million more than normal on cleaning supplies and protective equipment.
Little government scrutiny
A recent study by the Long Term Care Community Coalition identified 15 states as having some good oversight practices for nursing home purchases, including requiring companies to disclose what other assets they own. Of the nine states in which Portopiccolo operates, none made the list.
“If your facilities in other states have very low staffing or a history of citations, you should not be allowed to purchase another one,” said Mollot, executive director of the coalition. “But states have a very hands-off approach to anything that happens outside their borders.”
Maryland Department of Health spokesman Charles Gischlar said the agency saw “no reason to change” the way it tracks shifts in nursing home ownership during the pandemic.
The Maryland Health Care Commission, another entity meant to oversee the sale of nursing homes, last year started asking prospective owners to affirm that they have not been convicted of a felony within the past 10 years or penalized more than $10 million because of their ownership of nursing homes.
But this requirement, which was designed “to keep out poor performers,” has not deterred a single transaction, said Paul Parker, a director at the commission.
For each facility that Hyman and Zanziper bought in Maryland, they declared to state regulators that they would not make substantive changes to services, staffing or bed ratios. State officials did not respond to questions asking how they ensured this would be true.
Gupta, the Wharton professor, said there should have been a moratorium on nursing home sales when the pandemic started because the changes that follow any acquisition can hamper a facility’s pandemic response.
But federal and state lawmakers never considered such a move.
“Nobody knew what was going on, nobody was in control,” Gupta said.
Joani Latimer, Virginia’s long-term-care ombudsman, said her office has been concerned by Portopiccolo’s pattern of buying facilities with low CMS ratings. Such facilities need more investment — not less — for conditions to turn around, she said.
“It’s not a process that you can just streamline to machine-like efficiency,” she said. “These are human needs with human challenges.”
Officials at the Virginia Department of Health, however, said they did not pay particular attention to Portopiccolo’s acquisition this year of Accordius Health at Courtland in Southampton County and Accordius Health at Waverly in Sussex County.
Such deals are “a business decision between the parties involved,” said Kimberly Beazley, director of the state Office of Licensure and Certification. “And we do not regulate business decisions made by facilities.”
Weeks with no hot water
Multiple employees at Portopiccolo-owned facilities, including one who worked in the kitchen at Chestertown, said their new managers had so much trouble filling staffing gaps this spring that employees were asked to work after learning they had the virus.
“It was a disaster,” said the Chestertown employee, who said she tested positive May 15 and declined when asked to come to work three days later. “People were still testing positive, and we were being asked to reapply for our jobs because this new company was coming in.”
Kent County Health Officer William Webb said local officials intervened that month after learning that a different employee at the facility who also had coronavirus was still working. “It was very concerning to me at the time, and we made sure to put a stop to it,” he said.
The facility’s water heater was broken from July to September, which meant there was no hot water for dishes or hand-washing. State inspectors fined the facility $730,000 for not fixing or reporting the problem, which they said posed “immediate jeopardy” to residents’ health. Collins said the firm is disputing the fine.
Webb said Peak’s decision not to promptly replace the water heater was “especially difficult” because the facility had seen scores of coronavirus cases and more than a dozen deaths in April and May. “If you’re in the business,” he said, “[you know] ample hot water is the core of any infection prevention program.”
When Peak took over managing the facility, roommates Patricia Sparkman, 82, and Brenda Middleton, 79, were isolated in their ground-floor room after testing positive for the virus.
Sparkman said in an interview that staff members left after the transition. Those who remained seemed less able to help, she said, including with basic tasks like bringing her water.
Middleton’s daughter, Tina Hurley, said the family moved Middleton a few months later to Peak Healthcare at Denton, about 30 miles away, so they could visit more frequently. But that facility had also been acquired by Portopiccolo on May 1.
Hurley said her mother is rarely checked on in Denton and has fallen several times while trying to get things for herself. At one point, she added, Middleton injured her leg but went without care from the facility’s doctor for days.
“I wouldn’t have brought her here if I knew how bad it would be,” Hurley said.
For Pearthree, the social worker at Sligo Creek, the breaking point came when she was asked to transfer back to Fox Chase in mid-May as director of social work. By then, Peak was operating both facilities.
She found residents she had known for years alone in their rooms, she said, confused and despondent in some cases. Relatives of those who died, she added, were given little information about how or when their loved ones had gotten sick.
When she raised concerns with managers, she said, she was brushed aside.
“The families felt betrayed by us,” Pearthree said. “And that was the part that overwhelmed me.” She sent a resignation letter in June.
Collins said Fox Chase administrators were unaware of her resignation and said Pearthree was terminated after she stopped coming to work. But the executive director of Fox Chase left Pearthree a voice mail on June 3 acknowledging her resignation and pleading with her to return.
“You do your job great and I like that,” the director said in the voice mail, which Pearthree shared with The Post.
Collins said that Portopiccolo leaders see their employees as “health care heroes.”
“We remain committed to putting care first,” he added.
Days before Thanksgiving, as all but one of the firm’s Maryland facilities reported new coronavirus outbreaks to the state, the firm closed on deals worth $37.7 million to acquire four more facilities in Florida.
Pre-Christmas air travel surpassed 1 million daily passengers nationwide for three consecutive days this weekend — breaking the record for most weekend travelers of the pandemic and outpacing Thanksgiving numbers that assumed that title and worried health experts last month. The 3.2 million passengers screened Friday, Saturday and Sunday mark the only time during the pandemic that over 1 million air travelers were seen three days in a row.
The influx in air travel undercuts health officials’ guidance for Americans to stay home this holiday season. The Centers for Disease Control and Prevention issued guidance earlier this month that discouraged travel and urged those who need to travel to acquire coronavirus tests before and after their journey.
The next two contenders for busiest travel weekends were those before and after Thanksgiving, Transportation Security Administration spokesperson Daniel Velez said in an email. Pre-Thanksgiving weekend saw 3,052,139 travelers, with the following weekend logging 2,961,120.
On Saturday, TSA spokesperson Lisa Farbstein noted the upswing in passenger volume on Twitter and shared images of TSA agents sanitizing security checkpoints, which have new touchless procedures and glass barriers between travelers and staff.
Farbstein also reminded passengers that they are permitted to bring up to 12 ounces of hand sanitizer through security — more than the standard three-ounce limit that applies to other liquids — during the pandemic.
“Until further notice, passengers may bring one container of hand sanitizer up to 12oz in carry-on bags,” the TSA said in a tweet. “Expect containers to be screened separately, which may add time to the checkpoint screening experience.”
While the amount of people flying every day is still consistently less than half of the same numbers seen last year before the pandemic began, the influx marks a steady increase in the frequency of days in which travel volumes surpass 1 million daily passengers. Since March, there have been a total of eight days that saw more than 1 million screenings: One occurred in October, four in November, and three have been recorded so far this month.https://a85aee93c838e6222057ae0ce825fc95.safeframe.googlesyndication.com/safeframe/1-0-37/html/container.html
“Travel can increase your chance of spreading and getting COVID-19. Postponing travel and staying home is the best way to protect yourself and others from COVID-19,” the CDC said in updated guidance on Dec. 2. For those who do plan to travel, the agency recommends getting tested one to three days before the trip and three to five days afterward. It also says to “reduce non-essential activities for a full 7 days after travel, even if your test is negative.”
Those unable to acquire a test, the guidance says, should “reduce non-essential activities for 10 days after travel.”
While the strain has not yet been reported in the United States, New York Gov. Andrew M. Cuomo (D) on Monday called for the country to follow suit and ban travel from the United Kingdom.
“Right now, this variant in the U.K. is getting on a plane and flying to JFK,” Cuomo said on a conference call with reporters. “We have about six flights a day coming in [to JFK airport] from the U.K., and we have done absolutely nothing.”
After officials in the United Kingdom said Saturday that the variant first identified there was spreading 70 percent faster than others, Google searches about the mutation have spiked. But American public health experts and federal officials say that although it appears that the variant may be more contagious, it is not any more dangerous than others already detected in the United States.
“I don’t think there should be any reason for alarm right now,” Adm. Brett Giroir, who has been in charge of testing, told George Stephanopoulos on ABC’s “This Week.”
Variations to the virus are nothing new, and experts say the novel coronavirus does not mutate as much as influenza, meaning it is less likely that a vaccine would need to be developed every year to keep up with the new strains.
Still, much about this variant remains unknown, such as whether it is a new strain — a functionally different version of the virus.
“The take-home message for right now is that we need to get more information,” said Krutika Kuppalli, an infectious-diseases specialist at the Medical University of South Carolina. “In the meantime, we all need to really double down on our public health measures — wearing masks, remaining physically distanced, avoiding crowds of people.”
Where has the variant been detected?
In September, U.K. researchers discovered the variant’s prevalence when they collected samples from infected people in southeastern England. It seemed to spread quickly.
“This lineage came up quite rapidly,” Nick Loman, one of the researchers and a professor of microbial genomics at the University of Birmingham, told The Washington Post.
Since then, Australia, Denmark and the Netherlands have identified cases of the variant in their countries, the World Health Organization told the BBC. On Sunday, Italian officials announced that a patient returning from Britain “in the last few days” was in isolation after scientists detected the mutation.
In South Africa, health officials said Sunday that a version of the virus similar to the U.K. variant has been found in 80 to 90 percent of samples analyzed since mid-November.
Is the variant already in the United States?
The virus has not been detected in the United States, but officials are watching for developments in Britain, Giroir told Stephanopoulos.
Although guidance from federal agencies discourages traveling to Britain, the United States has not banned travel from there.
“I really don’t believe we need to do that yet,” Giroir said.
But New York Gov. Andrew M. Cuomo (D) pointed out Sunday that it would take only one flight to the United States to spread the mutation, urging federal officials to restrict travel.
“Right now, this variant in the U.K. is getting on a plane and flying to JFK,” Cuomo said on a conference call with reporters.
However, Kuppalli warned that little is known about the effectiveness of a ban, referring to instances in which people rushed to airports and congregated in long lines trying to travel before restrictions were put into effect earlier in the pandemic.
It is also not entirely certain whether the virus gained its foothold in the southeast of England because of its altered genetic markers or through super-spreading events, said Scott Gottlieb, a former head of the Food and Drug Administration.
“It seems like this new strain is more contagious,” Gottlieb said on CBS’s “Face the Nation.” “It doesn’t seem to be any more virulent, any more dangerous than run-of-the-mill covid. The next question is: Will it obviate our natural immunity?”
Will the authorized vaccines still be effective against this variant of the virus?
As of now, experts say there has been no indication that the variant is resistant to the Pfizer and Moderna vaccines authorized by the FDA.
“There is no reason to believe that the vaccines that have been developed will not be effective against this virus as well,” Vivek H. Murthy, President-elect Joe Biden’s nominee for surgeon general, told host Chuck Todd on NBC’s “Meet the Press.” “The bottom line is if you’re at home and hearing this news, it does not change what we do in terms of precautions.”
Although the vaccine remains out of reach for most Americans, following guidance such as social distancing and wearing masks remains the most practical way to prevent transmission.
Several hospitals in Los Angeles County are preparing for the possibility of restrategizing care delivery in the coming weeks amid growing COVID-19 hospitalizations, according to the Los Angeles Times.
Los Angeles County reported 6,018 COVID-19 hospitalizations Dec. 20 — a 2.5 percent increase from the day prior — with 1,198 patients in ICUs, according to the state’s data dashboard. Statewide, 17,750 patients are hospitalized with COVID-19, 3,710 of them in ICUs.
The LA Times obtained a document recently circulated among physicians at the four county-run hospitals that outlines resource allocation in crisis situations. The guidelines call for physicians to save as many patients as possible versus trying everything to save a patient, meaning those less likely to survive will not receive the level of care they would have otherwise. L.A. County Health Services Director Christina Ghaly, MD, told the LA Times that the guidelines were not in place as of Friday night.
California activated its “mass fatality” program last week, which coordinates mutual aid across several government agencies when more deaths take place in a period of time than can be handled by local coroner or medical emergency personnel, NPR reports.
Nearly all of the state is under stay-at-home orders, with residents prohibited from gathering with anyone outside their immediate household.
“I have yet to see any clear signals that things are slowing down, and I’m very concerned about the next two months,” Timothy Brewer, MD, an epidemiologist with UCLA Health, told the LA Times. He said UCLA Health is scheduling several infectious disease specialists to be on call at any time, and the biggest issue is that hospitals may quickly run out of providers who can administer ICU-level care.
Congressional leaders have reached an agreement on a $900 billion COVID-19 relief package and $1.4 trillion government funding deal with several healthcare provisions, according to Senate Majority Leader Mitch McConnell, R-Ky., and Minority Leader Chuck Schumer, D-N.Y.
Here are seven things to know about the relief aid and funding deal:
1. Congressional leaders have yet to release text of the COVID-19 legislation, but have shared a few key details on the measure, according to CNBC.Becker’s breaks down the information that has been released thus far.
2. The COVID-19 package includes $20 billion for the purchase of vaccines, about $9 billion for vaccine distribution and about $22 billion to help states with testing, tracing and other COVID-19 mitigation programs, according to Politico.
3. Lawmakers are also expected to include a provision changing how providers can use their relief grants. In particular, the bill is expected to allow hospitals to calculate lost revenue by comparing budgeted revenue for 2020. Hospitals have said this tweak will allow them to keep more funding.
4. The agreement also allocates $284 billion for a new round of Paycheck Protection Program loans.
5. The COVID-19 relief bill also provides$600 stimulus checks to Americans earning up to $75,000 per year and $600 for their children, according to NBC. It also provides a supplemental $300 per week in unemployment benefits.
6. The year-end spending bill includes a measure to ban surprise billing. Under the measure, hospitals and physicians would be banned from charging patients out-of-network costs their insurers would not cover. Instead, patients would only be required to pay their in-network cost-sharing amount when they see an out-of-network provider, according to The Hill.The agreement gives insurers 30 days to negotiate a payment on the outstanding bill. After that period, they can enter into arbitration to gain higher reimbursement.
7. Lawmakers plan to pass the relief bill and federal spending bill Dec. 21.
A Florida taxi driver and his wife had seen enough conspiracy theories online to believe the virus was overblown, maybe even a hoax. So no masks for them. Then they got sick. She died. A college lecturer had trouble refilling her lupus drug after the president promoted it as a treatment for the new disease. A hospital nurse broke down when an ICU patient insisted his illness was nothing worse than the flu, oblivious to the silence in beds next door.
Lies infected America in 2020. The very worst were not just damaging, but deadly.
President Donald J. Trump fueled confusion and conspiracies from the earliest days of the coronavirus pandemic. He embraced theories that COVID-19 accounted for only a small fraction of the thousands upon thousands of deaths. He undermined public health guidance for wearing masks and cast Dr. Anthony Fauci as an unreliable flip-flopper.
But the infodemic was not the work of a single person.
Anonymous bad actors offered up junk science. Online skeptics made bogus accusations that hospitals padded their coronavirus case numbers to generate bonus payments. Influential TV and radio opinion hosts told millions of viewers that social distancing was a joke and that states had all of the personal protective equipment they needed (when they didn’t).
It was a symphony of counter narrative, and Trump was the conductor, if not the composer. The message: The threat to your health was overhyped to hurt the political fortunes of the president.
Every year, PolitiFact editors review the year’s most inaccurate statements to elevate one as the Lie of the Year. The “award” goes to a statement, or a collection of claims, that prove to be of substantive consequence in undermining reality.
It has become harder and harder to choose when cynical pundits and politicians don’t pay much of a price for saying things that aren’t true. For the past month, unproven claims of massive election fraud have tested democratic institutions and certainly qualify as historic and dangerously bald-faced. Fortunately, the constitutional foundations that undergird American democracy are holding.
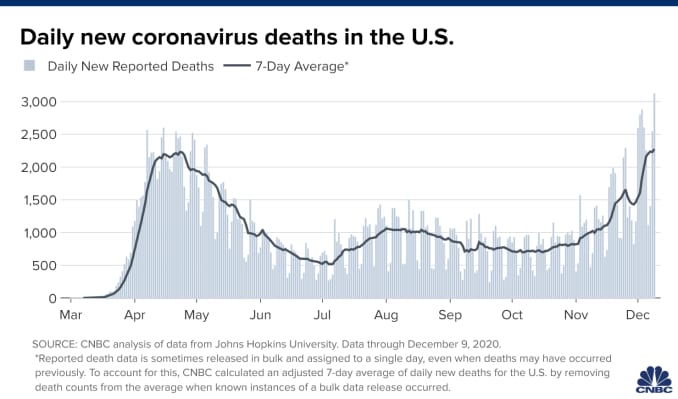
Meanwhile, the coronavirus has killed more than 300,000 in the United States, a crisis exacerbated by the reckless spread of falsehoods.
PolitiFact’s 2020 Lie of the Year: claims that deny, downplay or disinform about COVID-19.
‘I always wanted to play it down’
On Feb. 7, Trump leveled with book author Bob Woodward about the dangers of the new virus that was spreading across the world, originating in central China. He told the legendary reporter that the virus was airborne, tricky and “more deadly than even your strenuous flus.”
Trump told the public something else. OnFeb. 26, the president appeared with his coronavirus task force in the crowded White House briefing room. A reporter asked if he was telling healthy Americans not to change their behavior.
“Wash your hands, stay clean. You don’t have to necessarily grab every handrail unless you have to,” he said, the room chuckling. “I mean, view this the same as the flu.”
Three weeks later, March 19, he acknowledged to Woodward: “To be honest with you, I wanted to always play it down. I still like playing it down. Because I don’t want to create a panic.”
His acolytes in politics and the media were on the same page. Rush Limbaugh told his audience of about 15 million on Feb. 24 that coronavirus was being weaponized against Trump when it was just “the common cold, folks.” That’s wrong — even in the early weeks, it was clear the virus had a higher fatality rate than the common cold, with worse potential side effects, too.
As the virus was spreading, so was the message to downplay it.
“There are lots of sources of misinformation, and there are lots of elected officials besides Trump that have not taken the virus seriously or promoted misinformation,” said Brendan Nyhan, a government professor at Dartmouth College. “It’s not solely a Trump story — and it’s important to not take everyone else’s role out of the narrative.”
The skeptics cited Centers for Disease Control and Prevention data to claim that only 6% of COVID-19 deaths could actually be attributed to the virus. On Aug. 24, BlazeTV host Steve Deace amplified it on Facebook.
“Here’s the percentage of people who died OF or FROM Covid with no underlying comorbidity,” he said to his 120,000 followers. “According to CDC, that is just 6% of the deaths WITH Covid so far.”
That misrepresented the reality of coronavirus deaths. The CDC had always said people with underlying health problems — comorbidities — were most vulnerable if they caught COVID-19. The report was noting that 6% died even without being at obvious risk.
But for those skeptical of COVID-19, the narrative confirmed their beliefs. Facebook users copied and pasted language from influencers like Amiri King, who had 2.2 million Facebook followers before he was banned. The Gateway Pundit called it a “SHOCK REPORT.”
“I saw a statistic come out the other day, talking about only 6% of the people actually died from COVID, which is very interesting — that they died from other reasons,” Trump told Fox News host Laura Ingraham on Sept. 1.
Fauci, director of the National Institute of Allergy and Infectious Diseases, addressed the claim on “Good Morning America” the same day.
“The point that the CDC was trying to make was that a certain percentage of them had nothing else but just COVID,” he said. “That does not mean that someone who has hypertension or diabetes who dies of COVID didn’t die of COVID-19 — they did.”
Trump retweeted the message from an account that sported the slogans and symbols of QAnon, a conspiracy movement that claims Democrats and Hollywood elites are members of an underground pedophilia ring.
False information moved between social media, Trump and TV, creating its own feedback loop.
“It’s an echo effect of sorts, where Donald Trump is certainly looking for information that resonates with his audiences and that supports his political objectives. And his audiences are looking to be amplified, so they’re incentivized to get him their information,” said Kate Starbird, an associate professor and misinformation expert at the University of Washington.Weakening the armor: misleading on masks
At the start of the pandemic, the CDC told healthy people not to wear masks, saying they were needed for health care providers on the frontlines. But on April 3 the agency changed its guidelines, saying every American should wear non-medical cloth masks in public.
Trump announced the CDC’s guidance, then gutted it.
“So it’s voluntary. You don’t have to do it. They suggested for a period of time, but this is voluntary,” Trump said at a press briefing. “I don’t think I’m going to be doing it.”
Rather than an advance in best practices on coronavirus prevention, face masks turned into a dividing line between Trump’s political calculations and his decision-making as president. Americans didn’t see Trump wearing a mask until a July visit to Walter Reed National Military Medical Center.
In September, the CDC reported a correlation between people who went to bars and restaurants, where masks can’t consistently be worn, and positive COVID-19 test results. Bloggers and skeptical news outlets countered with a misleading report about masks.
On Oct. 13, the story landed on Fox News’ flagship show, “Tucker Carlson Tonight.” During the show, Carlson claimed “almost everyone — 85% — who got the coronavirus in July was wearing a mask.”
“So clearly (wearing a mask) doesn’t work the way they tell us it works,” Carlson said.
That’s wrong, and it misrepresented a small sample of people who tested positive. Public health officials and infectious disease experts have been consistent since April in saying that face masks are among the best ways to prevent the spread of COVID-19.
But two days later, Trump repeated the 85% stat during a rally and at a town hall with NBC’s Savannah Guthrie.
“I tell people, wear masks,” he said at the town hall. “But just the other day, they came out with a statement that 85% of the people that wear masks catch it.”
The assault on hospitals
On March 24, registered nurse Melissa Steiner worked her first shift in the new COVID-19 ICU of her southeast Michigan hospital. After her 13-hour day caring for two critically ill patients on ventilators, she posted a tearful video.
“Honestly, guys, it felt like I was working in a war zone,” Steiner said. “(I was) completely isolated from my team members, limited resources, limited supplies, limited responses from physicians because they’re just as overwhelmed.”
“I’m already breaking, so for f—’s sake, people, please take this seriously. This is so bad.”
Steiner’s post was one of manyemotionalpleas offered by overwhelmed hospital workers last spring urging people to take the threat seriously. The denialists mounted a counter offensive.
On March 28, Todd Starnes, a conservative radio host and commentator, tweeted a video from outside Brooklyn Hospital Center. There were few people or cars in sight.
“This is the ‘war zone’ outside the hospital in my Brooklyn neighborhood,” Starnes said sarcastically. The video racked up more than 1.5 million views.
Starnes’ video was one of the first examples of #FilmYourHospital, a conspiratorial social media trend that pushed back on the idea that hospitals had been strained by a rapid influx of coronavirus patients.
Several internet personalities asked people to go out and shoot their own videos. The result: a series of user-generated clips taken outside hospitals, where the response to the pandemic was not easily seen. Over the course of a week, #FilmYourHospital videos were uploaded to YouTube and posted tens of thousands of times on Twitter and Facebook.
Nearly two weeks and more than 10,000 deaths later, Fox News featured a guest who opened a new misinformation assault on hospitals.
Dr. Scott Jensen, a Minnesota physician and Republican state senator, told Ingraham that, because hospitals were receiving more money for COVID-19 patients on Medicare — a result of a coronavirus stimulus bill — they were overcounting COVID-19 cases. He had no proof of fraud, but the cynical story took off.
Trump used the false report on the campaign trail to continue to minimize the death toll.
“Our doctors get more money if somebody dies from COVID,” Trump told supporters at a rally in Waterford, Mich., Oct. 30. “You know that, right? I mean, our doctors are very smart people. So what they do is they say, ‘I’m sorry, but, you know, everybody dies of COVID.’”
The real fake news: The Plandemic
The most viral disinformation of the pandemic was styled to look like it had the blessing of people Americans trust: scientists and doctors.
In a 26-minute video called “Plandemic: The Hidden Agenda Behind COVID-19,” a former scientist at the National Cancer Institute claimed that the virus was manipulated in a lab, hydroxychloroquine is effective against coronaviruses, and face masks make people sick.
Judy Mikovits’ conspiracies received more than 8 million views in May thanks in part to the online outrage machine — anti-vaccine activists, anti-lockdown groups and QAnon supporters — that push disinformation into the mainstream. The video was circulated in a coordinated effort to promote Mikovits’ book release.
A couple of months later, a similar effort propelled another video of fact-averse doctors to millions of people in only a few hours.
On July 27, Breitbart publisheda clipof a press conference hosted by a group called America’s Frontline Doctors in front of the U.S. Supreme Court. Looking authoritative in white lab coats, these doctors discouraged mask wearing and falsely said there was already a cure in hydroxychloroquine, a drug used to treat rheumatoid arthritis and lupus.
Trump, who had been talking up the drug since March and claimed to be taking it himself as a preventive measure in May, retweeted clips of the event before Twitter removed them as misinformation about COVID-19. He defended the “very respected doctors” in a July 28 press conference.
When Olga Lucia Torres, a lecturer at Columbia University, heard Trump touting the drug in March, she knew it didn’t bode well for her own prescription. Sure enough, the misinformation led to a run on hydroxychloroquine, creating a shortage for Americans like her who needed the drug for chronic conditions.
A lupus patient, she went to her local pharmacy to request a 90-day supply of the medication. But she was told they were only granting partial refills. It took her three weeks to get her medication through the mail.
“What about all the people who were silenced and just lost access to their staple medication because people ran to their doctors and begged to take it?” Torres said.No sickbed conversion
On Sept. 26, Trump hosted a Rose Garden ceremony to announce his nominee to replace the late Ruth Bader Ginsburg on the U.S. Supreme Court. More than 150 people attended the event introducing Amy Coney Barrett. Few wore masks, and the chairs weren’t spaced out.
In the weeks after, more than two dozen people close to Trump and the White House became infected with COVID-19. Early Oct. 2, Trump announced his positive test.
Those hoping the experience and Trump’s successful treatment at Walter Reed might inform his view of the coronavirus were disappointed.
Trump snapped back into minimizing the threat during his first moments back at the White House. He yanked off his mask and recorded a video.
“Don’t let it dominate you. Don’t be afraid of it,” he said, describing experimental and out-of-reach therapies he received. “You’re going to beat it.”
In Trump’s telling, his hospitalization was not the product of poor judgment about large gatherings like the Rose Garden event, but the consequence of leading with bravery. Plus, now, he claimed, he was immune from the virus.
On the morning after he returned from Walter Reed, Trump tweeted a seasonal flu death count of 100,000 lives and added that COVID-19 was “far less lethal” for most populations. More false claims at odds with data — the U.S. average for flu deaths over the past decade is 36,000, and experts said COVID-19 is more deadly for each age group over 30.
When Trump left the hospital, the U.S. death toll from COVID-19 was more than 200,000. Today it is more than 300,000. Meanwhile, this month the president has gone ahead with a series of indoor holiday parties.
The vaccine war
The vaccine disinformation campaign started in the spring but is still underway.
In April, blogs and social media users falsely claimed Democrats and powerful figures like Bill Gates wanted to use microchips to track which Americans had been vaccinated for the coronavirus. Now, false claims are taking aim at vaccines developed by Pfizer and BioNTech and other companies.
A blogger claimed Pfizer’s head of research said the coronavirus vaccine could cause female infertility. That’s false.
An alternative health website wrote that the vaccine could cause an array of life-threatening side effects, and that the FDA knew about it. The list included all possible — not confirmed— side effects.
Social media users speculated that the federal government would force Americans to receive the vaccine. Neither Trump nor President-elect Joe Biden has advocated for that, and the federal government doesn’t have the power to mandate vaccines, anyway.
As is often the case with disinformation, the strategy is to deliver it with a charade of certainty.
“People are anxious and scared right now,” said Dr. Seema Yasmin, director of research and education programs at the Stanford Health Communication Initiative. “They’re looking for a whole picture.”
Most polls have shown far from universal acceptance of vaccines, with only 50% to 70% of respondents willing to take the vaccine. Black and Hispanic Americans are even less likely to take it so far.
Meanwhile, the future course of the coronavirus in the U.S. depends on whether Americans take public health guidance to heart. The Institute for Health Metrics and Evaluation projected that, without mask mandates or a rapid vaccine rollout, the death toll could rise to more than 500,000 by April 2021.
“How can we come to terms with all that when people are living in separate informational realities?” Starbird said.