Insurers and health systems across the U.S. have been at odds during the most recent cycle of contract negotiations, and terminated contracts are affecting thousands of patients.
As hospitals continue to recover financially from the COVID-19 pandemic and deal with higher supply costs and employee wages, many organizations have tightening margins and hope to negotiate higher rates with insurers as a result. Hospitals are also pointing to rising inflation as a reason for needing higher rates.
One recent example is Fort Lauderdale, Fla.-based Broward Health’s public breakup with UnitedHealthcare. Thousands of the insurer’s beneficiaries went out of network with Broward April 1 after the two sides failed to agree on a new contract. Broward reportedly asked UnitedHealthcare for a pay increase to the same level UnitedHealthcare pays other South Florida health systems.
UnitedHealthcare said Broward’s rate increase request would amount to 88 percent higher reimbursement for its providers in the next four years, which the insurer said was “unreasonable.” Negotiations continue, but patients are out of network in the meantime.
Blue Cross & Blue Shield of Mississippi and the University of Mississippi Medical Center let their contract expire April 1 after they failed to agree on pay rate increases, according to the Clarion Ledger. The medical center treated more than 50,000 patients in the 18 months before the contract expiration.
LouAnn Woodward, MD, vice chancellor for health affairs and dean of the medical center’s school of medicine, said the health system wants “fair reimbursement” from Blue Cross & Blue Shield to reinvest in its facilities and programs. The insurer said the medical center wanted a 30 percent overall rate increase, including a 50 percent increase for some services, according to the newspaper report.
Physician groups and surgery centers aren’t immune from insurer conflicts. Blue Cross Blue Shield of Illinois terminated its contract with Springfield (Ill.) Clinic late last year, knocking 100,000 beneficiaries out of network.
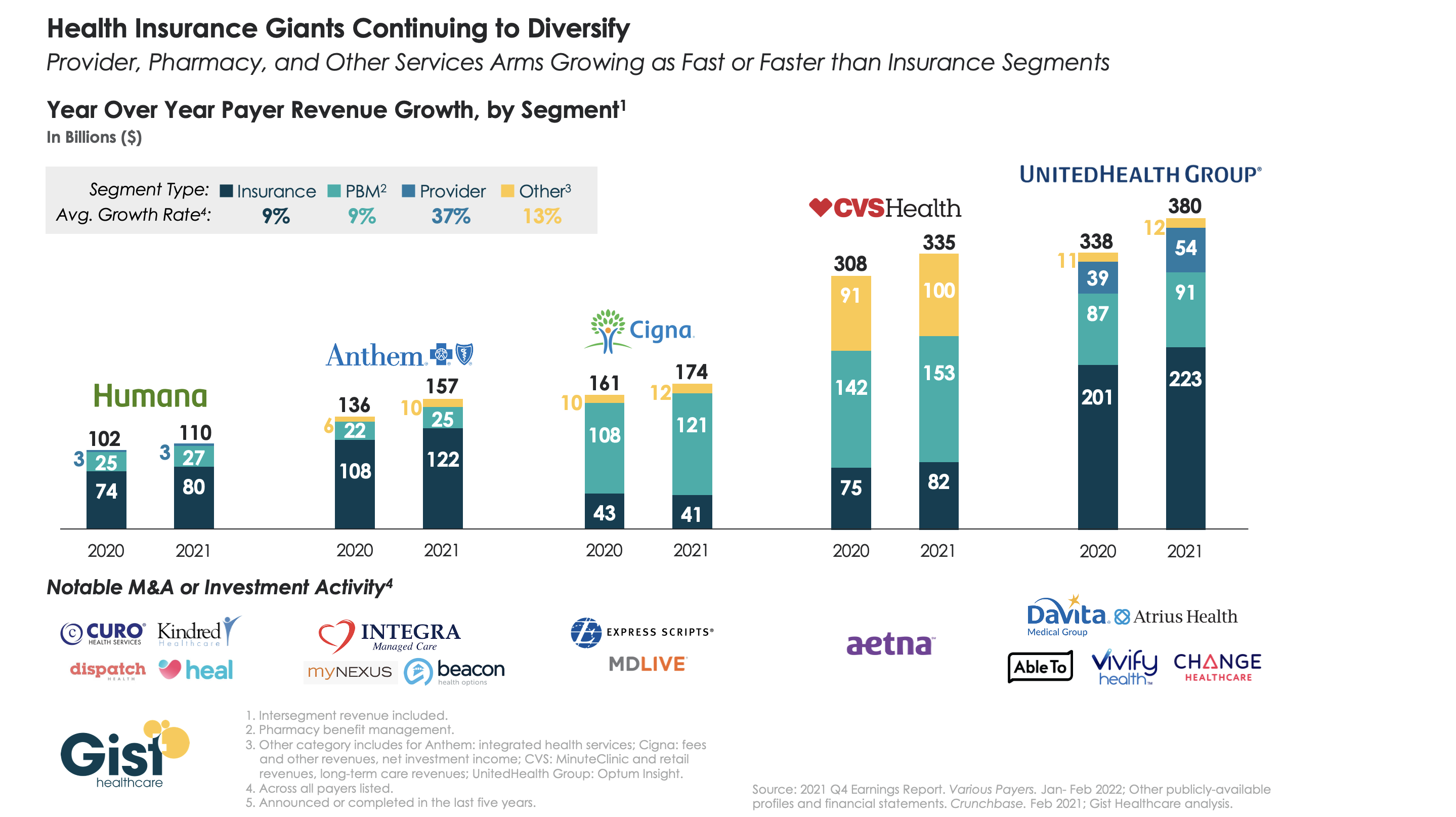
The largest health insurers are quickly becoming vertically integrated healthcare organizations that span the care and coverage continuum. While 2021 was a mixed year for these companies as healthcare volumes bounced back, their diversified portfolios helped cushion losses from higher claims.
The graphic above analyzes revenue growth by segment for the five largest insurers across the last two years. On averagethe insurance and pharmacy benefit management components of the companies grew at nine percent, while care delivery and integrated health services grew at much higher rates. UnitedHealth Group (UHG) and Anthem boasted the highest year-over-year revenue growth, driven by UHG’s Optum subsidiary and Anthem’s integrated health services.
Cigna and CVS Health each earned less than a quarter of their total revenue from their insurance arms lastyear. While Humana lags the others in topline revenue, it has assembled a robust portfolio of care delivery investments and partnerships, surpassed only by UHG.
As antitrust scrutiny on vertical integration increases (case in point: the DOJ is now challenging UHG’s acquisition of Change Healthcare), insurers will face the hard task of integrating their portfolio of service—and demonstrating that they deliver value to consumers and patients.
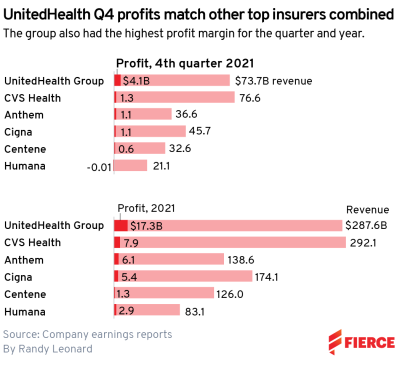
UnitedHealth Group was the most profitable payer in 2021, bringing in more than double the profit of itsnext-closest competitor with $17.3 billion in earnings.
CVS Health recorded the second-highest profit for the year among six major national insurers, earning $7.9 billion. CVS did bring in the highest revenue for the year, though, edging out UnitedHealth with $292.1 billion.
UHG reported $287.6 billion in revenue for 2021, according to the company’s earnings report.
Both healthcare giants expect to top $300 billion in revenue this year, according to their forecasts.
UnitedHealth was also the fourth quarter’s most profitable company, raking in $4.1 billion, which matched what its competitors earned combined, according to the filings.
UnitedHealth Group’s results represented significant growth over both the full-year and fourth quarter of 2020. According to its earnings report, this was driven in part by gains in Medicare Advantage and Medicaid at UnitedHealthcare as well as another quarter of double-digit growth at Optum.
CVS was also the next-highest earner in Q4, with $1.3 billion in profit on $76.6 billion in revenue. UHG was just behind on revenue with $73.7 billion.
CVS Health executives said that the retail business outperformed expectations in the fourth quarter amid increased demand for COVID-19 tests and booster shots.
The healthcare giant performed 32 million tests and 59 million vaccine doses over the course of the year, with 8 million tests and 20 million vaccinations reported in the fourth quarter alone.
While CVS and UnitedHealth duked it out for the top spot, all six of the big national payers were profitable for 2021, though Humana did post a $14 million loss for the fourth quarter.
Centene Corporation lands in sixth place for the year in profitability, bringing in $1.3 billion in profit on $126 billion in revenue. It also reported $599 million in profit for Q4.
Humana earned $2.9 billion for the year and $83.1 billion in revenue despite the Q4 loss, according to the company’s earnings report. Executives said the insurer braced for headwinds related to COVID-19 during the year and also saw disappointing growth in new Medicare Advantage members.
Anthem and Cigna fall in the middle of the pack, according to our review. They both reported about $1.1 billion in profit for Q4, though Cigna was ahead with $45.7 billion in revenue.
Anthemearned $6.1 billion in profit on $138.6 billion in revenue for the year, and executives shrugged off concerns about the Medicare Advantage market, saying its performance in open enrollment met expectations. In addition, it’s seeing growth at its in-house pharmacy benefit manager, IngenioRx, as it expands clientele.
A Florida physician was convicted Feb. 10 for his role in a healthcare fraud scheme that involved billing health insurance companies for $110 million in medically unnecessary services, according to the Justice Department.
Mark Agresti, MD, of Palm Beach, Fla., unlawfully billed insurers for $110 million of drug testing services that were medically unnecessary. The patients who received the unnecessary drug tests were residents of Good Decisions Sober Living in West Palm Beach. Dr. Agresti was the medical director of the facility, according to the Justice Department.
“Patients at GDSL were required to submit to excessive, medically unnecessary urine drug tests as a condition of residency approximately three or four times per week,” the Justice Department said. “These [urinalysis] drug tests cost as much as $6,000 to $9,000 per test.”
According to evidence presented at trial, Dr. Agresti also had Good Decisions Sober Living patients sent to his own medical practice to fraudulently bill for services.
Dr. Agresti was convicted of 11 counts of healthcare fraud and one count each of conspiracy to commit healthcare fraud and wire fraud. He is scheduled to be sentenced April 21.
Last week, we examined how the fast-growing Medicare Advantage (MA) market remains heavily concentrated among a handful of large carriers. But amid this concentration, consumers have more options than ever before, both in terms of carriers and plans, as shown in the graphic below.
The average MA enrollee can now choose from among 39 health plans offered by nine different payers, the majority of which feature $0 insurance premiums. An increasing number of plans also now offer a variety of non-medical benefits.
Landing an MA consumer soon after they become eligible is critical for carriers, as more than seven in 10 Medicare beneficiaries stick with the plan they have year after year. While this “stickiness” may suggest enrollees are satisfied with their current coverage, it also calls into question whether the MA marketplace is actually working as intended.
With another revenue boost to MA plans proposed for 2023, competition between plans—as well as consolidation among carriers—will continue to heat up, especially as the number of Medicare-eligible Americans will increase by nearly 50 percent over the next three decades.
The California Assembly is poised to vote on a bill Jan. 31 that aims to create a single-payer healthcare system in the state — the bill’s first major battle since a funding proposal for the program was introduced Jan. 6 — according to KTVU FOX 2.
The state’s plan to create a universal healthcare system involves two bills — AB 1400 and ACA 11 — that would implement and subsequently fund the program, dubbed CalCare. The Assembly is expected to only vote on AB 1400 on Jan. 31.
The Assembly must pass the bill Jan. 31 if it hopes to pass the single-payer framework bill by the end of the year. If the bill passes in the Assembly, it would then need approval in the Senate and from voters.
The plan is being met with public pressure that believesthe system would “create a new and exorbitantly expensive government bureaucracy.” Lawmaker opposition also largely focuses on the bill’s cost, which would be between $314 billion and $391 billion annually, according to KTVU. The bill’s funding counterpart, ACA 11, proposes to pay for it with a tax increase on businesses and high-earning individuals.
However, proponents argue that CalCare would cost less than the state’s current system, which equates to $517 billion when considering both taxes and household spending.
The second year of the pandemic did not dampen UnitedHealth Group’s finances, and the company actually surpassed its initial 2021 revenue and profit projections, Bob writes.
The big picture: UnitedHealth’s revenue has tripled from 2010 to 2021, and profit has almost quadrupled. The company continues to make more of its money from owning doctor groups and controlling pharmacy benefits instead of relying on health insurance.
We recently caught up with a health system chief clinical officer, who brought up some recent news about CVS. “I was really disappointed to hear that they’re going to start employing doctors,” he shared, referring to the company’s announcement earlier this month that it would begin to hire physicians to staff primary care practices in some stores. He said that as his system considered partnerships with payers and retailers, CVS stood out as less threatening compared to UnitedHealth Group and Humana, who both directly employ thousands of doctors: “Since they didn’t employ doctors, we saw CVS HealthHUBs as complementary access points, rather than directly competing for our patients.”
As CVS has integrated with Aetna, the company is aiming to expand its use of retail care sites to manage cost of care for beneficiaries. CEO Karen Lynch recently described plans to build a more expansive “super-clinic” platform targeted toward seniors, that will offer expanded diagnostics, chronic disease management, mental health and wellness, and a smaller retail footprint. The company hopes that these community-based care sites will boost Aetna’s Medicare Advantage (MA) enrollment, and it sees primary care physicians as central to that strategy.
It’s not surprising that CVS has decided to get into the physician business, as its primary retail pharmacy competitors have already moved in that direction. Last month, Walgreens announced a $5.2B investment to take a majority stake in VillageMD, with an eye to opening of 1,000 “Village Medical at Walgreens” primary care practices over the next five years. And while Walmart’s rollout of its Walmart Health clinics has been slower than initially announced, its expanded clinics, led by primary care doctors and featuring an expanded service profile including mental health, vision and dental care, have been well received by consumers. In many ways employing doctors makes more sense for CVS, given that the company has looked to expand into more complex care management, including home dialysis, drug infusion and post-operative care. And unlike Walmart or Walgreens, CVS already bears risk for nearly 3M Aetna MA members—and can immediately capture the cost savings from care management and directing patients to lower-cost servicesin its stores.
But does this latest move make CVS a greater competitive threat to health systems and physician groups? In the war for talent, yes. Retailer and insurer expansion into primary care will surely amp up competition for primary care physicians, as it already has for nurse practitioners. Having its own primary care doctors may make CVS more effective in managing care costs, but the company’s ultimate strategy remains unchanged: use its retail primary care sites to keep MA beneficiaries out of the hospital and other high-cost care settings.
Partnerships with CVS and other retailers and insurers present an opportunity for health systems to increase access points and expand their risk portfolios. But it’s likely that these types of partnerships are time-limited. In a consumer-driven healthcare market, answering the question of “Whose patient is it?” will be increasingly difficult, as both parties look to build long-term loyalty with consumers.
Oak Street Health, a value-based primary care network for adults on Medicare, is facing a Department of Justice inquiry into its relationships with third-party marketing agents and its provision of free transportation for members.
The DOJ is investigating whether Oak Street violated the False Claims Act, per a regulatory filing published Monday. On a call with investors Tuesday, management declined to provide additional information into the government’s request, saying it was too early to know for sure what exactly the agency is investigating but that they’re working to comply.
Otherwise, the provider had a generally solid third quarter with better-than-expected revenue and well-controlled medical costs, analysts said. Oak Street increased its full-year 2021 guidance following the results, which beat Wall Street expectations with topline revenue of $389 million, up 78% year over year and a quarterly record for the company.
Dive Insight:
The federal government is increasingly cracking down on alleged fraud, especially in the Medicare Advantage program. In privately run MA plans, CMS pays companies on a per-member basis, then adjusts payments based on the acuity or severity of their member’s health status, as supported by provider data like diagnostic codes. Generally, the sicker the member, the higher the plan’s reimbursement.
That’s led to allegations of plans hiking risk scores to overinflate members’ health needs, resulting in higher payments from CMS. Watchdogs have been finding higher incidence of fraud and abuse as the MA program becomes more popular, growing to cover more than 40% of all Medicare beneficiaries.
Oak Street isn’t a traditional plan itself, but enters into full-risk contracts with Medicare Advantage plans, and via CMS’ direct contracting program, in which it assumes full responsibility for patients’ medical expenses in exchange for a fixed per-member, per-month payment. The Chicago-based company is the latest target of a federal inquiry into whether it violated the False Claims Act.
According to the primary care company, the DOJ sent a civil investigative demand on Nov. 1 asking for information about Oak Street’s relationships with third-party marketers and transportation partners.
Oak Street does provide patients transportation to appointments when they need it and has various ways for finding new patients, including community partnerships, but it’s unclear what the DOJ is specifically investigating, CEO Mike Pykosz told investors.
“We have had no meaningful conversations with the government,” Pykosz said. “I’m not really sure what the link is.”
The CEO noted it’s not unusual for such inquiries to take months to resolve, particularly in the hyper-regulated healthcare industry, but said he wouldn’t speculate further.
A civil investigative demand is a form of administrative subpoena, and doesn’t denote any regulatory or legal action itself. However, it is used by the government to kick off investigating potential False Claims violations, and determine whether there’s sufficient evidence to warrant filing an action, according to the National Law Review.
Penalties for violating the act could range from $11,655 to $23,331 per violation, plus triple damages. Total penalties have resulted recently in some significant payouts from MA participants. Notably, in late August, integrated health system Sutter Health agreed to pay $90 million to settle whistleblower allegations of risk adjustment fraud, in the largest False Claims Act settlement against a hospital system in the MA program.
Analysts noted the inquiry, while in early stages, is a point of concern for Oak Street’s future stock performance.
“This creates a new potential risk factor that we are unlikely to get clarity on for some time,” SVB Leerink analyst Whit Mayo wrote in a note.
Oak Street, which also provides services to patients with a range of insurance options, had an otherwise solid quarter, eclipsing $1 billion of year-to-date revenue for the first time in the company’s history.
The highly infectious delta variant did contribute to higher expenses, as it has with other providers.
Oak Street reported $15 million in costs from COVID-19 admissions in the first half of the year, and another $10 million in the third quarter. COVID-19-related expenses surged in the latter half of August and continued into September, but tailed off early into the fourth quarter, CFO Tim Cook said.
The majority of Oak Street’s patients are in northern U.S. markets, however, which experienced coronavirus surges last year during the winter as more people stayed indoors.
“We will see what happens in November and December,” Cook said. “While COVID costs are going to be lower in Q4, unfortunately we’re not in a world where they’re going to be zero.”
In the quarter, the primary care provider’s medical claims expense doubled year over year to almost $310 million. Oak Street’s medical loss ratio of 82.2% was lower than analysts expected, though management said they expected it to be higher in the fourth quarter.
Pykosz and Cook called out medical costs from new patients brought in during 2021 as a system-wide stressor.
Because diagnoses from 2020 claims are used to determine 2021 risk scores, fewer claims last year could mean lower risk scores and lower payments for plans this year. Oak Street’s patients, especially older adults in low-income communities, used fewer services last year during COVID-19, which resulted in lower revenues this year even as costs expanded.
Management said they expected to get back on track in 2022 as patients new to Oak Street this year will contribute to higher reimbursement next year, closing the current medical-cost gap between tenured and new patients.
“This is certainly an outlier year from every other year we’ve had results,” Pykosz said.
Oak Street, which was founded in 2012 and went public in August 2020 at a $9 billion valuation, reported a net loss of almost $110 million in the quarter, compared to a loss of $59 million at the same time last year.
Oak Street continued expanding its membership and network in the quarter, reporting 69% at-risk patient growth and opening 15 new centers in seven new markets.
But Pykosz pointed to Oak Street’s exclusive relationship with senior group AARP and its acquisition of specialty telehealth provider RubiconMD as differentiators, while noting there’s room for a number of players in the space.
“At this point we don’t feel there’s a lot of pressure or competitive dynamics pressuring our performance,” Pykosz said.
In the third quarter, Oak Street served 100,500 risk-based patients, representing 76% of its total patient base. The company expects at-risk patient volume to grow to between 111,500 and 113,500 patients this year.
Workers at Pittsburgh-based UPMC plan to strike over wages and benefits, the Post-Gazette reported Nov. 5.
Service Employees International Union Healthcare Pennsylvania, which does not represent the workers but is supporting them, told Becker’s Hospital Review the strike would involve workers at UPMC hospitals in Pittsburgh, including transporters, dietary workers, housekeepers, nurses, patient care techs, medical assistants, pharmacy techs, surgical techs, valets, therapists, health unit coordinators and administrative assistants. Workers plan to strike for one day on Nov. 18.
The workers are demanding a $20 per hour minimum wage, affordable high-quality healthcare, elimination of all medical debt and respect for union rights, according to a union news release.
Their strike notice came after UPMC announced Nov. 2 that the health system is giving 92,000 staff members a bonus of $500 to thank them for their work during the pandemic. UPMC will issue the bonuses on Nov. 26. The health system also announced improvements to employee compensation and benefit programs, including raising the entry level wage to $15.75 in January, according to the Post-Gazette.
“There was no ‘thank you pay’ until we started organizing to strike,” Juilia Centofanti, pharmacy tech at UPMC Children’s Hospital of Pittsburgh, said in a news release.
Ms. Centofanti added that employees are “owed this [$20 per hour wage] and so much more,” and said she “will continue organizing with my co-workers for the pay, safer staffing and union rights we deserve.”
In announcing the bonuses, Leslie Davis, president and CEO of UPMC, told workers, “Over the past 20 months, you have risen in truly exceptional ways to meet challenges we could have never anticipated. With your critical support, UPMC continues to care for so many.”
A UPMC spokesperson declined to comment to Becker’s on Nov. 5.
UPMC is a $23 billion healthcare provider and insurer. SEIU Healthcare Pennsylvania has been trying to organize about 3,500 hourly workers at UPMC Presbyterian and Shadyside hospitals for nearly a decade, but has not yet held a unionization vote, according to the Post-Gazette.