A jury found former Vanderbilt Health nurse RaDonda Vaught guilty of negligent homicide and gross neglect of an impaired adult after she committed a fatal drug error in 2017. Vaught, who gave a patient a lethal dose of the paralytic agent vecuronium rather than the sedative Versed, overlooking several warning alerts, now faces up to six years in prison.
The Gist: Criminal charges for unintentional medical errors like this one are very unusual; discipline is normally the purview of licensing boards and civil courts. While Vaught certainly made an egregious mistake that directly led to a patient’s death, there’s a delicate line between holding caregivers accountable and making them criminally liable for unintentional errors.
The American Nurses Association warns this verdict could set a dangerous precedent, and have a chilling effect on providers’ reporting errors. Health systems have worked diligently over decades to promote a culture of quality improvement and transparency—central to that is an environment that encourages providers to report all medical errors in order to improve patient safety. Many providers are now concerned that this conviction could reverse that progress.
As the workforce shortages worsened and the pandemic caused widespread burnout, many hospitals and health systems saw their labor expenses significantly rise as they were forced to pay more to attract and retain workers.
Hospitals and health systems ramped up wages, provided hiring bonuses and offered new benefits to ensure they could staff beds. However, it left us with one question: Are these rising labor expenses sustainable?
The answer to the question appears to be multifaceted and dependent on an organization’s vantage point. For example, unions say hospitals can afford wage increases and bonuses, while CFOs argue that there needs to be more sustainable methods.
Northwell Health CFO Michele Cusack lays it out very clearly: “Growth in wages more than revenue trends is not sustainable.”
Moving to a more sustainable method
At the start of the workforce shortage, hospitals and health systems turned to more immediate retention and recruitment efforts: bonuses and pay increases, according to Kaufman Hall’s Senior Vice President Therese Fitzpatrick, PhD, RN, and Managing Director Dawn Samaris. However, now that the staffing shortage has stabilized in some parts of the country — though not all — hospitals are turning to more strategic, long-term strategies to ease the labor shortage, they said.
“Initially, there was a scramble to find bonus structures and increase everybody’s pay,” Ms. Samaris said. “Now, folks are stepping back and saying, ‘Well, that can’t be the only tool. We’ve got to have other options available.”
New Hyde Park, N.Y.-based Northwell Health, for example, has been focused on bending this unsustainable cost curve of rising labor expenses “by focusing on culture, our mission and ensuring that the employees know and recognize their contribution to their communities and that they are special and are making a difference,” Ms. Cusack told Becker’s Hospital Review.
For Andrew Gaasch, CFO of Centennial, Colo.-based Centura Health, a health system with about 21,000 employees, recruitment and retention is about remaining competitive with the market when it comes to pay, while also keeping the sustainability of the organization in mind.
“That’s paramount for us to be able to deliver high-quality, whole-person care across all of our flourishing communities in Colorado and western Kansas,” Mr. Gaasch said. “At the same time, we have to maintain a healthy margin to be able to continue to invest in our communities, both from a human capital and physical capital perspective. It really is a tightrope between the two.”
He said his health system’s motto around this is, “Save where we can to spend where we should.”
“We need to be able to spend and should be able to spend on employees and in our communities,” Mr. Gaasch said.
Are hiring bonuses in healthcare here to stay?
In the fall, Centura Health offered a market bonus for bedside registered nurses. The $15,000 one-time payment, which was tied to a certain time commitment to the health system, helped reduce RN turnover from 41 percent last October to 28 percent currently.
“We took a moment and took a step back and said, ‘We have to do something more creative than just adding more dollars just to the average hourly rate. We need to do something different.’ So that’s why we approached the market bonus for bedside caregivers,” Mr. Gaasch said.
About 2,500 employees accepted the market bonus and of those, only 19 have left Centura Health. About 850 employees turned down the market bonus and of those, 137 have left Centura Health.
One thing that is staying at Centura Health: sign-on bonuses for hard-to-fill positions.
Mr. Gaasch said there are different tiers of eligibility around the sign-on bonuses, which are based on factors such as market conditions and vacancy rates. The range for sign-on bonuses at Centura Health is $7,500 to $20,000.
Over the last 14 months, Centura Health has invested more than $200 million in additional employee compensation and benefits. Additionally, the health system recently announced another $31 million investment in employees through market adjustments and benefits including student loan assistance and child care assistance.
“We’re really trying to listen to the needs of our incredible people because it’s not just about base wages, it’s about the total package and it’s about benefits,” Mr. Gaasch said.
Unions: Hiring bonuses are great, but more long-term change is needed
One of the health systems that has recently offered major sign-on incentives is Providence in Renton, Wash. In September, the health system announced $1,000 bonuses for all caregivers, referral bonuses of up to $7,500 and sign-on bonuses for 17,000 positions.
The Providence perks were designed “to reward, retain and recruit,” amid a lack of staff and rising numbers of COVID-19 patients. Though the perks may be successful at attracting more workers, Tyler Kissinger with the National Union of Healthcare Workers says those workers won’t stay for long unless underlying issues are addressed.
“Hospitals were chronically understaffed before the pandemic. Short-term bonus programs might help get more workers hired, but they won’t stay if the hospital is chronically understaffed and their patients aren’t getting the care they need,” Mr. Kissinger said.
Mr. Kissinger is an organizing coordinator with the NUHW in Northern California, focused on Providence hospitals located in Sonoma and Napa counties. He believes incentives like sign-on and referral bonuses only go so far, and improving the workplace itself is key to attracting and retaining employees.
“The only way to sustainably attract and retain workers is to increase staffing to sustainable levels so healthcare workers don’t burn out trying to do everything they can to care for their patients,” Mr. Kissinger said. “Healthcare workers get into this field because they want to help people get better. When they see hospitals skimp on staffing, while paying their CEOs millions of dollars, it’s disheartening, and it results in people leaving.”
The same week Providence announced their incentive programs, a Gallagher survey reported a 75 percent increase in average hourly rates for agency RNs nationwide, rising from $75 pre-pandemic to more than $130 in September 2021. Despite the major increase in pay, the national RN vacancy rate stood at 19 percent, more than double pre-pandemic levels. To find enough nurses, 75 percent of healthcare organizations are turning to agency and travel RN companies.
“We’re seeing major healthcare chains like Providence rely more heavily on travelers and hiring bonuses. That’s not a sustainable solution,” Mr. Kissinger said. “The sustainable solution for hospital chains like Providence is to change their business model to focus less on profit and more on providing care, and that starts with hiring more caregivers and making the work more manageable so more people will enter and stay in the field.”
Other healthcare unions such as the Illinois Nurses Association signaled their full support for sign-on bonuses to boost critical staffing levels, but say these types of incentives may be sustainable for health systems because they aren’t necessarily spending more to fund them.
“INA understands and supports hospitals that offer signing bonuses to attract nurses if these are used as part of a comprehensive and fair compensation strategy that treats nurses with respect and dignity,” an INA spokesperson said. “All too often, we have found that these bonuses replace compensation and benefits that could be used for senior nurses who have worked several years for institutions that have not treated them well, especially during the last two years.”
It’s a sentiment shared by Mr. Kissinger, who says nurses and physicians may be offered major sign-on bonuses, increased pay and benefits like child care subsidies, but support positions won’t be offered nearly as much, if at all.
“At Providence hospitals, we’ve secured better wages for many workers in certified and licensed positions, but Providence has so far refused our proposals to increase pay for lower-paid workers such as housekeepers, nursing assistants, transporters and kitchen staff,” Mr. Kissinger said.
Reducing or sunsetting other expenses
Dr. Fitzpatrick of Kaufman Hall said the focus is now on creating a robust pipeline of staff, whether it’s professional staff, technical staff or entry-level staff. One example of how organizations are doing this is through partnerships with higher education to train students and then move them to employment. Ms. Samaris said some places are also creating simulation labs that imitate a real hospital setting for community colleges to train their students.
Another example is through “shadow traveler” programs, or internal travel nursing, Ms. Samaris said. This gives nurses the opportunity to travel within the system for slightly higher pay, rather than forcing them to move to an external agency. Pittsburgh-based UPMC is among the organizations using this approach.
Ms. Samaris added that hospitals are enacting strategies to lower costs in other areas. This includes optimizing staffing in the areas that need it most, analyzing where there is a duplication of services and creating partnerships with other organizations to offer services, like behavioral health or home health.
At Northwell Health, Ms. Cusack said that in response to wage pressures and other COVID-19 costs, the health system has reduced discretionary spending and placed a great focus on increasing product standardization and other operating efficiencies. Northwell is also reducing costs through the remote-work shift.
“With the growth of the hybrid work environment, we can reduce our administrative real estate portfolio to further counterbalance the expense pressure from wage growth,” Ms. Cusack said.
Mr. Gaasch cited examples of where the health system is using its motto to save costs to offset this labor pressure, such as leveraging Centura Health’s size and scale where possible; automating processes where possible; considering centralization of services as appropriate; ensuring overhead functions operate as efficiently as possible; and reviewing work-from-home policies and corresponding real estate costs.
He said Centura Health is also reducing premium pay categories that the health system has been heavily reliant on through the pandemic.
“The pandemic has slowed as far as the number of COVID-19 patients we’re treating, so we’re starting to look at premium pay categories that we instituted and how can we start to ratchet those down, in a corresponding timeline with the number of COVID patients decreasing and regaining our footing on staffing,” he explained.
He said Centura Health is also considering its supply chain and is trying to standardize where possible on products and use across the health system.
Is there a hard stop for how high labor expenses can grow?
Overall, Mr. Gaasch said he doesn’t have a set ceiling on how high labor costs can grow, because paying clinicians is vital to remain competitive.
Ms. Cusack agreed that there’s not a “hard stop” on how high labor expenses rise, saying that the health system must “ensure we have the appropriate staffing levels in the various clinical functional areas in response to the volume of patients that we care for every day.”
Dr. Fitzpatrick agreed, saying: “There really is no hard stop. … This is a continually evolving situation. … I think the solutions will continue to evolve as well.”
Becker’s calculated the payer mix within the nation’s top ranked hospitals to determine the share of their patients covered under commercial plans, Medicare, Medicaid, Medicare Advantage, uninsured/bad debt and charity care.
The 2019 data released April 5 is from the coverage, cost and value team at the National Academy for State Health Policy in collaboration with Houston-based Rice University’s Baker Institute for Public Policy.
Payer mix in the nation’s top 19 hospitals:
(1) Mayo Clinic Hospital — Rochester, Minn.
Commercial: 50 percent
Medicare: 33 percent
Medicare Advantage: 9 percent
Medicaid: 7 percent
Charity care: 1 percent
Uninsured / Bad debt: 0 percent
(2) Cleveland Clinic Hospital
Commercial: 45 percent
Medicare: 24 percent
Medicare Advantage: 17 percent
Medicaid: 12 percent
Charity care: 1 percent
Uninsured / Bad debt: 1 percent
(3) Ronald Reagan UC Los Angeles Medical Center
Commercial: 45 percent
Medicare: 27 percent
Medicaid: 18 percent
Medicare Advantage: 8 percent
Charity care: 0 percent
Uninsured / Bad debt: 0 percent
(4) Johns Hopkins Hospital — Baltimore
Commercial: 46 percent
Medicare: 28 percent
Medicaid: 22
Medicare Advantage: 2 percent
Uninsured / Bad debt: 2 percent
Charity Care: 1 percent
(5) Massachusetts General Hospital — Boston
Commercial: 48 percent
Medicare: 32 percent
Medicaid: 11 percent
Medicare Advantage: 7 percent
Charity care: 1 percent
Uninsured / Bad debt: 1 percent
(6) Cedars-Sinai Medical Center — Los Angeles
Commercial: 42 percent
Medicare: 41 percent
Medicaid: 10 percent
Medicare Advantage: 6 percent
Charity care: 1 percent
Uninsured / Bad debt: 0 percent
(7) NewYork-Presbyterian Hospital — New York City
Commercial: 34 percent
Medicaid: 25 percent
Medicare: 22 percent
Medicare Advantage: 17 percent
Charity Care: 1 percent
Uninsured / Bad debt: 1 percent
(8) NYU Langone Hospital — New York City
Commercial: 42 percent
Medicare: 25 percent
Medicaid: 19 percent
Medicare Advantage: 6 percent
Charity care: 1 percent
Uninsured / Bad debt: 0 percent
(9) UC San Francisco Medical Center
Commercial: 42 percent
Medicaid: 25 percent
Medicare: 25 percent
Medicare Advantage: 5 percent
Charity Care: 1 percent
Uninsured / Bad debt: 0 percent
(10) Northwestern Memorial Hospital — Chicago
Commercial: 52 percent
Medicare: 27 percent
Medicaid: 11 percent
Medicare Advantage: 7 percent
Charity care: 2 percent
Uninsured / Bad debt: 1 percent
(11) Michigan Medicine — Ann Arbor
Commercial: 53 percent
Medicare: 20 percent
Medicaid: 14 percent
Medicare Advantage: 11 percent
Charity care: 1 percent
Uninsured / Bad debt: 1 percent
(12) Stanford Hospital — Palo Alto, Calif.
Commercial: 46 percent
Medicare: 34 percent
Medicaid: 13 percent
Medicare Advantage: 7 percent
Charity care: 0
Uninsured / Bad debt: 0
(13) Penn Presbyterian Medical Center — Philadelphia
Commercial: 46 percent
Medicare: 29 percent
Medicaid: 13 percent
Medicare Advantage: 12 percent
Uninsured / Bad debt: 1 percent
Charity Care: 0
(14) Brigham and Women’s Hospital — Boston
Commercial: 53 percent
Medicare: 30 percent
Medicaid: 10 percent
Medicare Advantage: 6 percent
Charity Care: 1 percent
Uninsured / Bad debt: 1 percent
(15) Mayo Clinic Hospital — Phoenix
Commercial: 51 percent
Medicare: 42 percent
Medicare Advantage: 4 percent
Medicaid: 3 percent
Charity Care: 1 percent
Uninsured / Bad debt: 0 percent
(16) Houston Methodist Hospital
Commercial: 43 percent
Medicare: 33 percent
Medicare Advantage: 18 percent
Charity care:3 percent
Medicaid: 2 percent
Uninsured / Bad debt: 1 percent
(17 — tie) Barnes-Jewish Hospital — St. Louis
Commercial: 43 percent
Medicare: 29 percent
Medicare Advantage: 13 percent
Medicaid: 10 percent
Charity care: 4 percent
Uninsured / Bad debt: 1 percent
(17 — tie) Mount Sinai Hospital — New York City
Commercial: 33 percent
Medicaid: 28 percent
Medicare: 22 percent
Medicare Advantage: 15 percent
Charity care: 1 percent
Uninsured / Bad debt: 0 percent
(18) Rush University Medical Center — Chicago
Commercial: 41 percent
Medicare: 31 percent
Medicaid: 20 percent
Medicare Advantage: 6 percent
Charity care: 2 percent
Uninsured / Bad debt: 1 percent
(19) Vanderbilt University Medical Center — Nashville, Tenn.
Several hospitals are trimming their workforces due to financial and operational challenges, and some are offering affected workers new positions.
1. Watsonville (Calif.) Community Hospital is preparing to lay off 658 workers, according to a notice filed with the state and shared with Becker’s Hospital Review. The hospital, which filed for Chapter 11 bankruptcy in December, expects the layoffs to occur between May 16 and May 23.
2. Toledo, Ohio-based ProMedica’s health plan, Paramount, is laying off about 200 employees in July after losing a Medicaid contract. Anthem acquired Paramount’s Medicaid contract, and ProMedica and Anthem have been working to identify open roles for employees affected by the layoffs.
3. NYC Test & Trace Corps, the city’s initiative for COVID-19 testing and contact tracing, is ending universal contact tracing by the end of April. NYC Health + Hospitals, which leads the program in collaboration with the city’s department of health and other agencies, is planning to lay off 874 workers when the program scales back, according to a notice filed with state regulators March 4. The health system said affected temporary employees will be laid off at the end of April. Managerial employees affected by the layoffs will have their employment terminated between May 13 and May 27, according to the notice.
4. MarinHealth Medical Center is laying off 104 revenue cycle and supply chain employees in April after entering into a contract with Optum to provide those services, according to a notice filed with state regulators in February. Greenbrae, Calif.-based MarinHealth said that as a result of the contract with Optum, all non-contractual revenue cycle and supply chain employees will be terminated from employment with the hospital on April 9. Optum is offering jobs to most workers affected by the layoffs. Employees who accept an offer will begin employment with Optum on the first work day following separation from MarinHealth, a spokesperson for the hospital told Becker’s Hospital Review.
5. St. Mary’s Medical Center in West Palm Beach, Fla., is laying off 49 employees, including 21 registered nurses, when it stops providing mental health services in April, according to a notice filed with state regulators.
6. West Reading, Pa.-based Tower Health closed Brandywine Hospital in Coatesville, Pa., on Jan. 31. As a result of the closure, 534 employees were laid off Feb. 7, according to a notice filed with state regulators.
7. Community Hospital Long Beach (Calif.) shut down and surrendered its acute care license to the state in December, according to the Long Beach Post. The hospital laid off 328 employees early this year, according to a notice filed with state regulators. The hospital said the layoffs would begin Feb. 1 and may come in stages. The hospital’s owner is planning to transition the facility into a behavioral health and wellness campus.
Due to financial struggles, West Reading, Pa.-based Tower Health is looking for other health systems to take over St. Christopher’s Hospital for Children, which it co-owns with Drexel University, rather than renew its $85 million line of credit to the hospital, The Philadelphia Inquirer reported April 8.
Tower Health’s credit line was set to expire March 31, but Drexel University renewed its line of credit to the Philadelphia hospital for the next four years.
Philadelphia-based St. Chris has been struggling financially, but has recently improved. Its projected loss was $23.6 million for the year ended June 30, compared to $97.6 million in fiscal year 2021, Drexel University President John Fry told the Inquirer.
“We will stand behind this hospital and we will find a solution. We just need more help than the help that Drexel and Tower can provide,” Mr. Fry told the paper.
The hospital was part of the American Academic Health System bankruptcy in 2019. It was previously owned by Dallas-based Tenet Healthcare.
Tower Health has also been dealing with financial problems, with operating losses of more than $900 million in the last four and a half fiscal years, according to the paper.
Temple University Health System confirmed to the Inquirer that it is in discussions to help support the hospital.
Insurers and health systems across the U.S. have been at odds during the most recent cycle of contract negotiations, and terminated contracts are affecting thousands of patients.
As hospitals continue to recover financially from the COVID-19 pandemic and deal with higher supply costs and employee wages, many organizations have tightening margins and hope to negotiate higher rates with insurers as a result. Hospitals are also pointing to rising inflation as a reason for needing higher rates.
One recent example is Fort Lauderdale, Fla.-based Broward Health’s public breakup with UnitedHealthcare. Thousands of the insurer’s beneficiaries went out of network with Broward April 1 after the two sides failed to agree on a new contract. Broward reportedly asked UnitedHealthcare for a pay increase to the same level UnitedHealthcare pays other South Florida health systems.
UnitedHealthcare said Broward’s rate increase request would amount to 88 percent higher reimbursement for its providers in the next four years, which the insurer said was “unreasonable.” Negotiations continue, but patients are out of network in the meantime.
Blue Cross & Blue Shield of Mississippi and the University of Mississippi Medical Center let their contract expire April 1 after they failed to agree on pay rate increases, according to the Clarion Ledger. The medical center treated more than 50,000 patients in the 18 months before the contract expiration.
LouAnn Woodward, MD, vice chancellor for health affairs and dean of the medical center’s school of medicine, said the health system wants “fair reimbursement” from Blue Cross & Blue Shield to reinvest in its facilities and programs. The insurer said the medical center wanted a 30 percent overall rate increase, including a 50 percent increase for some services, according to the newspaper report.
Physician groups and surgery centers aren’t immune from insurer conflicts. Blue Cross Blue Shield of Illinois terminated its contract with Springfield (Ill.) Clinic late last year, knocking 100,000 beneficiaries out of network.
Moody’s Investors Service has downgraded the ratings on Providence’s revenue bond debt to “A1” from “Aa3.”
“The downgrade to ‘A1’ is driven by the disaffiliation with Hoag Hospital, and the expectation that weaker operating, balance sheet, and debt measures will continue for the time being,” Moody’s said in an April 5 release.
Renton, Wash.-based Providence and Newport Beach, Calif.-based Hoag ended their affiliation Jan. 31. The two organizations cut ties at a time when Providence is facing several challenges, including operating pressures, variable utilization and reliance on temporary labor, Moody’s said.
The “A1” rating and stable outlook also reflect Providence’s strengths, including a large service area, a large revenue base of more than $25 billion and a leading market share in all of its markets.
Moody’s said it expects Providence to continue to grow its operating platform and generate additional revenue growth.
Thousands of nurses at Stanford and Lucile Packard Children’s hospitals in Palo Alto, Calif., have authorized the union representing them to call a strike.
In an April 8 news release, the Committee for Recognition of Nursing Achievement said more than 4,500 nurses at Stanford and Packard, or 93 percent of all nurses eligible, voted in favor of strike authorization. They are calling on hospital management to adequately address staffing, citing consistent overtime and nurses’ complaints of inadequate resources, training or staff. They also seek improved access to mental health counseling, as well as competitive wages and benefits.
“The decision by members to overwhelmingly authorize a strike shows that we are fed up with the status quo of working conditions at the hospitals,” Colleen Borges, union president and a nurse in the pediatric oncology department, said in the release. “We need contracts that allow us to care for ourselves and our families so we can continue providing world-class care.”
Nurses authorized the strike after bargaining for the last 13 weeks and are working without contracts. The vote does not mean a strike will occur, but it gives the union the ability to issue an official strike notice.
In a statement shared with Becker’s, Stanford expressed its support for negotiations rather than a strike.
“We are committed, through good faith bargaining, to reach agreement on new contracts that provide nurses a highly competitive compensation package, along with proposals that further our commitment to enhancing staffing and wellness benefits for nurses,” the statement said.
The hospital also said it is taking the steps to prepare for the possibility of a strike, while hoping a strike is averted.
“Given the progress we have made by working constructively with the union, we should be able to reach agreements that will allow us to continue to attract and retain the high caliber of nurses who so meaningfully contribute to our hospitals’ reputation for excellence,” the statement read.
Hospitals across the U.S. saw their operating margins remain negative for the second consecutive month in February as they continued to feel the repercussions of the winter omicron surge, according to Kaufman Hall’s “National Hospital Flash Report: March 2022” posted March 28.
The median operating margin in February was -3.45 percent, up from -4.52 percent in January, but “still well below sustainable levels,” Kaufman Hall said.
Kaufman Hall said the improvement in hospital margin was driven by disproportionate increases among several hospitals that saw margin gains, but most hospitals reported margin declines in February. Specifically, the median operating margin was down 11.8 percent month over month.
“The second month of 2022 brought further challenges for the nation’s hospitals and health systems,” Kaufman Hall said. “Overall, the year is off to a difficult start.”
Kaufman Hall noted that patient days were down 13.3 percent month over month, and fewer severely ill COVID-19 patients also contributed to shorter hospital stays as the average length of stay dropped 5.3 percent month over month.
Hospitals’ gross operating revenue also decreased 7.4 percent compared to January 2022, with outpatient revenue falling 5 percent and inpatient revenue declining 19.3 percent.
Kaufman Hall noted that hospitals saw some improvement month over month in terms of expenses. Total expenses per adjusted discharge fell 4.5 percent compared to January, labor expense per adjusted discharge fell 6.1 percent and non-labor expenses per adjusted discharge was down 3.6 percent. However, Kaufman Hall noted that year over year, expenses are still up significantly, with total adjusted expense per adjusted discharge rising 10.4 percent compared to February 2021.
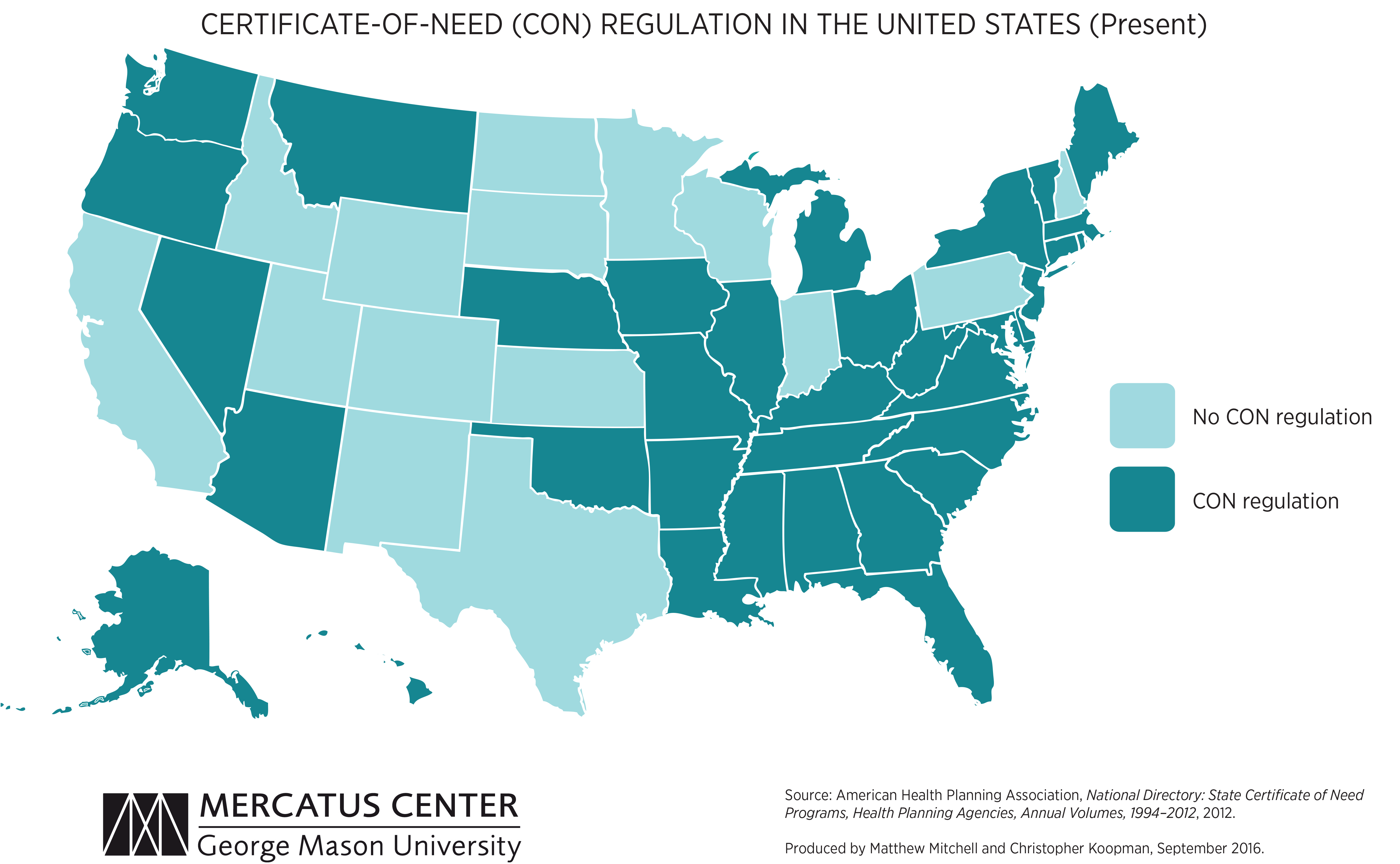
We’re picking up on a growing concern among health system leaders that many states with “certificate of need” (CON) laws in effect are on the cusp of repealing them. CON laws, currently in place in 35 states and the District of Columbia, require organizations that want to construct new or expand existing healthcare facilities to demonstrate community need for the additional capacity, and to obtain approval from state regulatory agencies. While the intent of these laws is to prevent duplicative capacity, reduce unnecessary utilization, and control cost growth, critics claim that CON requirements reduce competition—and free market-minded state legislators, particularly in the South and Midwest, have made them a target.
One of our member systems located in a state where repeal is being debated asked us to facilitate a scenario planning session around CON repeal with system and physician leaders. Executives predicted that key specialty physician groups would quickly move to build their own ambulatory surgery centers, accelerating shift of surgical volume away from the hospital.
The opportunity to expand outpatient procedure and long-term care capacity would also fuel investment from private equity, which have already been picking up in the market. An out-of-market health system might look to build microhospitals, or even a full-service inpatient facility, which would be even more disruptive.
CON repeal wasn’t all downside, however; the team identified adjacent markets they would look to enter as well. The takeaway from our exercise: in addition to the traditional response of flexing lobbying influence to shape legislative change, the system must begin to deliver solutions to consumers that are comprehensive, convenient, and competitively priced—the kind of offerings that might flood the market if CON laws were lifted.