

Cartoon – Please Give

| Three million shots a day |
| The Biden administration has been quite cautious in setting its public vaccination goals. |
| During the transition, officials said they hoped to give shots to one million Americans per day — a level the Trump administration nearly reached in its final days, despite being badly behind its own goals. In President Biden’s first week in office, he raised the target to 1.5 million, although his aides quickly added that it was more of a “hope” than a “goal.” Either way, the country is now giving about 1.7 million shots per day. |
| I have spent some time recently interviewing public-health experts about what the real goal should be, and I came away with a clear message: The Biden administration is not being ambitious enough about vaccinations, at least not in its public statements. |
| An appropriate goal, experts say, is three million shots per day — probably by April. At that pace, half of adults would receive their first shot by April and all adults who wanted a shot could receive one by June, saving thousands of lives and allowing normal life to return by midsummer. |
| Biden struck a somewhat more ambitious tone yesterday, telling CNN that anybody who wanted a vaccine would be able to get one “by the end of July.” But Dr. Anthony Fauci also said that the timeline for when the general population could receive shots was slipping from April to May or June. |
| The shots are on their way |
| The key fact is that the delivery of vaccine doses is on the verge of accelerating rapidly. Since December, Moderna and Pfizer have delivered fewer than one million shots per day to the government. |
| But over the next month and a half, the two companies have promised to deliver at least three million shots per day — and to accelerate the pace to about 3.3 million per day starting in April. Johnson & Johnson is likely to add to that total if, as expected, it receives the go-ahead to start distributing shots in coming weeks. |
| Very soon, the major issue won’t be supply. It will be logistics: Can the Biden administration and state and local governments administer the shots at close to the same rate that they receive them? |
| “I’m not hearing a plan,” Dr. Peter Hotez, a vaccine expert at Baylor College of Medicine, told me. “In the public statements, I don’t hear that sense of urgency.” |
| Bankers’ hours for vaccine clinics |
| The experts I interviewed said they understood why Biden had set only modest public goals so far. Manufacturing vaccines is complex, and falling short of a high-profile goal would sew doubt during a public-health emergency, as Barry Bloom, a Harvard immunologist, told me. If he were president, Bloom added, he would also want to exceed whatever goal was appearing in the media. |
| But setting aside public relations, experts say that the appropriate goal is to administer vaccine shots at roughly the same rate that drug makers deliver them — with a short delay, of a week or two, for logistics. Otherwise, millions of doses will languish in storage while Americans are dying and the country remains partially shut down. |
| “We should be doing more,” Jennifer Nuzzo, an epidemiologist at Johns Hopkins, said. “I am kind of surprised by how constrained we’ve been.” Many vaccine clinics operate only during business hours, she noted. And the government has not done much to expand the pool of vaccine workers — say, by training E.M.T. workers. |
| The newly contagious variants of the virus add another reason for urgency. They could cause an explosion of cases in the spring, Hotez said, and lead to mutations that are resistant to the current vaccines. But if the vaccines can crush the spread before then, the mutations may not take hold. |
| “We need to be laser focused on getting as many people vaccinated now as possible,” Dr. Paul Sax, a top infectious-disease official at Brigham and Women’s Hospital in Boston, told me. |
| As my colleague Katie Thomas, who covers the vaccines, said: “The future looks bright — if we can do vaccination quickly enough, if people actually want the vaccines and if the variants don’t mess with the plan.” |
| ‘Our historic moment of crisis’ |
| Nobody doubts that vaccinating three million Americans every day for months on end would be a herculean task. |
| When I asked Biden about his virus plan during a December phone call, he used the term “logistical nightmare” to describe a rapid national vaccination program. “This is going to be one of the hardest and most costly challenges in American history,” he said. |
| Since then, his aides have emphasized the challenges — the possibility of manufacturing problems, the difficulty of working with hundreds of local agencies, the need to distribute vaccines equitably. They also point out that they have nearly doubled the pace of vaccination in their first month in office, accelerated the pace of delivery from drugmakers and have plans to do more, like open mass-vaccination clinics and expand the pool of vaccine workers. |
| Part of me wonders whether the White House knows that three million shots per day is the right goal and simply doesn’t want to say so. |
| When Biden and his advisers talk about the fight against Covid-19, they sometimes compare it to wartime mobilization. And the U.S. has accomplished amazing logistical feats during wartime. A single Michigan auto plant figured out how to manufacture a new B-24 bomber plane every hour during World War II, and a network of West Coast factories built one warship per day — for four years. |
| “This is our historic moment of crisis and challenge,” Biden said during his inaugural address. “We have never, ever, ever failed in America when we have acted together.” |
| Near the end of the speech, he added a question: “Will we rise to the occasion?” |
The CDC selected Walmart and Sam’s Club to help administer COVID-19 vaccines in communities across the United States.
Why it’s important: With 5,000+ pharmacy locations, the company can administer the vaccine in hard-to-reach parts of the country.


Nearly 4 million Americans have been unemployed for 27 weeks or longer — trapped in a vicious cycle that makes it harder to get back to work.
The big picture: Long-term unemployment during a pandemic is a double whammy. Millions are experiencing food and housing insecurity and lack health care when they need it most.
What’s happening: “The troubling amount of long-term unemployment and its continuing rise is dangerous for the U.S. labor market,” says Nick Bunker, an economist at the jobs site Indeed. “A fast labor market recovery will help alleviate these concerns, but that bounce back is still a ways away and dependent on controlling the coronavirus.”
Why it matters: Studies have shown that long-term unemployment hurts workers’ physical and mental health, reports Bloomberg. And the longer someone is unemployed, the harder it is for that person to get another job — let alone another job at the same pay level.
Job-seeking is even more exhausting during a pandemic, says Tim Classen, an economist at the Quinlan School of Business at Loyola University in Chicago.
“The fluctuations in uncertainty play into this, too,” Classen says. Millions of restaurant workers, flight attendants, retail workers and more aren’t sure when the pandemic will end — or if their employers will even survive it.
There’s a bit of a silver lining, though.
In recent weeks, U.S. coronavirus case data — long a closely-watched barometer of the pandemic’s severity — has sent some encouraging signals: The rate of newly recorded infections is plummeting from coast to coast and the worst surge yet is finally relenting. But scientists are split on why, exactly, it is happening.
Some point to the quickening pace of coronavirus vaccine administration, some say it’s because of the natural seasonal ebb of respiratory viruses and others chalk it up to social distancing measures.
And every explanation is appended with two significant caveats: The country is still in a bad place, continuing to notch more than 90,000 new cases every day, and recent progress could still be imperiled, either by new fast-spreading virus variants or by relaxed social distancing measures.
The rolling daily average of new infections in the United States hit its all-time high of 248,200 on Jan. 12, according to data gathered and analyzed by The Washington Post. Since then, the number has dropped every day, hitting 91,000 on Sunday, its lowest level since November.
A former director of the Centers for Disease Control and Prevention endorsed the idea that Americans are now seeing the effect of their good behavior — not of increased vaccinations.
“I don’t think the vaccine is having much of an impact at all on case rates,” Tom Frieden said in an interview Sunday on CNN’s “Fareed Zakaria GPS.” “It’s what we’re doing right: staying apart, wearing masks, not traveling, not mixing with others indoors.”
However, Frieden noted, the country’s numbers are still higher than they were during the spring and summer virus waves and “we’re nowhere near out of the woods.”
“We’ve had three surges,” Frieden said. “Whether or not we have a fourth surge is up to us, and the stakes couldn’t be higher.”
The current CDC director, Rochelle Walensky, said in a round of TV interviews Sunday morning that behavior will be crucial to averting yet another spike in infections and that it is far too soon for states to be rescinding mask mandates. Walensky also noted the declining numbers but said cases are still “more than two-and-a-half-fold times what we saw over the summer.”
“It’s encouraging to see these trends coming down, but they’re coming down from an extraordinarily high place,” she said on NBC’s “Meet the Press.”
Researchers at the University of Washington’s Institute for Health Metrics and Evaluation, publisher of a popular coronavirus model, are among those who attribute declining cases to vaccines and the virus’s seasonality, which scientists have said may allow it to spread faster in colder weather.
In the IHME’s most recent briefing, published Friday, the authors write that cases have “declined sharply,” dropping nearly 50 percent since early January.
“Two [factors] are driving down transmission,” the briefing says. “1) the continued scale-up of vaccination helped by the fraction of adults willing to accept the vaccine reaching 71 percent, and 2) declining seasonality, which will contribute to declining transmission potential from now until August.”
The model predicts 152,000 more covid-19 deaths by June 1, but projects that the vaccine rollout will save 114,000 lives.
In the past week, the country collectively administered 1.62 million vaccine doses per day, according to The Washington Post’s analysis of state and federal data. It was the best week yet for the shots, topping even President Biden’s lofty goal of 1.5 million vaccinations per day.
Nearly 40 million people have received at least their first dose of a coronavirus vaccine, about 12 percent of the U.S. population. Experts have said that 70 percent to 90 percent of people need to have immunity, either through vaccination or prior infection, to quash the pandemic. And some leading epidemiologists have agreed with Frieden, saying that not enough people are vaccinated to make such a sizable dent in the case rates.
A fourth, less optimistic explanation has also emerged: More new cases are simply going undetected. On Twitter, Eleanor Murray, a professor of epidemiology at Boston University School of Public Health, said an increased focus on vaccine distribution and administration could be making it harder to get tested.
“I worry that it’s at least partly an artifact of resources being moved from testing to vaccination,” Murray said of the declines.
The Covid Tracking Project, which compiles and publishes data on coronavirus testing, has indeed observed a steady recent decrease in tests, from more than 2 million per day in mid-January to about 1.6 million a month later. The project’s latest update blames this dip on “a combination of reduced demand as well as reduced availability or accessibility of testing.”
“Demand for testing may have dropped because fewer people are sick or have been exposed to infected individuals, but also perhaps because testing isn’t being promoted as heavily,” the authors write.
They note that a backlog of tests over the holidays probably produced an artificial spike of reported tests in early January, but that even when adjusted, it’s still “unequivocally the wrong direction for a country that needs to understand the movements of the virus during a slow vaccine rollout and the spread of multiple new variants.”
Where most experts agree: The mutated variants of the virus pose perhaps the biggest threat to the country’s recovery. One is spreading rapidly and another, known as B.1.351, contains a mutation that may help the virus partly evade natural and vaccine-induced antibodies.
Fewer than 20 cases have been reported in the United States, but a critically ill man in France underscores the variant’s potentially dangerous consequences. The 58-year-old had a mild coronavirus infection in September and the B.1.351 strain reinfected him four months later.
No matter what’s causing the current downturn in new infections, experts have urged Americans to avoid complacency.
“Masks, distancing, ventilation, avoiding gatherings, getting vaccinated when eligible. These are the tools we have to continue the long trip down the tall mountain,” Caitlin Rivers, an epidemiologist at Johns Hopkins University, said on Twitter. “The variants may throw us a curve ball, but if we keep driving down transmission we can get to a better place.”
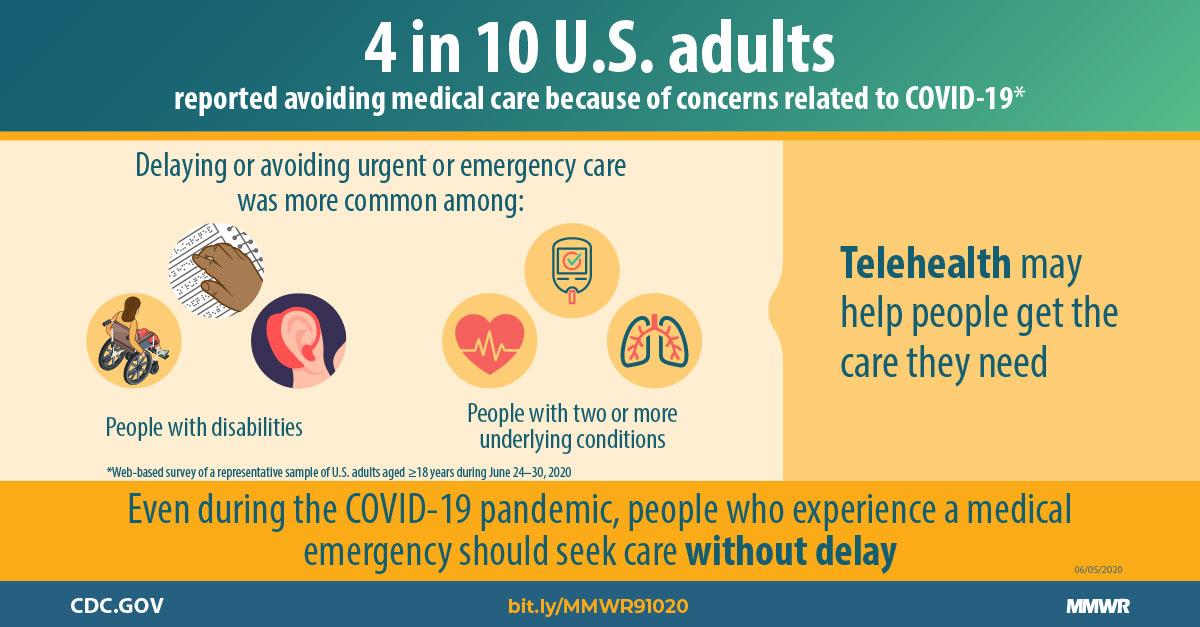
The early days of the pandemic saw widespread halts in non-emergency care, with big hits to provider finances.
In recent months, health systems have emphasized the services can be provided in hospitals and doctors offices safely as long as certain protocols are followed, and at least some research has backed them up. Groups like the American Hospital Association have launched ad campaigns urging people to return for preventive and routine care as well as emergencies.
But patients are apparently still wary, according to the findings based on surveys of about 4,000 adults conducted in September.
The research shows another facet of the systemic inequities harshly spotlighted by the pandemic. People of color are more likely to put off care than other groups. While 34% of Whites said they put off care, that percentage rose to 40% among Blacks and 36% among Latinos.
Income also played a role, as 37% of those with household incomes at or below 250% of the poverty level put off care, compared to 25% of those with incomes above that threshold.
Putting off care has had an impact industrywide, as the normally robust healthcare sector lost 30,000 jobs in January. Molina Healthcare warned last week that utilization will remain depressed for the foreseeable future.
Younger Americans were also impacted, with nearly 30% of parents saying they delayed at least one type of care for their children, while 16% delayed multiple types of care. As with adults, dental care was the most common procedure that was put off, followed by checkups or other preventative healthcare screenings.
The researchers recommended improving communications among providers and patients.
“Patients must be reassured that providers’ safety precautions follow public health guidelines, and that these precautions effectively prevent transmission in offices, clinics, and hospitals,” they wrote. “More data showing healthcare settings are not common sources of transmission and better communication with the public to promote the importance of seeking needed and routine care are also needed.”
https://www.healthcaredive.com/news/molina-expects-utilization-to-remain-depressed-in-2021/594895/

Insurers have largely remained unbruised from the pandemic, unlike some providers, but the fourth quarter was a different story.
The pandemic took a bite out of Molina’s net income in the fourth quarter as the company reported that figure fell to $34 million from $168 million in Q4 2019.
The biggest contributor to the impact on the bottom line was Medicaid refunds to states, including California, Michigan and Ohio. States have clawed back some of the money they pay insurers like Molina as members continue to defer care, which is a benefit to insurers as they then pay out less.
Molina painted a clearer picture of this scenario during Thursday’s conference call with investors.
For the full year, Molina estimated that medical cost suppression amounted to $620 million while direct COVID-19 costs amounted to $200 million. In other words, curbed utilization continued to outweigh direct COVID-19 costs, resulting in a $420 million benefit from the pandemic, which the company characterized as a surplus.
But states took back a total of $565 million through rate refunds. Overall, the net impact of COVID-19 was a $180 million hit to Molina for 2020 when factoring in other costs.
Looking ahead, executives seemed cautiously optimistic for 2021 but noted headwinds from the pandemic will persist. While the forecast reflects future growth, Zubretsky said, “it is a constrained picture” of the company’s potential earnings.
Some of those headwinds include Medicare risk scores that don’t fully capture the acuity of their Medicare members. As seniors put off care in 2020, companies like Molina were unable to capture diagnosis codes to help them determine how sick members are and the ultimate risk they pose.
Still, there are some bright spots. As the public health emergency is likely to be continued throughout the remainder of the year, it means that redeterminations will remain halted, or, in other words, Medicaid members will not be kicked off coverage.
This was a boon for Molina in 2020, as it allowed them to pick up a significant number of new members. Overall, it was a major catalyst for Medicaid membership growth in 2020, Zubretsky said.
Molina expects care utilization to improve this year but not fully return to normal. Instead, it expects utilization suppression to be about one third of 2020 levels.
Molina, which solely focuses its portfolio on government sponsored and marketplace plans, said it expects to pick up as many as 30,000 additional members during the Affordable Care Act special enrollment period.
Opening up a special enrollment period was one of the first moves made by the new administration in the White House. Zubretsky seems enthused by the recent moves through executive orders and the unfolding bill developments in Congress that are looking to raise premium subsidies on the exchanges.
Those early actions “just couldn’t be better for government sponsored managed care, and we’re pleased to see that progress already being made,” Zubretsky said.
https://mailchi.mp/41540f595c92/the-weekly-gist-february-12-2021?e=d1e747d2d8

Starting next week, millions of uninsured Americans will have the opportunity to sign up for coverage on the federal insurance marketplace, the result of President Biden’s executive order to create a 90-day special enrollment period. The graphic above highlights the potential impact of this enrollment period on the uninsured population.
According to a Kaiser Family Foundation analysis, of the nearly 15M uninsured who are marketplace-eligible, nearly 9M qualify for free or subsidized coverage. Enrollment of these individuals will come with added challenges, as they tend to be less educated, younger, more rural, and less likely to speak English, as compared to the general population. An Urban Institute survey found almost half of uninsured individuals are unfamiliar with marketplace coverage options, and nearly two-thirds lack an understanding of available financial assistance.
The federal government is dedicating $50M to advertise the special enrollment period, to assist with outreach and education. Given the population most likely to have lost insurance due to the COVID pandemic, this funding will be critical to making sure eligible people take advantage or free or low-cost coverage.

COVID-19 vaccine makers are under intense pressure to rev up production, but the scale of the challenge is unprecedented — and the speed of production is limited.
Why it matters: Even with help from the federal government and outside companies, vaccine-making is a complex, time-consuming biological process. That limits how quickly companies like Pfizer and Moderna can accelerate their output even during a crisis.
The big picture: With new, more transmissible variants emerging, we’re in a race to get shots into more people’s arms. What would normally take years to set up is being compressed into less than a year, leaving engineers to adapt manufacturing processes on the fly.
Between the lines: Making vaccines is complex, and the process can be hindered at different steps.
How it works: Axios got a deep dive into the making of Pfizer’s vaccine, a three-phase process that takes weeks from start to finish and involves three different facilities.
1) DNA manufacturing: At a plant near St. Louis, Mo., Pfizer produces DNA that encodes messenger RNA — instructions for cells to make part of the spike protein on the surface of the coronavirus. That primes the immune system to defend against future encounters with the virus.
2) Making the mRNA: In Andover, the template DNA is incubated with messenger RNA building blocks in a reactor to make the mRNA. Pfizer has been making two, 40-liter batches per week — up to 10 million doses worth —but expects to double that to four batches per week.
3) Formulating the vaccine: In Kalamazoo, the mRNA and lipid nanoparticles (oily envelopes that deliver mRNA to cells in the body) are combined and go through a series of filtrations.
Where it stands: Both Pfizer and Moderna say they’re on track to meet their commitments to deliver 200 million doses each to the U.S. over the first half of the year.
The latest: The Biden administration said last week that it will use its wartime powers under the Defense Production Act to give Pfizer priority access to critical components such as filling pumps and filtration units to try to help address bottlenecks.
Ordering other drug manufacturers to stand up manufacturing lines to whip up extra batches of Pfizer’s or Moderna’s vaccines is not an efficient or practical way for the federal government to quickly increase supplies, some experts say.
What to watch: Johnson & Johnson has requested emergency use authorization from the FDA for its single-dose vaccine, but is reportedly lagging in production, the NYT first reported last month.
