If you decided to read the names of every American who is known to have died of covid-19, the disease caused by the novel coronavirus, at a rate of one per second starting at 5 p.m. Tuesday, you would not finish until a bit after 10 a.m. Saturday. Except, of course, that’s only including the deaths known as of writing; by then, we can expect 8,000 more deaths, pushing the recitation past noon.
Preliminary federal figures indicate that more than 3.2 million Americans will die over the course of 2020, the highest figure on record. It’s just a bit shy of 1 percent of the total population as of July 1, and about 1 in 10 of those deaths will be a result of covid-19.
That’s the primary context in which any discussion about how the pandemic has affected the United States should occur. Secondarily, we should consider how the number of new coronavirus infections correlates to that figure. At the moment, nearly two people are dying of covid-19 each minute, a function of a massive surge in the number of new infections that began in mid-September.
The surge and the deaths are inextricable. For months, the number of new deaths on any given day has been about 1.8 percent of new cases several weeks prior. Allowing the virus to spread wildly means allowing more Americans to die.
In an opinion piece for the Wall Street Journal, one of the architects of the decision to let the virus spread, former White House adviser Scott Atlas, blames the scale of the pandemic on the media. It’s the “politicization” of the virus, he argues, that has led to the dire outcomes we see, and that’s largely due to “media distortion.”
It’s hard to overstate both how dishonest Atlas’s argument is and how ironic it is that he should point the blame elsewhere. He makes false assertions about where states have been successful and suggests that mitigation efforts that weren’t 100 percent effective shouldn’t be used. He boasts that the effort to combat the spread of the virus was left to states — which is precisely the criticism aimed at President Trump’s administration. When Trump (and Atlas) undercut efforts to slow the spread of the virus, Trump supporters — including state leaders — picked up on that approach, contributing to the current spread.
Trump and Atlas shared the view that allowing the virus to spread was beneficial, as doing so increased population immunity. That another result would be surging deaths was met with a shrug or silence.
At the end of March, Trump offered one of his only forceful endorsements of slowing the spread of the virus. Having been presented with research indicating that as many as 2.2 million Americans would die of the virus if no effort was taken to limit its spread, he endorsed stay-at-home measures aimed at preventing new infections. His team suggested that implementing such mitigation efforts would keep the death toll under 240,000, with the added benefit of preventing hospitals from being overwhelmed.
This was one of Atlas’s arguments, too: Let the virus spread but backstop hospitals to prevent them from being flooded. The government accomplished the first goal, at least.
So we’ve raced past the 240,000-death mark, passing 300,000 deaths this month.
It’s important to remember, too, how often Trump himself promised this wasn’t going to be the country’s future. As the virus was spreading without detection — in part thanks to the Centers for Disease Control and Prevention’s failure to develop a working test — Trump repeatedly downplayed how bad things would get. There were thousands of deaths around the world, he noted in early March, but less than a dozen in the United States. He compared the coronavirus to the seasonal flu and to the H1N1 pandemic in 2009, an event that had the politically useful characteristic of having occurred while Trump’s eventual opponent in the presidential election was vice president.
Over and over, Trump predicted a high-water mark for coronavirus deaths. Over and over, the country surged past his predictions. As the election approached, he began simply comparing the death toll to that 2.2-million-death figure he’d first introduced in March.
The United States will not reach 2.2 million coronavirus deaths over the course of the pandemic. We probably won’t reach 500,000, assuming that the national vaccination effort — the far-safer way to spread immunity — progresses without significant problems.
Right now, though, thousands of people are dying every day and tens of thousands more are on an inevitable path to the same result. More robust efforts to prevent new infections could have reduced these numbers, as robust efforts did elsewhere (contrary to Atlas’s theories). A consistent, forceful message from a president whose base is devoutly supportive of him would unquestionably have reshaped the virus’s spread. Had Trump embraced the expertise of government virologists, instead of a radiologist he saw on Fox News, it would have perhaps pushed the curve depicting the number of deaths each day back down instead of driving it higher.
This was the deadliest year in American history. Perhaps it would inevitably have been, given the size of the population (particularly the elderly population) and the emergence of covid-19. But it unquestionably didn’t have to be as deadly as it was.
An estimated 803,000 people applied for unemployment aid for the first time last week, the Labor Department said Wednesday, showing the economy’s persistent weakness as new drama swirls over Washington’s response to the crisis. The figure was a slight decrease from the previous week but still much higher than normal.
The new Labor Department data show how weak the economy is, particularly the labor market. The surge in new coronavirus cases and deaths in the past few months has cooled the partial economic recovery from the summer.
Retail sales have weakened, and hiring has slowed markedly. The travel and tourism industries have not recovered much of the business lost since March, and thousands of companies — particularly restaurants and bars — have closed. U.S. household spending slipped in November, marking the first drop since April.
After months of stop-and-start negotiations, the bipartisan stimulus package finally offered some hope for households and businesses fighting to make it through the winter.
If Trump does not sign the bill, up to 14 million Americans would lose unemployment aid after Christmas. An eviction moratorium will expire at the end of the year, and $25 billion in emergency rental assistance will not get out the door. Billions of dollars for nutrition assistance, aid for small businesses, child care, transportation services and more will be in jeopardy, and the government will shut down on Dec. 29.
Trump did not play much of a role in the economic relief talks that resulted in Congress passing the $900 billion stimulus package. In the video Trump posted Tuesday night, his main complaint was that he wanted the $600 stimulus checks in the package to be increased to $2,000. This would add $370 billion to the measure.
Democrats quickly rallied around Trump’s demand, and House Speaker Nancy Pelosi (D-Calif.) plans to try to hold a vote on it as soon as Thursday. But it could be virtually impossible to pass such a measure through Congress with unanimous support, leaving the entire bill’s future uncertain.
The stimulus package would extend unemployment benefits of up to $300 per week, beginning as soon as Dec. 27 and run at least through mid-March. The measure also would extend Pandemic Unemployment Assistance — which targets part-time and gig workers who did not qualify for state unemployment insurance benefits — for 11 weeks.
Wednesday’s data showed nearly 400,000 new claims for the Pandemic Unemployment Assistance program.
Rare words from an incoming president: “Our darkest days in the battle against COVID are ahead of us, not behind us,” President-elect Biden warned this afternoon during remarks in Wilmington.
Why it matters:Biden is promising to tell America the truth, which includes the reality of many more horrific months, no matter who is in charge.
If we’re lucky, vaccinations will provide enough herd immunity to allow some normality by this summer or fall.
Another blunt reality: Most of the benefits in the $900 billion coronavirus rescue package expire months before America has any hope of being back to normal.
The $300 boost for unemployment benefits expires in March.
The new $284 billion round of the Paycheck Protection Program (PPP) is meant to last 3 months.
There’s no new funding earmarked for state and local governments.
The other side:There’s funding for schools and childcare and mass transit and vaccination distribution, which helps bail out the above from those obligations.
The entertainment sector got $15 billion, helping out theaters and museums and live entertainment venues.
$600 checks will start showing up next week for individuals making under $75,000 (phases out for incomes above that), with an extra $600 per child.
The bottom line: Georgia’s Jan. 5 Senate runoffs could be the difference between a big stimulus under Biden, or more trouble for parts of the U.S. hospitality sector.
An investment firm has bought more than 20 nursing homes during the coronavirus pandemic, leading to disruptions at multiple facilities that weakened care for vulnerable residents amid the worst health crisis in generations, interviews and documents show.
From April through July, the New Jersey-based Portopiccolo Group — which buys troubled nursing homes and tries to make them profitable — paid hundreds of millions of dollars to acquire facilities in Maryland, Virginia and elsewhere.
The purchases drew scant scrutiny from regulators despite poor safety records at dozens of the company’s other nursing homes, including hefty fines for infection-control lapses and shortages of staff.
Many of Portopiccolo’s existing facilities were struggling to contain outbreaks of the coronavirus when its leaders went seeking new properties, state health records show. At a Virginia nursing home, staff hosted a hallway dance party for residents in April, weeks after federal guidelines had cautioned against such events. Conditions were so bad at one North Carolina facility that it was placed on a federal watch list even after the Centers for Disease Control and Prevention dispatched a strike team to help.
At its new nursing homes in Maryland, Portopiccolo’s operating companies made major changes to insurance and time-off benefits, failed to buy enough supplies and protective equipment and asked some employees to keep working after testing positive for coronavirus, said 14 current and former employees from four of the eight facilities.
Many veteran staffers quit as a result of the changes, said the employees, most of whom spoke on the condition of anonymity because they feared reprisals. Those who remained found themselves tending to dozens of residents at a time, the employees said.
“It was hair on fire,” said Katrina Pearthree, a former social worker at two facilities purchased by Portopiccolo over the last 15 months. She resigned from her job after losing health insurance coverage and disagreeing with new managers on patient care.
Portopiccolo spokesman John Collins denied that caregiving suffered and said that while benefits changed, they remained competitive within the industry. The firm, he said, wants to fill the gap left by nursing home owners exiting the industry because of the pandemic.
“Our company was founded by people who share a passion for caring for the sick, elderly and forgotten,” Collins said in a statement. “Any attempts to characterize our work or the work of our teams differently is flat out wrong.”
Elder-care advocates say Portopiccolo’s record of fines at other facilities, and the timing of its acquisitions, should have raised red flags for regulators, especially as the virus decimated the country’s nursing home population.
But the Centers for Medicare and Medicaid Services (CMS), the main federal agency regulating nursing homes, said the only way it tracks ownership changes is when facilities report the information for Medicare enrollment.
President-elect Joe Biden has said he wants to increase federal oversight through mandatory audits of nursing home cost reports and ownership data. Typically, such monitoring has fallen to state regulators, said Charlene Harrington, a professor emerita of sociology and nursing at the University of California at San Francisco. But even before the coronavirus crisis, she said, most states did a poor job.
In Maryland, the commission that oversees changes in nursing home ownership said the sale of a facility requires little more than “timely notification.” Virginia officials said they don’t closely monitor such sales, either.
“Your history indicates what you’re going to do in the future,” said Richard Mollot, executive director of a national advocacy group called the Long Term Care Community Coalition. “There needs to be more oversight of these purchases.”
‘From bad to worse’
Portopiccolo founders Simcha Hyman, 31, and Naftali Zanziper, 38, bought their first nursing home in 2016 after selling their medical supplies company to a private equity firm. They have since purchased more than 70 facilities in nine states, including 18 in Virginia. The nursing homes are run by operating companies set up and financed by the firm, including Peak Healthcare, Accordius Health and Pelican Health — a trend first reported by the business magazine Barron’s.
For years, Hyman and Zanziper described Portopiccolo as a private equity firm. But that description, along with the group’s promise to swiftly turn “distressed assets” profitable, was removed from the Portopiccolo website in early December after inquiries from The Washington Post about the firm’s nursing home acquisitions.
Collins said the label “private equity” — which typically describes groups that raise funding from private investors — is inaccurate. He declined to explain why the group described itself that way for months, including in news releases, and still does on its LinkedIn page.
Atul Gupta, a professor of health-care management at the Wharton School at the University of Pennsylvania, said it is possible Portopiccolo is trying to rebrand itself because of the increasingly negative stigma tied to private equity groups — which have been criticized for slashing costs at nursing homes, then selling them off to new owners.Studies, by Gupta and others, show that private equity ownership correlates with declines in staffing and quality of care.
Collins declined to say how many facilities Portopiccolo owns, how many it has sold or how much the firm has profited. Neither Peak Healthcare nor Accordius Health responded to multiple requests for comment.
An analysis of federal data shows that nearly 70 percent of facilities Portopiccolo owned before the pandemic have Medicare ratings of one or two stars out of five — based on patient-care metrics such as staffing ratios and infection control.
Two Portopiccolo facilities last month were placed in a federal monitoring program for having “a history of serious quality issues”; two others were listed as candidates because of severe deficiencies. Prior to the pandemic, the firm’s facilities in North Carolina were fined more than $480,000 for violating state and federal rules, federal data shows.
One facility placed in the monitoring program was the Citadel Salisbury, a one-star nursing home in Salisbury, N.C., where more than 150 staff and residents have contracted the virus, according to state data. Employees and residents alleged in a lawsuit filed in Rowan County Superior Court that Portopiccolo, which bought the facility from Genesis HealthCare on Feb. 1, left the nursing home woefully unprepared for the pandemic.
Employees testified in sworn affidavits that managers from Accordius, the operating group, prohibited staff from wearing masks in March, saying that doing so would scare residents. Nurses sometimes had to care for more than 50 residents at a time, employees alleged.
The lawsuit asks that the facility be required to improve conditions or be closed or put under new ownership. But lawyers for Portopiccolo asserted that staffing and equipment have been adequate. Hyman, Zanziper and Accordius executives sought to downplay their role at the Citadel, claiming in a motion to dismiss that daily operations were the responsibility of staff on site.
At the same time, Portopiccolo sued the families in federal court, arguing that they had signed agreements that preclude litigation against the nursing home.
Such arbitration clauses have become increasingly common at for-profit nursing homes,studies show, and have been criticized by consumer advocates as well as lawmakers as a way for facilities to avoid accountability. Biden said he wants to restore an Obama-era ban on the practice that was overturned by the Trump administration.
In June, North Carolina officials identified a slew of violations at the Citadel that they said placed residents in “immediate jeopardy,” including a systemic failure to control infection and failing to inform the families of those who tested positive. Some found out their relatives had the virus from an emergency room physician. One man said he learned his aunt had died only when a funeral director called, asking what to do with her body.
Two hundred miles away in Virginia, staff shortages at Accordius Health in Harrisonburg were so dire before the pandemic that residents sometimes went days without showers, inspection records show.
“This place has gone from bad to worse,” one resident told an inspector. “They cut costs at our expense.”
After Accordius took over the facility in 2019, Ruth Simmers-Domzalski said, she noticed fewer staff members tending to her mother-in-law, Mary Domzalski, whose family twice found her lying on soiled bedsheets. On April 6, the facility held a hallway dance party where residents interacted without masks.
Domzalski, 88, attended. Three weeks later, she died of covid-19.
When asked about the event, Collins said the dance party did not conflict with federal guidelines at the time. CMS said on April 2 that all nursing home residents should cover their noses and mouths while interacting with staff; nearly a month before, it told facilities to cancel all group activities.
Tumultuous takeovers
Portopiccolo declined to say how many nursing homes it has bought during the pandemic, but The Post used CMS records to identify at least 22 facilities — eight in Maryland — that reported that Hyman and Zanziper had become owners since April.
Three of the Maryland facilities were bought from Genesis HealthCare, one of the largest skilled-nursing operators in the country. Amid plummeting occupancy rates and ballooning expenses, Genesis told stockholders this year that the firm would “improve its liquidity position” by selling off nearly two dozen of its roughly 400 nursing homes.
One was the Sligo Creek Center in Takoma Park, Md., where Pearthree, 59, worked part time as a social worker.
She had spent 18 years full time at another Genesis nursing home, the Fox Chase Rehabilitation Center in Silver Spring, leaving months after Portopiccolo bought it in 2019.
That sale was a “nightmare,” said Pearthree, recalling that new managers failed to secure local suppliers, leaving employees scrambling for medication and food. One afternoon, she said, staff members were unable to access digital patient records because Peak Healthcare had not put a new software system in place.
Less than a year after she left Fox Chase, Pearthree found herself facing another Portopiccolo takeover — this time amid a pandemic.
Again, the transition was chaotic. Peak did not actively recruit employees or offer them competitive packages prior to the takeover, leading to the departure of longtime staffers, including the administrator and director of nursing, said Pearthree and a senior Sligo Creek employee who spoke on the condition of anonymity because she feared reprisals. The former administrator and director of nursing did not respond to requests for comment.
Pearthree, a graduate student who worked 30 hours a week, was told she would have to increase her hours to keep her health insurance, she and Collins said.
Pearthree and the current employee also said Peak stopped providing hazard pay for contract employees and laid off a group of nonmedical staff Genesis had assembled to take temperatures and wipe down surfaces at the onset of the pandemic.
The facility has been cited twice by Maryand regulators since Peak took over, state inspection records show — in June for failing to test all residents and staff, and in August for failing to consistently inform family members of viral outbreaks.
Collins said staffing gaps were part of a nationwide shortage of nursing home workers and disputed the accounts from Pearthree and the current employee, saying supplies at both Sligo and Fox Chase were adequate and benefits were fair.
Eleven workers at three other Maryland nursing homes acquired by Portopiccolo during the pandemic said they lost paid time off and were offered more limited insurance packages. One worker who has asthma and high blood pressure said her bimonthly health insurance co-pay increased from $67 to $113 when Peak took over.
At Peak Healthcare Chestertown, on Maryland’s Eastern Shore, employees said the company offered a more limited benefits package than the facility’s previous owners, Autumn Lake, including less paid time off for new employees and no paid time off on major holidays.
The company scrimped on supplies, including cutlery, cleaning materials and clothing for residents, said employees at three facilities, who also spoke on the condition of anonymity out of fear of retribution.
Three employees at another facility said nurses have had to use hand soap to clean residents and rip up towels or bedsheets to dry them off.
“We risk our lives every day, and we don’t have proper supplies,” said one geriatric nursing assistant who brings her own gloves to work. “At what point do we put the patients first?”
Collins denied there were shortages, adding that at Chestertown, the budget for supplies had actually increased. He also denied that employees lost time off to which they were entitled, but said he could not address specific claims without knowing the names of the employees.
Reducing operating costs appears to be part of Portopiccolo’s business strategy, according to documents reviewed by The Post. In 2019, while acquiring three nursing homes in North Carolina, the group said it expected to save $360,000 by lowering expenses associated with employee benefits and insurance and $410,000 by cutting equipment and transportation costs. These measures, outlined in a mortgage loan contract, had allowed Portopiccolo to save more than $50 million across 37 facilities.
Collins said Portopiccolo has invested more than $6.7 million to purchase cleaning supplies and protective equipment since the start of this year. In comparison, Genesis, which operates about three times as many nursing homes, said that as of September, it had spent about $40 million more than normal on cleaning supplies and protective equipment.
Little government scrutiny
A recent study by the Long Term Care Community Coalition identified 15 states as having some good oversight practices for nursing home purchases, including requiring companies to disclose what other assets they own. Of the nine states in which Portopiccolo operates, none made the list.
“If your facilities in other states have very low staffing or a history of citations, you should not be allowed to purchase another one,” said Mollot, executive director of the coalition. “But states have a very hands-off approach to anything that happens outside their borders.”
Maryland Department of Health spokesman Charles Gischlar said the agency saw “no reason to change” the way it tracks shifts in nursing home ownership during the pandemic.
The Maryland Health Care Commission, another entity meant to oversee the sale of nursing homes, last year started asking prospective owners to affirm that they have not been convicted of a felony within the past 10 years or penalized more than $10 million because of their ownership of nursing homes.
But this requirement, which was designed “to keep out poor performers,” has not deterred a single transaction, said Paul Parker, a director at the commission.
For each facility that Hyman and Zanziper bought in Maryland, they declared to state regulators that they would not make substantive changes to services, staffing or bed ratios. State officials did not respond to questions asking how they ensured this would be true.
Gupta, the Wharton professor, said there should have been a moratorium on nursing home sales when the pandemic started because the changes that follow any acquisition can hamper a facility’s pandemic response.
But federal and state lawmakers never considered such a move.
“Nobody knew what was going on, nobody was in control,” Gupta said.
Joani Latimer, Virginia’s long-term-care ombudsman, said her office has been concerned by Portopiccolo’s pattern of buying facilities with low CMS ratings. Such facilities need more investment — not less — for conditions to turn around, she said.
“It’s not a process that you can just streamline to machine-like efficiency,” she said. “These are human needs with human challenges.”
Officials at the Virginia Department of Health, however, said they did not pay particular attention to Portopiccolo’s acquisition this year of Accordius Health at Courtland in Southampton County and Accordius Health at Waverly in Sussex County.
Such deals are “a business decision between the parties involved,” said Kimberly Beazley, director of the state Office of Licensure and Certification. “And we do not regulate business decisions made by facilities.”
Weeks with no hot water
Multiple employees at Portopiccolo-owned facilities, including one who worked in the kitchen at Chestertown, said their new managers had so much trouble filling staffing gaps this spring that employees were asked to work after learning they had the virus.
“It was a disaster,” said the Chestertown employee, who said she tested positive May 15 and declined when asked to come to work three days later. “People were still testing positive, and we were being asked to reapply for our jobs because this new company was coming in.”
Kent County Health Officer William Webb said local officials intervened that month after learning that a different employee at the facility who also had coronavirus was still working. “It was very concerning to me at the time, and we made sure to put a stop to it,” he said.
The facility’s water heater was broken from July to September, which meant there was no hot water for dishes or hand-washing. State inspectors fined the facility $730,000 for not fixing or reporting the problem, which they said posed “immediate jeopardy” to residents’ health. Collins said the firm is disputing the fine.
Webb said Peak’s decision not to promptly replace the water heater was “especially difficult” because the facility had seen scores of coronavirus cases and more than a dozen deaths in April and May. “If you’re in the business,” he said, “[you know] ample hot water is the core of any infection prevention program.”
When Peak took over managing the facility, roommates Patricia Sparkman, 82, and Brenda Middleton, 79, were isolated in their ground-floor room after testing positive for the virus.
Sparkman said in an interview that staff members left after the transition. Those who remained seemed less able to help, she said, including with basic tasks like bringing her water.
Middleton’s daughter, Tina Hurley, said the family moved Middleton a few months later to Peak Healthcare at Denton, about 30 miles away, so they could visit more frequently. But that facility had also been acquired by Portopiccolo on May 1.
Hurley said her mother is rarely checked on in Denton and has fallen several times while trying to get things for herself. At one point, she added, Middleton injured her leg but went without care from the facility’s doctor for days.
“I wouldn’t have brought her here if I knew how bad it would be,” Hurley said.
For Pearthree, the social worker at Sligo Creek, the breaking point came when she was asked to transfer back to Fox Chase in mid-May as director of social work. By then, Peak was operating both facilities.
She found residents she had known for years alone in their rooms, she said, confused and despondent in some cases. Relatives of those who died, she added, were given little information about how or when their loved ones had gotten sick.
When she raised concerns with managers, she said, she was brushed aside.
“The families felt betrayed by us,” Pearthree said. “And that was the part that overwhelmed me.” She sent a resignation letter in June.
Collins said Fox Chase administrators were unaware of her resignation and said Pearthree was terminated after she stopped coming to work. But the executive director of Fox Chase left Pearthree a voice mail on June 3 acknowledging her resignation and pleading with her to return.
“You do your job great and I like that,” the director said in the voice mail, which Pearthree shared with The Post.
Collins said that Portopiccolo leaders see their employees as “health care heroes.”
“We remain committed to putting care first,” he added.
Days before Thanksgiving, as all but one of the firm’s Maryland facilities reported new coronavirus outbreaks to the state, the firm closed on deals worth $37.7 million to acquire four more facilities in Florida.
Congressional leaders have reached an agreement on a $900 billion COVID-19 relief package and $1.4 trillion government funding deal with several healthcare provisions, according to Senate Majority Leader Mitch McConnell, R-Ky., and Minority Leader Chuck Schumer, D-N.Y.
Here are seven things to know about the relief aid and funding deal:
1. Congressional leaders have yet to release text of the COVID-19 legislation, but have shared a few key details on the measure, according to CNBC.Becker’s breaks down the information that has been released thus far.
2. The COVID-19 package includes $20 billion for the purchase of vaccines, about $9 billion for vaccine distribution and about $22 billion to help states with testing, tracing and other COVID-19 mitigation programs, according to Politico.
3. Lawmakers are also expected to include a provision changing how providers can use their relief grants. In particular, the bill is expected to allow hospitals to calculate lost revenue by comparing budgeted revenue for 2020. Hospitals have said this tweak will allow them to keep more funding.
4. The agreement also allocates $284 billion for a new round of Paycheck Protection Program loans.
5. The COVID-19 relief bill also provides$600 stimulus checks to Americans earning up to $75,000 per year and $600 for their children, according to NBC. It also provides a supplemental $300 per week in unemployment benefits.
6. The year-end spending bill includes a measure to ban surprise billing. Under the measure, hospitals and physicians would be banned from charging patients out-of-network costs their insurers would not cover. Instead, patients would only be required to pay their in-network cost-sharing amount when they see an out-of-network provider, according to The Hill.The agreement gives insurers 30 days to negotiate a payment on the outstanding bill. After that period, they can enter into arbitration to gain higher reimbursement.
7. Lawmakers plan to pass the relief bill and federal spending bill Dec. 21.
Applications for jobless benefits resumed their upward march last week as the worsening pandemic continued to take a toll on the economy.
More than 947,000 workers filed new claims for state unemployment benefits last week, the Labor Department said Thursday. That was up nearly 229,000 from the week before, reversing a one-week dip that many economists attributed to the Thanksgiving holiday. Applications have now risen three times in the last four weeks, and are up nearly a quarter-million since the first week of November.
On a seasonally adjusted basis, the week’s figure was 853,000, an increase of 137,000.
Nearly 428,000 applied for Pandemic Unemployment Assistance, a federal program that covers freelancers, self-employed workers and others who don’t qualify for regular state benefits.
Unemployment filings have fallen greatly since last spring, when as many as six million people a week applied for state benefits. But progress had stalled even before the recent increases, and with Covid-19 cases soaring and states reimposing restrictions on consumers and businesses, economists fear that layoffs could surge again.
“It’s very clear the third wave of the pandemic is causing businesses to have to lay people off and consumers to cut back spending,” said Daniel Zhao, senior economist for the career site Glassdoor. “It seems like we’re in for a rough winter economically.”
Jobless claims rose in nearly every state last week. In California, where the state has imposed strict new limits on many businesses, applications jumped by 47,000, more than reversing the state’s Thanksgiving-week decline.
The monthly jobs report released on Friday showed that hiring slowed sharply in early November and that some of the sectors most exposed to the pandemic, like restaurants and retailers, cut jobs for the first time since the spring. More up-to-date data from private sources suggests that the slowdown has continued or deepened since the November survey was conducted.
“Every month, we’re just seeing the pace of the recovery get slower and slower,” said AnnElizabeth Konkel, an economist with the job site Indeed. Now, she said, the question is, “Are we actually going to see it slide backward?”
Many economists say the recovery will continue to slow if the government does not provide more aid to households and businesses. After months of gridlock in Washington, prospects for a new round of federal help have grown in recent days, with congressional leaders from both parties signaling their openness to a compromise and the White House proposing its own $916 billion spending plan on Tuesday. But the two sides remain far apart on key issues.
The stakes are particularly high for jobless workers depending on federal programs that have expanded and extended unemployment benefits during the pandemic. Those programs expire later this month, potentially leaving millions of families with no income during what epidemiologists warn could be some of the pandemic’s worst months.
Despite taking a huge volume hit in Q2, most hospitals have managed to maintain positive operating margins—largely thanks to a $100B cash infusion from the federal government via the Coronavirus Aid, Relief and Economic Security (CARES) Act.
According to Kaufman Hall’s most recent National Hospital Flash Report, based on data from over 900 hospitals of all sizes nationwide, hospitals would have been operating at a significant loss without federal aid. As the graphic above shows, the average hospital operating margin without CARES Act relief funds would have been negative eight percent in April—and would still be in the red as of October, despite much of the cancelled elective business returning across the summer and early fall.
However, with the aid, hospitals operating margins only turned negative in April and May. When compared to the same time period last year, year-to-date (YTD) gross revenue is down almost five percent, though net patient service revenue per discharge is up—the result of longer lengths of stay, the 20 percent Medicare reimbursement bump for COVID-19 patients, and suspension of the two percent sequestration adjustment on Medicare fee-for-service payments. Yet hospital expenses per discharge are also up 13.5 percent, dampening profitability.
Though the CARES Act has been a stopgap solution for the vast majority of hospitals, a handful, most notably HCA Healthcare, have proactively returned the money. While motivations for doing so are varied, we’ve been hearing that the ever-changing reporting and spending requirements associated with CARES Act funding have many hospital leaders concerned about possible future claw-backs.
With COVID-19 hospitalizations now reaching record-breaking highs, potentially forcing another round of shut-downs, and with little movement on another round of federal relief, hospitals may be on their own for the time being—and the greatest hit to health system finances may still be yet to come.
Many hospitals are temporarily or permanently reducing the size of their workforce as they grapple with depleted revenues and the thorny question of when they can return to normal operating capacity. Here’s a tracker to follow the latest updates.
Hospitals across the country, financially battered as they face the dual challenges of sick COVID-19 patients and a precipitous decline in patient volume, are struggling to balance quickly shifting staffing needs. While some face and others brace for intense demand, many have announced furloughs of specialists and others that work in elective surgeries that have been drastically scaled back.
Thousands of healthcare workers at hospitals big and small have been asked not to return to work, and it’s still unclear how soon non-essential services will return. While some governors announce plans to reopen businesses, others have extended stay-at-home orders.
Most recent data from the U.S Bureau of Labor doesn’t cover the second half of March or early April, but during the first half of March, the healthcare industry shed 43,000 jobs — reversing a decade of growth in the sector. According to BLS data, the industry added 49,000 jobs in March 2019.
“Even our emergency room has seen a significant drop in patients coming in,” Sue Philips, an ICU nurse at Palomar Pomerado Health in Northern San Diego, told Healthcare Dive.
Phillips is a spokesperson with National Nurses United, the country’s largest nurses union.Palomar Health, which runs three medical centers in northern San Diego County, recently instituted 21-day temporary layoffs of 221 employees.
On April 28, Palomar announced that most of those layoffs were becoming permanent. The system laid off 5% of its workforce, eliminating 317 positions. Fifty of those employees were clinical RNs, mostly in part-time positions, and the rest spread across the organization ranging from clerical staff to technicians.
Due to a 50% decrease in patient volumes, Palomar lost $10 million in revenue in March alone, according to a statement. In April the system said it stands to lose $20 million or more.
“I’m an ICU nurse, so my job is pretty much protected,” Phillips said. “But you didn’t think you were expendable until you became expendable, and that’s a hard pill for nurses and caregivers to swallow.”
Congress has attempted to financially support struggling hospitals through ongoing coronavirus relief legislation, approving some $175 billion thus far. But without knowing what will come next, hospitals are attempting to remain nimble while reining in one of their most costly expenses — paying employees.
The following information is based on publicly reported data, along with interviews with hospital representatives and union members.
It’s not an exhaustive list, but features nonprofit and for-profit hospital systems that reported revenue above $10 billion in 2019. It also takes a look at smaller, more regionally based systems that have announced similar cutbacks.
Use the dropdown to find a company (Click on link above to access layoff tracker)
The U.S. economy added back the smallest number of jobs in seven months in November, as the labor market endured mounting pressure from the coronavirus pandemic while businesses wait for a vaccine to be distributed next year.
The U.S. Department of Labor released its monthly jobs report Friday morning at 8:30 a.m. ET. Here were the main results from the report, compared to Bloomberg consensus data as of Friday morning:
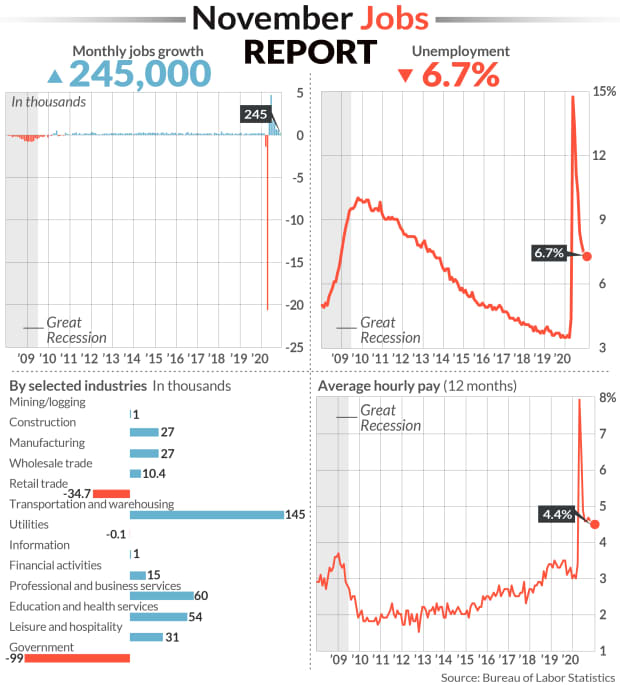
Change in non-farm payrolls: +245,000 vs. +460,000 expected and a revised +610,000 in October
Unemployment rate: 6.7% vs. 6.7% expected and 6.9% in October
Average Hourly Earnings month-over-month: 0.3% vs. +0.1% expected and +0.1% in October
Average Hourly Earnings year-over-year: 4.4% vs. +4.2% expected and a revised +4.4% in October
During November, a plethora of new stay-in-place measures and curfews swept the nation as COVID-19 cases, hospitalizations and deaths swelled to record levels. These renewed restrictions weighed on the rate of the recovery in the labor market, which had already been slowing after a record surge in rehiring followed the initial wave of lockdowns in the spring.
To that end, job gains in November sharply missed expectations. Non-farm payrolls grew by just 245,000 during the month for the smallest number since April’s record, virus-induced decline. October’s payroll gain was downwardly revised to 610,000 from the 638,000 reported earlier, while September’s gain was raised to 711,000 from 672,000.
A third straight month of declining government employment served as a drag on the headline payrolls figure, as another 93,000 temporary workers hired for the 2020 Census were let go.
In the private sector, retail trade industries shed nearly 35,000 jobs following a gain of 95,000 in October. Leisure and hospitality employers added just 31,000 jobs during November, declining by nearly 90% from October. And in goods-producing industries, manufacturing jobs rose by only 27,000 for the month, falling short of the 40,000 expected.
But a handful of other industries added more jobs in November from October: Transportation and warehousing jobs grew by 145,000 to more than double October’s advance, and growth in wholesale trade positions also doubled to 10,400.
November’s unemployment rate also improved just marginally to 6.7% from the 6.9% reported in October. While down from a pandemic-era high of 14.7% in April, the jobless rate remains nearly double that from before the pandemic.
Other employment reports this week underscored the decelerating trend. Private-sector hiring fell to the lowest level in four months in November, according to data tracked by ADP. New weekly jobless claims began rising again around the 12th of the month, when the Labor Department conducts its surveys for its monthly jobs report. And in the Federal Reserve’s November Beige Book, the central bank noted that nearly all districts reported rising employment, “but for most, the pace was slow, at best, and the recovery remained incomplete.”
The U.S. economy still has a ways to go before fully making up for the drop in payrolls induced by the pandemic.Even with a seventh straight month of net job gains, the economy remains about 9.8 million jobs short of its pre-pandemic level in February. The U.S. economy lost more than 22 million jobs between March and April.
And worryingly, the number of the long-term unemployed has kept climbing. Those classified as “permanent job losers” totaled 3.7 million in November, eclipsing the number of individuals on temporary layoff for the second time since the start of the pandemic. Permanent job losers have increased by 2.5 million since February, before the pandemic meaningfully hit the U.S. economy.
In Washington, congressional lawmakers have for months been at a stalemate over the size and scope of another stimulus package, which could help provide funds for businesses to help keep workers employed, and offer extended unemployment benefits for those the pandemic has kept out of work. Federal unemployment programs authorized under the CARES Act in the spring are poised to expire at the end of the month. These include the Pandemic Emergency Unemployment Compensation and Pandemic Unemployment Assistance programs, which together provide benefits for more than 13 million Americans.
“The only thing that matters about today’s NFP [non-farm payrolls] report is whether it increases the likelihood of a stimulus deal getting done during the lame duck session,” Peter Tchir, head of macro strategy for Academy Securities, said in an email Friday morning. “While the unemployment rate shrunk and wages ticked up nicely, the headline number dropped significantly, was well below average expectations, and included some downward revisions to last month (and upward revisions to 2 months ago) – all of which point to a less robust job market.”