A New York physician has been charged with manslaughter in the second degree and is facing other felonies related to the overdose death of a patient, New York Attorney General Letitia James announced Feb. 19.
Sudipt Deshmukh, MD, allegedly prescribed a lethal mix of opioids and other controlled substances that resulted in the overdose death of a patient. The physician allegedly knew the patient struggled with addiction.
An indictment, unsealed Feb. 18, alleges that between 2006 and 2016, Dr. Deshmukh ignored his professional responsibilities by prescribing combinations of opioid painkillers and other controlled substances, including hydrocodone, methadone and morphine, without regard to the risk of death associated with the combinations of those drugs.
Dr. Deshmukh is facing several felony charges, including healthcare fraud, for allegedly causing Medicare to pay for medically unnecessary prescriptions.
The indictment comes after the attorney general’s office filed a felony complaint against Dr. Deshmukh in August. In 2019, the New York State Office of Professional Medical Conduct found that he committed several counts of misconduct.
With nearly 30% of workers now having a high deductible health plan and a typical family being responsible for on average the first $8,000 of costs, consumers are increasingly weighing care versus cost. Historically, with a small copay, you would conveniently take care of an ailment without shopping around, but with the average person now bearing the brunt of the initial costs, wouldn’t you want to know how much a service costs and what other providers are charging before you “buy” the service?
CMS believes“consumers should be able to know, long before they open a medical bill, roughly how much a hospital will charge for items and services it provides.” Cue the hospital price transparency rule that just went into effect January 1, 2021. Hospitals are now required to post their standard charges, including the rates they negotiate with insurers, and the discounted price a hospital is willing to accept directly from a patient if paid in cash. As a consumer, the intent is to make it “easier to shop and compare prices across hospitals and estimate the cost of care before going to the hospital.”
There are a few different angles to analyze here:
Are hospitals following the rules?
Each hospital must post online a comprehensive machine readable file with all items and services, including gross charges, actual negotiated prices with insurers, and the cash price for patients who are uninsured. Additionally, hospitals must post the costs for 300 common “shoppable” services in a “consumer-friendly format.” Some hospitals and health systems have done a good job at posting these prices in a digestible format, like the Cleveland Clinic or Sutter Health, but others have posted complicated spreadsheets, relied on online cost estimator tools, or simply not posted them at all. An analysis from consulting firm ADVI of the top 20 largest hospitals in the U.S. found that not all of them appeared to completely comply with this mandate. In some instances, data was not able to be downloaded in a useable format, others did not post the DRG or service codes, and the variability in the terms/categories used simply created difficulty in comparing pricing information across hospitals. CMS has stated that a failure to comply with the rules could result in a fine of up to $300 per day. As with most new rules, there are growing pains, and hospitals will likely get better at this over time, assuming the data is being used for its original intent.
Is this helpful to consumers?
Consumers will able to see the variation in prices for the exact same service or procedure between hospitals and get an estimate of what they will be charged before getting the care. But how likely is the average person to go to their hospital’s website, look at a price, and change their decision about where to get care? In addition, awareness of these price transparency tools is still low among consumers. Frankly, it is competitors and insurers that have been first in line to review the data. Looking through a number of hospital websites, and even certain state agency sites that have done a good job at summarizing the costs, like Florida Health Price Finder, the price transparency tools are helpful, but appear to be much more suited for relatively standardized services that can be scheduled in advance, like a knee replacement. It’s highly unlikely you will be telling your ambulance driver what hospital to go to based on cost while in cardiac arrest…Plus, it’s all still confusing – even physicians have shared their bewilderment, when trying to decipher and compare pricing. Conceptually, price transparency should be beneficial to consumers, but it will take time; and it will need to involve not just the hospitals posting rates, but the outpatient care facilities as well. Knowing what you will pay before you decide to go to a physician’s office or a clinic or an urgent care or an ED will hopefully help drive consumers to make more educated decisions in the future.
Will this ultimately drive down costs?
I sure hope so. Revealing actual negotiated prices between hospitals and insurers should push the more expensive hospitals in the area to reduce prices, especially if consumers start using the other hospitals, instead. However, it could also have an inverse effect, with lower cost hospitals insisting on a payment increase from insurers; thereby driving up costs. In the end, as has historically been the case, the market power of certain providers will likely dictate the direction of costs in a given region. That is, until both price AND quality become fully transparent and the consumer is armed with the tools to shop for the best care at the lowest cost – consumerism here we come.
The CEO of a group of Texas-based hospice and home health companies was sentenced Feb. 3 to 15 years in prison for his role in a $150 million healthcare fraud and money laundering scheme, according to the Department of Justice.
Henry McInnis was sentenced more than a year after he was convicted of conspiracy to commit healthcare fraud, conspiracy to commit money laundering, obstruction of justice and healthcare fraud.
From 2009 to 2018, Mr. McInnis and others submitted more than $150 million in false and fraudulent claims for healthcare services. The claims were submitted through Merida Group, a hospice company with dozens of locations in Texas.
Mr. McInnis was CEO of Merida. He had no medical training but acted as the director of nursing for the company. He also enforced a companywide practice of falsifying medical records to conceal the scheme and ordered employees to change medical records to make it appear patients were terminally ill.
Mr. McInnis also paid bribes to physicians to certify unqualified patients for home health and hospice.
Mr. McInnis was sentenced less than two months after the owner of Merida Group, Rodney Mesquias, was sentenced to 20 years in prison and ordered to pay $120 million in restitution.
Dallas-based Baylor Scott & White Health will outsource, lay off or retrain 1,700 employees who work in information technology, billing, revenue cycle management and other support services, according to The Dallas Morning News.
The health system said outsourcing the finance and IT jobs and other support services will help it improve efficiencies and focus on reducing costs in noncore business areas. About two-thirds of the 1,700 employees will be joining third-party RCM, IT, billing or support staff vendors.About 600 to 650 positions will be eliminated.
Baylor Scott & White said that employees whose positions are being eliminated will be invited to participate in retraining programs.
The retraining program would allow the employees to remain employed at the health system and receive the same pay or higher, depending on their role, according to the report. Some of the retraining programs that will be available are learning to become a certified medical assistant or learning a job in patient support services.
“In no case — in no case — is anyone going to miss a paycheck,” Baylor Scott & White CEO Jim Hinton, told The Dallas Morning News. “We can afford to make these commitments, and we want to do the right thing for the great employees of Baylor, Scott & White. They’ve really done everything we’ve asked and more during this last year.”
This is the third time Baylor Scott & White has announced cost-cutting initiatives related to its workforce since the pandemic began. Last May, 930 Baylor Scott & White employees were laid off, and in December the health system said it would lay off employees and outsource 102 corporate finance jobs.
Mr. Hinton said that Baylor Scott & White has 2,000 clinical positions open, and it is investing in a new regional medical school campus and a joint venture to improve care for the underinsured.
“This is a transition to a new business model, a transition to a new way of working,” Mr. Hinton told The Dallas Morning News.
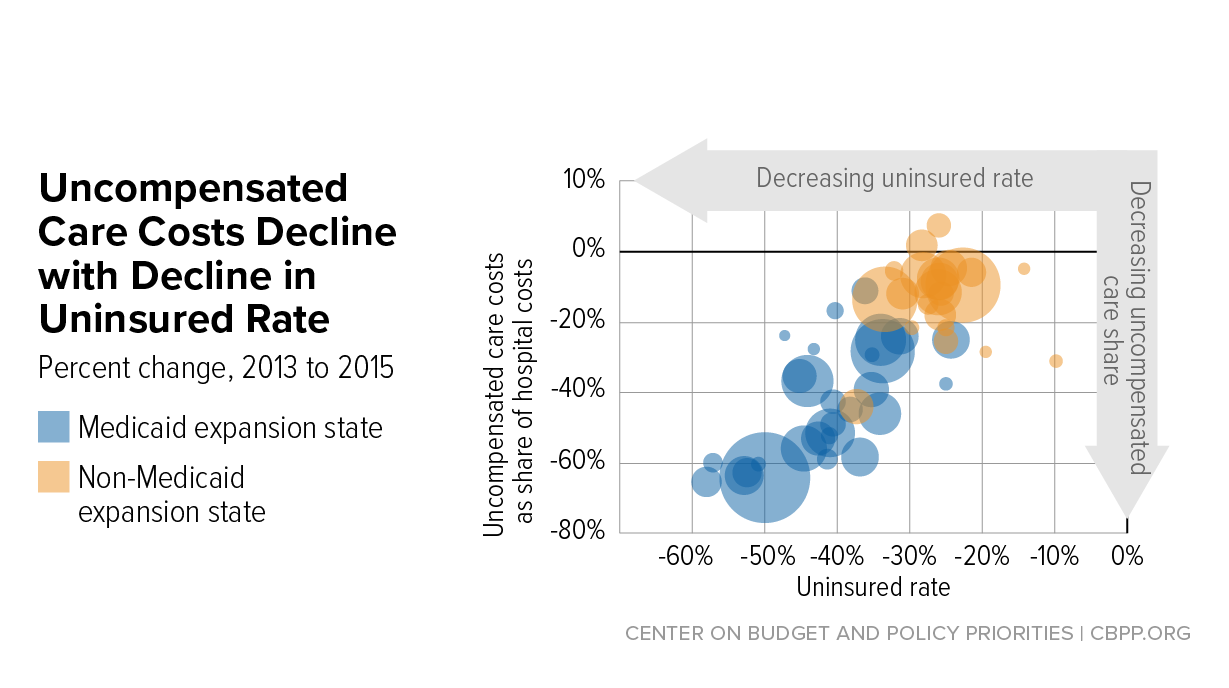
Hospital uncompensated care costs were up from $41.3B in 2018 and $38.4B in 2017, revealing an upward trend, according to AHA data.
Hospital uncompensated care costs increased right before the COVID-19 pandemic hit, according to new data from the American Hospital Association (AHA).
AHA data showed that hospitals incurred a new high of $41.61 billing in uncompensated care costs in 2019, the most recent year for which the group had complete data.
Uncompensated care costs in 2019 were up from $41.3 billion in 2018 and $38.4 billion in 2017 and were the second-highest per AHA records. Hospitals reported the most uncompensated care costs in 2013 when they incurred $46.8 billion.
Hospital uncompensated care costs decreased after the all-time high in 2013, but have recently started to tick back up after holding steady at $38.4 in 2016 and 2017.
In just the last 20 years, hospitals of all types have provided more than $660 billion in uncompensated care to patients, AHA reported. And that figure does not fully account for other ways in which provides provide financial assistance to patients of limited means, the group stated.
Each year, AHA aggregates data on uncompensated care, or care provided for which no reimbursement is received by hospitals from patients or payers. The data comes from the group’s Annual Survey of Hospitals, a comprehensive report of hospital financial data.
Uncompensated care is the sum of a hospital’s bad debt and financial assistance it provides, AHA explained.
Bad debt occurs when a hospital does not expect to obtain reimbursement for care provided, such as when patients are unable to pay their financial responsibility and do not qualify for financial assistance or are unwilling to pay their bills.
Hospitals also provide varying levels of financial assistance, AHA added. Financial assistance supports patients who cannot afford to pay and qualify for support from the hospital based on policies it has established based on the facility’s mission, financial condition, and geographic location, among other factors.
Combined, bad debt and financial assistance charges total a hospital’s uncompensated care charges, which is then multiplied by a hospital’s cost-to-charge ratio to determine total uncompensated care costs.
AHA noted that it expressed uncompensated care in costs versus charges because of significant variations in hospital payer mixes. Publishing the information as costs rather than charges enables better comparison across hospitals, the group said.
Nearly half of hospitals (48 percent) have seen bad debt and uncompensated care increase recently as a result of the ongoing COVID-19 pandemic, an analysis from consulting firm Kaufman Hall revealed.
More than 40 percent of hospitals also reported increases in percentage of uninsured or self-pay patients (44 percent) and the percentage of Medicaid patients (41 percent), which both contribute to unfunded or underfunded care at hospitals.
“The challenges brought on by the COVID-19 pandemic have affected nearly every aspect of hospital financial and clinical operations,” Lance Robinson, a managing director at Kaufman Hall, said at the time. “Organizations have responded to the challenge by adjusting their operations and strengthening important community relationships.”
Hospital uncompensated care costs – and bad debt as a result – are likely to increase in 2020 as hospitals come to terms with the impact COVID-19 has had on their financial health.
Already, hospitals have lost an estimated $323 billion in 2020 as a result of the COVID-19 pandemic, according to earlier projections from AHA.
About half of US hospitals also started the year in the red, AHA and Kaufman Hall stated in a recent report. The organizations predicted that hospital margins would sink to -7 percent in the second half of 2020 without comprehensive financial support from the government, but could decrease to a low of -11 percent if COVID-19 continued to periodically surge as it has.
Hospitals are now required to disclose the prices they secretly negotiate with insurers.
But many are dragging their feet on the new regulations, which were passed under President Donald Trump and could very well stay in place under President Biden.
The rules went into place Jan. 1, but hospital compliance is spotty.
“Hospitals are playing a hide-and-seek game,” said Ge Bai, an expert on health-care pricing at Johns Hopkins Bloomberg School of Public Health.“Even with this regulation, most of them are not being fully transparent.”
Hospitals lost a bruising court battle last year to stop the rules, which require them to publish a list of prices for goods and services. The point is to bring more transparency to prices for medical goods and services — information that has long been inaccessible to consumers. The new rules were a centerpiece of Trump’s promise to inject more price transparency in the health-care system and curb surprise billing.
But Nisha Kurani, a policy analyst at the Kaiser Family Foundation who is tracking hospital responses to the new rule, said she’s seen the full gamut.
MedStar in Washington posted its prices in an Excel sheet on its website, but other hospitals only posted price estimates, uploaded files in difficult to use formats, or promised to release information only after someone inputs their insurance, Kurani said.
A Gothamist investigation found that only one of five major New York hospitals posted a list of their negotiated services to their website, and even then, not for all procedures. The fine for not complying with the new rules — $300 a day — is a drop in the bucket for many hospitals.
The rules probably aren’t going away anytime soon.
The Biden administration hasn’t taken any public position on the rules — and right now, officials are focused on reversing dozens of other Trump administration regulations they believe are damaging to health insurance and costs in the United States.
Revising the hospital transparency rules — if that’s even something the new administration wants to do — would likely be far down on the priority list, despite heavy lobbying by the hospital industry to suspend enforcement of the new rule.
Plus, price transparency is broadly popular among the public and was one of the planks of a joint health policy plan developed by a task force Biden formed with Sen. Bernie Sanders (I-Vt.) after the 2020 primary elections.
The American Hospital Association says staff who would help with compliance are stretched thin.
Molly Smith, the association’s group vice president for public policy, said many of the staff members who would normally be tasked with compiling and formatting the price data are the same people being asked to help set up patient registries and vaccine tracking systems in response to the pandemic.
“We’ve got a lot of hospitals that are at or beyond capacity,” Smith said.
A lawyer for the hospital association said that it is considering petitioning its legal case to the Supreme Court. Meanwhile, the lobbying group has been pushing the Biden administration to suspend enforcement of the new rule.
Consumer advocates like the transparency rules designed to protect patients and drive down health-care costs.
“In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the health-care system,” said Cynthia Fisher, head of the nonprofit Patient Rights Advocate, which pushes for price transparency.
But now, Fisher says, “it’s the American consumer who is going to drive down the cost of care.”
But the effect might be modest.
Experts in health-care economics hotly debate whether the price transparency rules will, in fact, drive down costs. Even those who support the changes say the effect might be incremental.
“I don’t think it’s going to be an earthquake in terms of pricing, but it’s a first step in the right direction,” said Bai.
There are several reasons the new price transparency rule may not have a massive effect on hospital prices. Perhaps the biggest, and one often cited by the hospital lobby, is that most Americans are not going to pay the negotiated price for a procedure. Instead, they are likely to pay co-pays or coinsurance that amount to a fraction of this price.
This isn’t always true, of course. Those with high-deductible plans may pay the negotiated rate, and for those without insurance paying out of pocket, it can be helpful to get a peek behind the sticker price. But even for these patients, it may be challenging to extract useful information from unwieldy spreadsheets full of obscure billing codes.
Bai said that she is hopeful that third parties may make some of the pricing information easier for consumers to use. And some self-insured employers may start identifying cheaper providers and incentivizing patients to use them. The rules also require hospitals to provide cost-sharing estimates for commonly used procedures in an easily navigable format.
Still, price competition works only if there are players to compete.
The market for health care has become increasingly consolidated as hospitals merge and buy up physician practices. If a hospital is the only health-care provider in town, then there’s not a whole lot patients can do about high prices, even if they think they’re unfair.
“I don’t think transparency will fundamentally change the power balance between the payer and the hospital in many markets,” Bai said.
Chicago-based CommonSpirit and Blue Shield of California expanded a new billing program to 20 Dignity Health hospitals, the organizations said Jan. 11.
The Member Payments billing program aims to create faster and more transparent billing processes for Blue Shield of California members who receive care at Dignity facilities and owe money after their insurance is processed. CommonSpirit is the parent organization of Sacramento, Calif.-based Dignity.
Under the program, Dignity can get a patient’s portion of a bill at the time of claim adjudication. Patients who receive care from a Dignity facility get a monthly bill from Blue Shield of California. Through that bill, patients can then pay for their cost-sharing amount in full or through installments.
The program, announced in 2018, was launched in September 2019 by Dignity, CommonSpirit, Blue Shield of California and technology startup company Ooda Health. The program’s 12-month pilot started at two hospitals in Sacramento and grew to six hospitals by the end of the pilot year.
The addition of 20 Dignity hospitals comes after the process was found to streamline cost-sharing payments, resulting in a 92 percent satisfaction rate from patients who used the platform, the organizations said.
Fewer than four in every 10 American adults can afford a $1,000 surprise medical bill, according to survey results released Jan. 11 by finance company Bankrate.
Bankrate surveyed 1,003 Americans about their personal finances from Dec. 8 to 13, finding a 2 percent drop from the previous year in respondents who said they could comfortably cover a $1,000 expense. The study noted that credit card finance charges can often add up to hundreds of additional dollars when surprise expenses are not paid quickly.
However, some Americans have an optimistic outlook on their financial situation going forward, with 44 percent of respondents believing their personal finances will improve in 2021.