The estimated costs for treating COVID-19 could add up as much as $547 billion for private insurers from 2020 to 2021 depending on the rate of infection, an updated report found.
The report, released Monday from consulting firm Wakely and commissioned by insurance lobbying group America’s Health Insurance Plans (AHIP), looks at the utilization of medical services associated with a COVID-19 infection and the costs for such services. The analysis is restricted to insurers operating in commercial, Medicare Advantage and Medicaid managed care markets.
Wakely estimates that the pandemic could cost insurers between $30 billion and $547 billion.
The report explores the costs of COVID-19 based on a series of potential infection rates, which represent the total population infected. The study modeled infection rates based on 10%, 20% and 60%, while acknowledging that the true infection rate could be far lower.
Wakely then looked at the total costs the plan is liable to cover based on each infection rate.
A 10% rate would lead to a total cost of $30 billion to $92 billion from 2020 to 2021, and a rate of 20% would be $60 billion to $182 billion.
But an infection rate of 60% would cost insurers the greatest, with a range of $180 billion to $547 billion.
“We assume that a higher volume of COVID related services will be incurred in 2020 and lower volume in 2021, distributing approximately 75% of the total services to 2020 and 25% to 2021,” the study said.
Wakely notes it did not model any long-term costs for treating people recovering from COVID-19 infections.
The firm also didn’t factor in vaccine mitigation in 2021 nor a scenario in which large-scale infections occur throughout 2021.
While private insurers have waived cost-sharing for COVID-19 treatments, it remains unclear how long the waivers will last. Anthem and Molina announced Monday they will extend their cost-sharing waivers through the rest of 2020.
The report is an update to an earlier one distributed by Wakely back in March at the onset of the pandemic. That report pegged the total COVID-19 costs between $56 billion and $556 billion.
The main reason for the decline is Wakely factored in deferred care due to the pandemic.
Wakely also reduced the overall assumed rate of hospitalizations for COVID-19-infected individuals to align with more recent studies. But the estimated unit cost for a hospital admission also increased, based on survey data from AHIP members.
People have been putting off necessary care for fear of going to a doctor’s office, and hospital systems have canceled or postponed elective surgical procedures for months.
Hospitals have slowly started to resume elective procedures, but only after installing stringent requirements on cleaning and testing.
Insurers are bracing for a wave of healthcare utilization some time later this year or in 2021 to deal with this pent-up demand.
The deferred care costs would differ based on the infection rate of the virus.
“We assumed, particularly for higher infection rate scenarios, that there may be limited capacity to make up care in 2021,” the report said.
Banner Health warned of a major spike of COVID-19 cases over the past few weeks in Arizona as the state opened back up and eased social distancing guidelines.
Arizona’s COVID-19 hospitalizations are rapidly increasing and raising potential capacity concerns, the system said.
“As of June 4, there were 1,234 hospitalized COVID-19 patients,” the system said in a statement. “About 50% of those patients are hospitalized in Banner Health facilities.”
Banner officials said its ICUs have gotten very busy, and the system has been transferring patients and resources to avoid putting stress on one particular hospital. Banner Health operates 28 hospitals across six states, including several hospitals in Arizona. The health system’s update comes as other hospital systems are eyeing a potential resurgence of COVID-19 cases as states reopen their economies after months of stay-at-home orders.
“If these trends continue, Banner will soon need to exercise surge planning and flex up to 125% bed capacity,” the system warned.
The number of Banner Health patients in Arizona on a ventilator has also increased over the past few weeks, from 41 on May 22 to nearly 120 on June 3.
The system also attributed the increase in COVID-19 cases to a relaxation of the state’s stay-at-home order, which expired May 15.
The cases started to spike two weeks after the end of the order, which is the likely incubation period for the virus.
Banner emphasized that the public needs to continue certain behaviors like wearing a mask in public and social distancing in order to ensure capacity isn’t overwhelmed.
Hospitals not only have to worry about the prospects of a second surge of the virus in the fall but also a wave of pent-up demand for healthcare services put off due to the pandemic.
Banner Health, like all health systems, canceled or postponed elective procedures at the onset of the pandemic back in March. But health systems are taking small steps to resume elective procedures.
Banner Health has also taken steps to preserve its personal protective equipment (PPE), which has been in short supply across the healthcare industry throughout the pandemic. Banner was one of 15 healthcare systems to buy a minority stake in PPE domestic manufacturer Prestige Ameritech in the hopes of shoring up a supply chain that is traditionally reliant on overseas manufacturers.
After months of lock down, hospitals are eager to get patients back for routine care and elective procedures.
An executive at a Palm Beach hospital stands between a box of surgical masks and a Purell dispenser.
“We understand you haven’t been inside our hospitals for some time,” she says to the camera. The executive is delivering her line for a promotional video intended to get people back to hospitals after almost three months of avoiding the place at all costs.
Moments later, the film crew records her chatting with a vascular surgeon in an idled operating room, who soothingly reassures that a hospital is the cleanest place to be outside your home. “The hospital is safer than the grocery store,” the doctor says.
The video published on YouTube in mid-May is part of a marketing campaign by Tenet Healthcare, which operates 65 hospitals and about 250 ambulatory surgery centers. It’s one attempt to solve a problem the entire health-care industry faces: Most patients vanished when Covid-19 swept the country.
Billions in Losses
Much of routine health care came to a halt in March as hospitals cleared space for an expected wave of Covid-19 patients and authorities ordered a halt to surgeries and other procedures that could be postponed. The decline in volume has clobbered hospital finances, with the industry estimating it is losing $50 billion a month.
Emergency visits dropped by 42% in four weeks in April compared to the same period last year, the Centers for Disease Control reported June 3. The number of U.S. patients getting hospital care dropped by more than half in late March and early April compared to 2019, according to data from Strata Decision Technology, which provides software to hospitals.
Some of that rebounded modestly in May as distancing rules eased, but hospital volume is nowhere near pre-Covid levels. With the pandemic ongoing and many states still confirming hundreds of new cases daily, patients are hesitating to rush back to hospitals.
“The main thing that really is a gating factor at this point is patient comfort,” Tenet President and Chief Operating Officer Saumya Sutaria said at a recent virtual conference with investors. Tenet declined interview requests.
Free Masks
To counter the public’s fears, hospitals publicize what they’re doing to keep patients safe. They’re handing out masks at the door and spacing out chairs in waiting rooms. They’re steering Covid-19 patients to dedicated sites and testing staff regularly.
Hospitals need to show patients that their facilities are safe. At Catholic hospital chain Trinity Health, that includes moving patients through “Covid-free” zones with separate doors, elevators and waiting areas.
“We can put all of the outreach and marketing in place, but it’s only as effective as the people who execute those strategies,” said Julie Spencer Washington, Trinity’s chief marketing and communications officer.
The question for the entire industry is how quickly patients come back. The answer will depend on a constellation of related variables, including how reluctant people are to resume care, and the course of the pandemic. Future surges could force hospitals to shut down regular care again — and spook patients further.
Hospitals and doctors are going to have to do as much as they can as fast as they can until they can’t anymore,” said Lisa Bielamowicz, co-founder of consultancy Gist Healthcare.
Many patients, on the other hand, are in no rush. “They’re waiting and watching rather than pulling the trigger and going to see the doctor like they would have in the past,” Bielamowicz said.
The calculation for the health-care industry is different than for many other service businesses resuming operations. A hospital procedure or even a check-up is more intimate than a meal out.
For procedures that require in-patient rehab stints for recovery, the havoc Covid-19 has brought to nursing homes adds another layer of concern. “Those places seem like deathtraps now, so it’s much harder to bring back those patients because you need to find an alternative way for them to rehab,” Bielamowicz said.
And the biggest consumers of health care are the elderly and the chronically ill, the very people Covid-19 most threatens. “From personal discussions with my patients, the older and more co-morbidities that any individual has, the more nervous they are about returning,” said Shauna Gulley, chief clinical officer at Centura Health, which has hospitals in Colorado and Kansas.
Patients with serious ongoing needs like cancer treatment or emergencies like heart attacks and strokes have continued to get care. And many medical problems resolve on their own. The decline in those visits – for a migraine headache, for example – reduces providers’ revenue but may not harm patients in the long-term.
While people often go to the emergency room for needs better treated in other settings, now the concern is the opposite: That true medical emergencies will be neglected.
Ascension, the nation’s largest Catholic hospital chain, has purchased billboards that say “Don’t delay ER care.” On hospital websites and social media posts, Tenet facilities reminded patients that “Emergencies Can’t wait. We’re Open & Safe.”
Deferred Care
Doctors fear that some patients will defer needed care too long, allowing progressive conditions to deteriorate. Clinicians at Maimonides Medical Center in Brooklyn, New York, have seen patients arrive sicker because they didn’t come earlier, said Ken Gibbs, the hospital’s CEO.
“There are unmet needs, I think that’s clear,” he said. “And I think the data on that will emerge, but it will take time.”
Maimonides treated 471 Covid patients at the peak on April 9, Gibbs said, and still had about 100 in late May. The hospital has applied for a waiver from New York State to resume elective surgeries, which are still on hold in New York City.
Some hospitals are preparing for a lasting dent in their revenue. For years, health economists have pointed to waste in the health-care system, with the estimated cost of unnecessary treatments in the hundreds of billions of dollars. Covid-19 may demonstrate that patients are willing to forego some of that care or opt for more conservative treatment.
People who had delayed back surgeries, for example, may now decide that doing physical therapy at home is good enough, said Marvin O’Quinn, president and chief operating officer at CommonSpirit Health, a large Catholic hospital system.
“We’ve all talked about too much intervention in health care in the past,” he said. “I think we’ll see a new normal in terms of what patients want to do and what doctors want to do, and we will have to adjust to that.”
Preventing deaths from COVID-19 depends on people who get it seeking treatment – which also allows authorities to track down whom they came in contact with to reduce spread.
But, as the economic pain and joblessness caused by the statewide lockdowns continue to grow, more Americans are experiencing severe strains on their personal finances. This threatens our ability to contain the pandemic because those feeling the most financial stress are much less likely to seek medical care if they experience coronavirus symptoms, according to my analysis of a recent Federal Reserve survey.
The Fed conducts a survey of the economic health of U.S. households every quarter, most recently near the end of 2019. In April, it conducted a supplementary but similar survey to quickly gauge how people were handling the coronavirus crisis. Results of both surveys were released on May 14.
The Fed tries to measure financial stress in three key ways. Its surveys ask respondents if they are unable to pay all their monthly bills, couldn’t cover a US$400 emergency expense, or are “just getting by” or worse.
Even before the pandemic hit, the picture wasn’t pretty. In October, when the fourth-quarter survey was conducted, 42% of employed respondents reported fitting at least one of these descriptions, while over 8% said they fit all three. Those figures jumped to 72% and 20% for low-income workers.
But by April, tens of millions of people who had jobs in October lost them as most nonessential businesses across the U.S. either closed or reduced their services. The unemployment rate shot up to 14.7% that month – the highest since the Great Depression – and is expected to climb further when the May data are released on June 5.
The Fed’s April survey, however, paints an even broader picture of the economic impact of the pandemic. In that survey, about 28% of the previously employed respondents said they either lost their job, were being furloughed, had their hours cut or were taking unpaid leave. This has been financially devastating to many, with 68% of this group reporting one of the stresses listed above and 28% saying they were experiencing all three, regardless of income level.
Forgoing medical care
Separate questions in the surveys demonstrate just how strong the link is between financial and physical health.
The October survey also asks those respondents if they had skipped a doctor’s visit during the previous 12 months because of the cost. More than 20% of those who reported one of these financial stresses said they had, while almost 46% of those with all three said so.
In April, the Fed asked a more timely question: “If you got sick with symptoms of the coronavirus, would you try to contact a doctor?”
A third of those respondents who also said they’re experiencing all three financial stresses said “no.” This is especially significant because, unlike the October question, it describes a current, known threat, rather than referring to a previous medical issue of unknown severity. And the widely reported urgency and seriousness of the coronavirus suggests someone wouldn’t treat the decision to seek a doctor’s care or advice lightly.
Relieving the stress
That was back in April, less than a month into the coronavirus lockdowns. If the same questions were asked today, I believe the numbers would look a lot worse.
In the middle of a serious pandemic, we don’t want sick people avoiding treatment because they’re worried they won’t be able to put food on the table. This would likely worsen the spread of the coronavirus and make it a whole lot harder to contain.
As Congress debates additional measures to mitigate the economic and financial effects of the pandemic, it would be wise to keep in mind the connection between financial stress and individual decisions to seek medical care.
Insurers will be issuing a total of about $2.7 billion in refunds, estimates the Kaiser Family Foundation.
The COVID-19 pandemic’s postponement of elective surgeries and regular care has created a surplus in revenue for insurers due to lower spending.
Health plans are mandated to spend at least 80% of their revenues on medical care. When they make more than that, they have to give money back to the purchasers.
Insurers are doing this now, rather than later, according to the Advisory Board’s practice manager Rachel Sokol, who spoke during the company’s weekly meeting on the impact of COVID-19 to payers.
Insurers want to create immediate value for members, instead of waiting for 2021, she said.
“That’s why we’re seeing the premium discounts now,” Sokol said.
Among those insurers refunding money, UnitedHealthcare said it would provide more than $1.5 billion in initial assistance, including customer premium credits, because its members have been unable to access routine or planned care due to the COVID-19 pandemic.
UnitedHealthcare has seen a lower volume of medical care being delivered than it anticipated when it set premiums.
Commercial fully insured individual and employer customers will get credits ranging from 5% to 20% – depending upon the specific plan – which will be applied to premium billings in June.
WHY THIS MATTERS
Insurers are mandated to provide refunds, but also they want to motivate members to return for regular care, to prevent more costly and complex outcomes later.
While hospitals have taken a financial hit from COVID-19, the major health insurers have shown minimal impact.
In fact, insurers could see a benefit to earnings in 2020 as medical services decline, according to Moody’s Investors Service.
THE LARGER TREND
Under the Affordable Care Act, insurers are required to rebate some premiums to their customers if medical claims fall short of expectations, based on a three-year average of medical costs.
The Medical Loss Ratio of the Affordable Care Act requires insurance companies that cover individuals and small businesses to spend at least 80% of their premium income on healthcare claims and quality improvement, leaving the remaining 20% for administration, marketing, and profit.
The MLR threshold is higher for large group insured plans, which must spend at least 85% of premium dollars on healthcare and quality improvement, according to the Kaiser Family Foundation.
Insurers may either issue rebates in the form of a premium credit or a check payment and, in the case of people with employer coverage, the rebate may be shared between the employer and the employee, Kaiser said.
Using preliminary data reported by insurers to state regulators and compiled by Market Farrah Associates, Kaiser estimates that insurers will be issuing a total of about $2.7 billion across all markets – nearly doubling the previous record high of $1.4 billion last year.
A third of U.S. adults say their family couldn’t afford care in past year
One in four say care was deferred for a serious medical condition
Lower-income adults and Democrats most likely to report delayed care
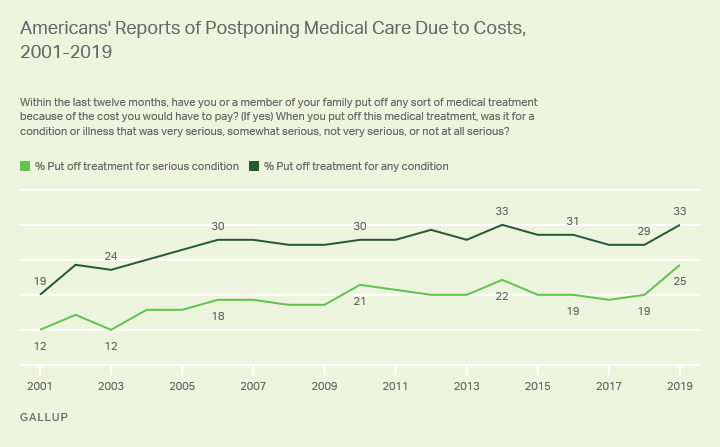
A record 25% of Americans say they or a family member put off treatment for a serious medical condition in the past year because of the cost, up from 19% a year ago and the highest in Gallup’s trend. Another 8% said they or a family member put off treatment for a less serious condition, bringing the total percentage of households delaying care due to costs to 33%, tying the high from 2014.
Gallup first asked this question in 1991, at which time 22% reported that they or a family member delayed care for any kind of condition, including 11% for a serious condition. The figures were similar in the next update in 2001, and Gallup has since asked this question annually as part of its Health and Healthcare poll. This year’s survey was conducted Nov. 1-14.
Americans’ reports of family members delaying any sort of medical treatment for cost reasons were lower in the early to mid-2000s when closer to a quarter reported the problem. Since 2006, the rate has averaged 30%.
The pattern is similar for the subset of Americans postponing medical treatment for a serious condition. The rate rose from 12% in 2001 to an average of 19% since 2006. However, the current 25% is the highest yet, exceeding the prior high-point of 22% recorded in 2014.
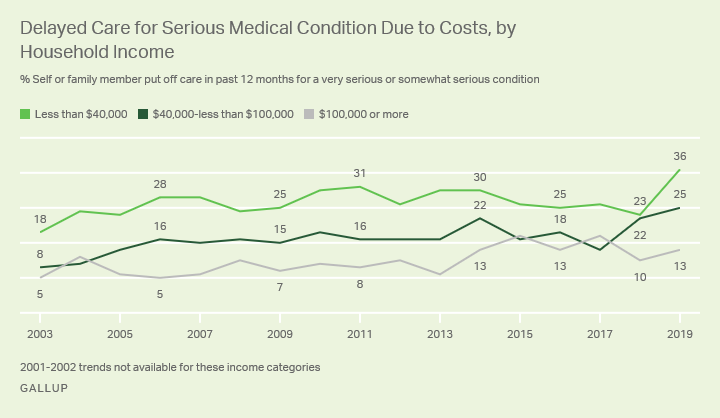
Income Gap Widens for Cost-Related Delays for Serious Conditions
Reports of delaying treatment for a serious condition jumped 13 percentage points in the past year to 36% among adults in households earning less than $40,000 per year while it was essentially flat (up a non statistically significant three points) among those in middle-income and higher-income households.
As a result of the spike in lower-income households this year, the gap between the top and bottom income groups for failure to seek treatment for a serious medical condition widened to 23 percentage points in 2019. The income gap had averaged 17 points in the early years of Barack Obama’s presidency, but narrowed to an average 11 points in the first few years after implementation of the ACA, from 2015 to 2018.
Delayed Care Up Most Among Those With Pre-Existing Conditions
Reports of delaying care for a serious condition due to costs are also up 13 points compared with last year among Americans who report they or another household member has a “pre-existing condition.”
At the same time, there has been virtually no change in the percentage of adults without pre-existing conditions in the household who delayed care for a serious health issue in the past year, currently 12% versus 11% in 2018.
Changes in health insurance coverage don’t appear to be the cause of the increase in delayed care as the percentage uninsured is 11% in the poll, within the 9% to 11% range seen each year since 2015. Also, the percentage delaying care has increased a similar proportion among those covered by private health insurance or Medicare/Medicaid as well as among the uninsured.
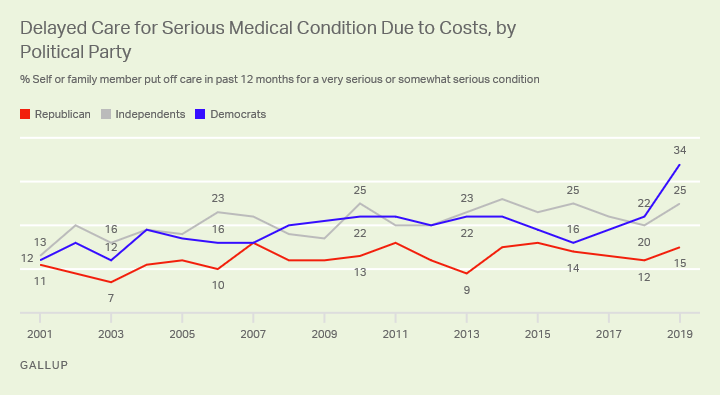
Recent Reports of Delayed Care May Have a Partisan Component
A cautionary note in the new findings is that most of the recent increase in reports that family members are delaying treatment for serious conditions has occurred among self-identified Democrats. This is up 12 points since 2018 among Democrats, compared with three- and five-point increases among Republicans and independents, respectively.
Whether these gaps are indicative of real differences in the severity of medical and financial problems faced by Democrats compared with Republicans or Democrats’ greater propensity to perceive problems in these areas isn’t entirely clear. But it’s notable that the partisan gap on putting off care for serious medical treatment is currently the widest it’s been in two decades.
Implications
Since 2001, Gallup has tracked a near 50% increase in the percentage of Americans saying that they or a family member chose not to get medical care because of the costs they would have to pay. Such delays in medical treatment, whether for injuries, illnesses or chronic conditions, can have significant implications for the economy and healthcare system, but also the political climate.
One indicator of the stress that delayed care can put on the healthcare system is the use of emergency departments. According to the American Hospital Association, patient visits to emergency departments in community hospitals increased 19% between 2001 and 2016 and has likely climbed to over 20% by today. While that may reflect many factors, including the aging of the population and the number of Americans living in close proximity to hospitals, it may also be indicative of a greater need for emergency care due to lack of routine care.
While most of the increase Gallup sees in delayed treatment occurred over a decade ago, the sharp increase in the past year, particularly among Democrats, suggests that healthcare costs could be a more potent political issue than previously seen. Presidential candidates who acknowledge the problem and propose solutions to address it may find a receptive ear among voters.
From an economic perspective, delayed care can have a range of negative effects, including reduced workplace productivity in the short-term, and increased healthcare costs and in the long-term — costs that ultimately burden the federal budget which has ripple effects on the economy.