Last week, we examined how the fast-growing Medicare Advantage (MA) market remains heavily concentrated among a handful of large carriers. But amid this concentration, consumers have more options than ever before, both in terms of carriers and plans, as shown in the graphic below.
The average MA enrollee can now choose from among 39 health plans offered by nine different payers, the majority of which feature $0 insurance premiums. An increasing number of plans also now offer a variety of non-medical benefits.
Landing an MA consumer soon after they become eligible is critical for carriers, as more than seven in 10 Medicare beneficiaries stick with the plan they have year after year. While this “stickiness” may suggest enrollees are satisfied with their current coverage, it also calls into question whether the MA marketplace is actually working as intended.
With another revenue boost to MA plans proposed for 2023, competition between plans—as well as consolidation among carriers—will continue to heat up, especially as the number of Medicare-eligible Americans will increase by nearly 50 percent over the next three decades.
A commentary piece in Health Affairs argues that CMS’s value-based payment (VBP) initiatives have not reached their full potential because they fail to take into account conflicting market dynamics.
The authors argue that VBP models won’t take hold unless CMS both increases the “carrots”, or positive incentives, that market dominant providers receive to support true care transformation, and sharpens the “sticks” by requiring participation in accountable care organization (ACO) models, decreasing the attractiveness of fee-for-service (FFS) payments, and banning anti-competitive commercial deals that discourage steering referrals toward lower-cost providers.
The Gist: To date, CMS’s VBP efforts have largely fallen short of their two primary objectives: transforming care at scale across the country, and generating meaningful savings for the federal government.
With more and more seniors choosing Medicare Advantage (MA) each year, the federal government clearly views MA as the primary vehicle to control Medicare cost growth in the future—although savings will ultimately hinge on CMS cutting payments to insurers in the future.
Over time, continuing to foster the growth of MA may prove more successful than overcoming the myriad complications of FFS-based VBP programs.
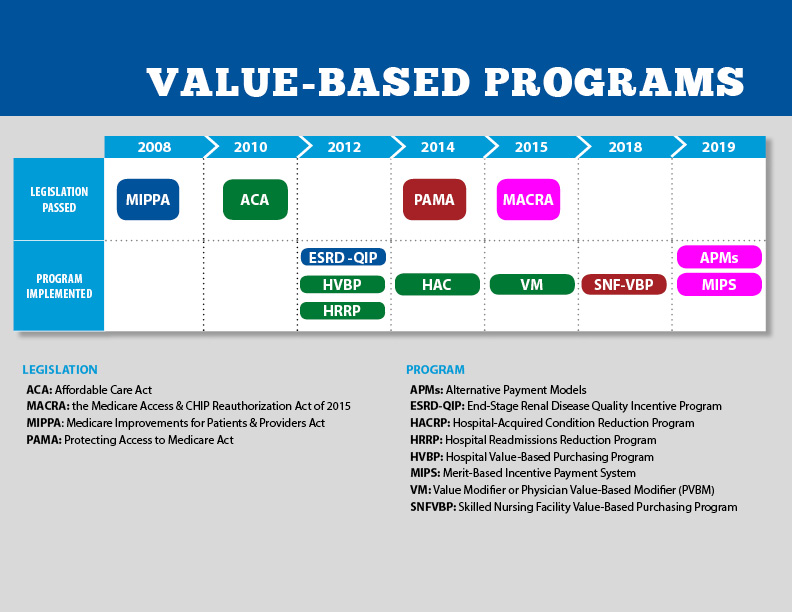
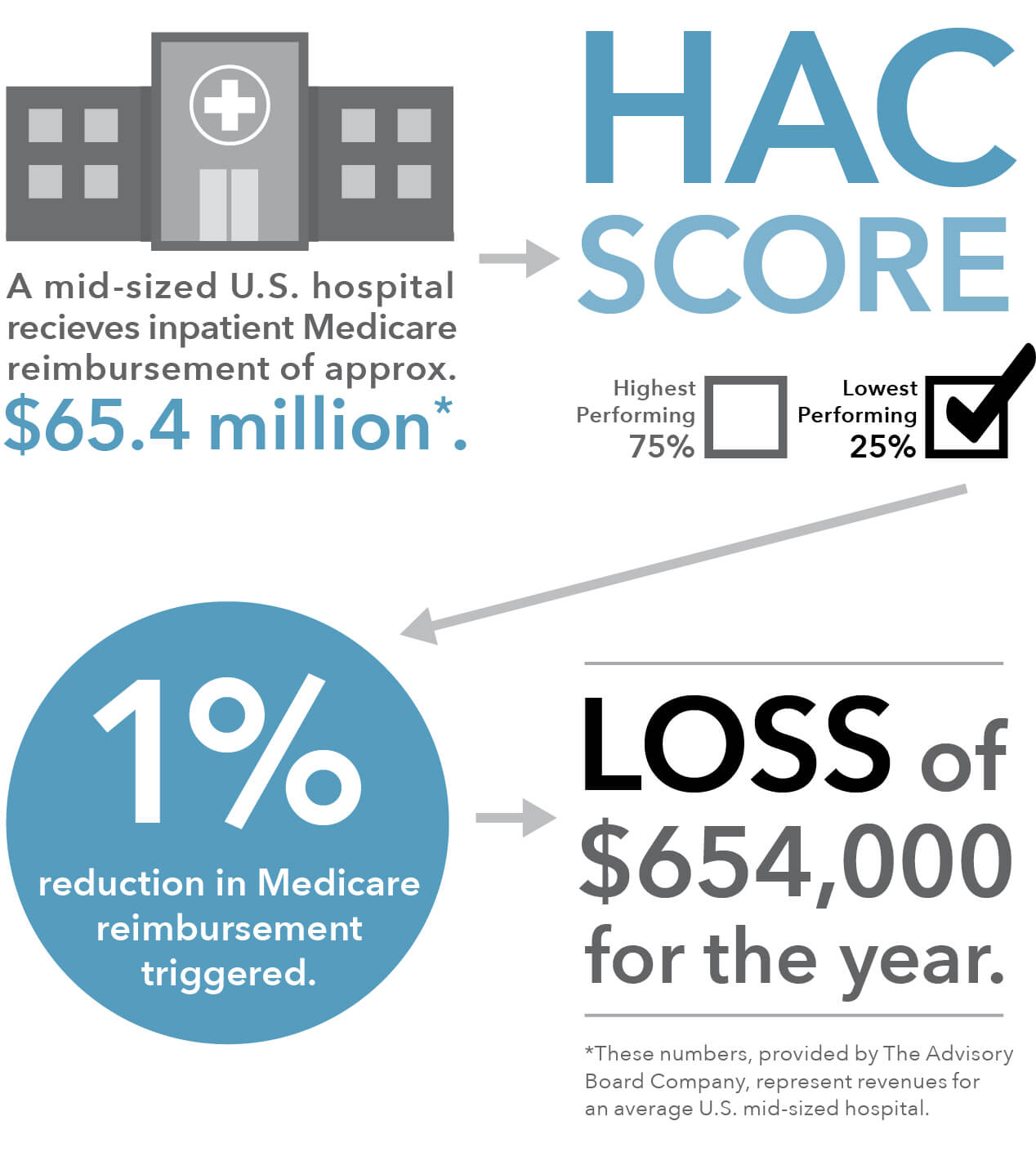
Of the 764 hospitals the Centers for Medicare and Medicaid Services (CMS) is penalizing this year with a one percent reduction in Medicare payments for scoring in the bottom quartile in the Hospital-Acquired Condition Reduction (HAC) Program, 38 also earned a five-star rating from CMS for overall quality of care.
This paradox is in part because Medicare’s star ratings compare a hospital’s safety and quality to a calculated average, whereas the HAC program requires Medicare to penalize the lowest-performing quartile of hospitals each year, even if they are showing improvement, or if the difference between low- and high-performing hospitals is miniscule.
The Gist: The promise of Medicare’s pay-for-performance incentive programs has not materialized, and is unlikely to be driving true clinical improvement. In addition to being confusing and tedious to comply with, the programs lack impact because penalties and rewards are too small to impact a hospital’s bottom line—the benefits don’t justify the costs of redesigning care processes or changing behavior. With years of evidence that many of these ACA-era quality programs aren’t producing the desired results, it’s time to find more effective ways of improving patient outcomes.
The American Hospital Association (AHA) is asking Congress for an additional $25B to help hospitals offset high labor costs, largely incurred by the need to rely on travel nurse staffing firms that charge two to three times pre-pandemic rates. The AHA, along with 200 members of Congress, is urging the Federal Trade Commission to investigate the staffing agencies for anti-competitive activity, although the agency has previously declined to do so.
The Gist: The Department of Health and Human Services (HHS) is now releasing$2B in of provider relief dollars from the CARES Act. Beyond that, after nearly two years and $178B of federal support, hospitals shouldn’t count on additional funds from the government, even as costs of labor and supplies continue to rise.
Instead, we’d expect more scrutinyover how the remaining relief dollars are spent. Federal support during the pandemic has masked structural economic flaws in provider economics, and we expect 2022 will be a year of financial reckoning for many hospitals and health systems.
Net prices of brand-name drugs have increased significantly over the last decade. But savings from generics have driven average prescription prices down in Medicare and Medicaid, Axios’ Caitlin Owens writes about a new analysis by the Congressional Budget Office.
Why it matters: The analysis reiterates that the generic market is largely working as it’s intended to.
By the numbers: The average net price of a prescription fell from $57 in 2009 to $50 in 2018 in Medicare Part D, and from $63 to $48 in Medicaid.
The drop is largely attributable to the growing use of generics, which jumped from 75% to 90% of all prescriptions nationally during that time frame. The average price for a generic prescription also fell in both programs.
But the average net brand-name prescription price more than doubled in Part D and increased by 50% in Medicaid, per the analysis. These increases were driven by higher launch prices for new drugs and price increases for drugs already on the market.
Large insurers Humana and Cigna, along with “insurtech” startups Bright Health and Alignment Healthcare, all lowered expectations for their MA membership growth after missing 2022 enrollment targets. The companies blamed fierce competition for the nation’s estimated 29.5M MA lives, and highlighted a focus on diversifying revenue through other business arms like healthcare delivery and service sales.
The Gist: Insurers’ missed expectations are leading some to question whether the MA market is beginning to weaken, but these concerns are overblown, with last fall’s enrollment affected by the pandemic, which hindered brokers’ ability to reach seniors.
Some MA-focused startups are finding challenges in their attempts to scale, and their stock prices will continue to retreat from the lofty valuations that drove their public offerings.
Insurers still have plenty of running room to grow their MA books of business, but will face increasing scrutiny of their ability to manage patients and control costs for the aging population.
Monthly premiums that cover physician and outpatient care for Medicare patients will increase by 15% next year, the Biden administration said in a notice Friday evening.
Why it matters: People on Medicare are getting slammed with a big hike during an election year, due largely to the big price tag from the questionable Alzheimer’s treatment, Aduhelm, and uncertainty stemming from the coronavirus.
By the numbers: Standard Medicare Part B premiums will be $170.10 per month next year, up from $148.50 per month this year.
That equals an extra $259.20 in extra costs over the course of the year, just in premiums.
The Part B deductible also is increasing 15%, from $203 to $233.
Between the lines: Medicare is still determining whether it will pay for Aduhelm yet, but federal actuaries have to plan for a “high-cost scenario of Aduhelm coverage,” regulators said.
The FDA approved Aduhelm in June, and Biogen priced Aduhelm at $56,000 per year on average.
That price tag, along with all of the hospital and doctor costs associated with administering the drug and ancillary tests, could lead to “very significant” costs for the taxpayer-funded program, according to the notice.
The bottom line: The pandemic has made it difficult to predict future Medicare spending, such as trying to determine whether patients will get more non-COVID care that had been put off.
But Aduhelm — a treatment that has not conclusively proved that it improves brain function of Alzheimer’s patients — is now a high-profile example of pharma pricing power affecting Medicare patients’ pocketbooks and represents a redistribution of taxpayer money into Biogen’s coffers.
Health economists study the economic determinants of health. They also analyze how health care resources are utilized and allocated, and how health care policies and quality of care can be improved. In this episode, we discuss what exactly a healthcare system would look like if these professionals were calling all the shots.
Medicare for All, which would extend health coverage to all Americans, has been a hot topic of debate in recent years. Researchers have looked into the many ways that a switch to Medicare for All might change our lives, and one of those areas of change might be wages. Employer provided healthcare is baked into our current system of healthcare, and there are a lot of studies that look at how employer paid premiums can depress wages, and how our paychecks might shift in a M4A-type situation.
The FDA could greenlight a vaccine for kids as soon as Friday and more workers now have vaccine mandates. But first:
Democrats are ditching progressives’ health priorities in their economic bill
The White House says Democrats have clinched a deal.
The $1.75 trillion framework for Biden’s massive social spending bill temporarily funds several of the party’s health care ambitions. But it includes big misses on health care, such as significantly paring back progressives’ goal of adding new benefits to Medicare — instead including only coverage for hearing services — and excluding Democrats’ plan aimed at lowering the sky-high prices of prescription drugs.
Will all Democrats get on board? Senior administration officials projected confidence that they would, and characterized the framework as the biggest expansion of health care in a decade. Yet, it includes major defeats for the party’s more liberal members, who have been reticent to draw red lines on what they would or wouldn’t support.
It’s a critical day. President Biden is heading to huddle privately with House Democrats this morning.House Speaker Nancy Pelosi announced plans for the chamber’s Rules Committee to hold a hearing, although legislative text hasn’t yet been released. And before leaving for his trip overseas, Biden will speak publicly about the path forward for his legislative agenda, per a White House official.
Early this morning, senior administration officials spoke to reporters on the condition of anonymity to detail the framework.
What’s in and what’s out
Prescription drug negotiation: OUT
Democrats campaigned on reducing prices of prescription drugs — and letting Medicare directly force lower prices is a key plank of that effort. But the party couldn’t overcome fierce divisions amid a lobbying storm.
“At the end of the day, there are not yet enough votes to get something across the line to deliver what the American people need and expect on prescription drugs,” a senior administration official said. “We’re going to keep fighting to get this done and deliver lower drug prices.”
The House’s signature drug proposal faced resistance from a trio of House moderates who instead backed more limited drug negotiation. On the other side of the Capitol, Sen. Kyrsten Sinema had raised objections and other senators had concerns with a bill as sweeping as the one the House passed in 2019. The industry’s main trade group has been working furiously to keep the proposal out of Democrats’ economic package.
Of note: The framework includes fully repealing a Trump-era ban on prescription drug rebates as a way to offset the cost of the package. The administration anticipates that would save $145 billion.
Medicare expansion: mostly OUT
Sen. Bernie Sanders (I-Vt.) and the House Congressional Progressive Caucus have been bullish on two main health policies: allowing the federal government to negotiate drug prices, and using those savings to expand Medicare to cover dental, vision and hearing.
The framework only creates a new Medicare benefit for hearing.
Rep. Pramila Jayapal (D-Wash.), the chair of the CPC, has repeatedly said her 96 members aren’t drawing red lines. But here’s how she characterized the CPC’s thoughts yesterday: “For a lot of members, it’s like what are we doing for seniors? How do we make sure we get some benefits for seniors in here?”
Sanders is the person to watch here. He’s long championed expanding Medicare, and has already come down on his ambitions for a wide-ranging $6 trillion bill.
Closing the Medicaid coverage gap: IN
The framework extends coverage for 2.2 million adults in the dozen, mostly GOP-led states that have refused Obamacare’s Medicaid expansion. They’ll get tax credits to receive premium-free health coverage on the Obamacare health exchanges through 2025.
Earlier this week, Manchin raised concerns with allowing the federal government to pay for health coverage for 2.2 million adults in the dozen, mostly GOP-led states refusing Obamacare’s Medicaid expansion. His own colleagues — such as Georgia Sens. Raphael Warnock and Jon Ossoff — lobbied heavily to change his mind.
Obamacare subsidies: IN
The framework would extend more generous financial help to Obamacare consumers through 2025, building on an effort that began in Biden’s coronavirus relief bill passed this spring.
In-home care: IN
Biden has pushed for a $400 billion investment in home care for seniors and the disabled. It’s been clear for weeks that his ask will be significantly pared back. Administration officials said funding for home and community-based services is included in the framework, but didn’t detail how much money would go toward the program helping keep seniors and those with disabilities out of institutional settings.