The U.S. health industry revolves around a flawed presumption: individuals and families are dependent on the health system to make health decisions on their behalf. It’s as basic as baseball and apple pie in our collective world view.
It’s understandable. Consumers think the system is complex. They believe the science on which diagnostics and therapeutics are based requires specialized training to grasp. They think health insurance is a hedge against unforeseen bills that can wipe them out. And they think everything in healthcare is inexplicably expensive.
This view justifies the majority of capital investments, policy changes and competitive strategies by organizations geared to protecting traditional roles and profits. It justifies guardianship of scope of practice limits controlled by medical societies because patients trust doctors more than others. It justifies pushback by hospitals, insurers and drug companies against pro-price transparency regulations arguing out-of-pocket costs matter more. It justifies mainstream media inattention to the how the health system operates preferring sensationalism (medical errors, price sticker shock, fraud) over more complicated issues. And it justifies large and growing disparities in healthcare workforce compensation ranging from hourly workers who can’t afford their own healthcare to clinicians and executives who enjoy high six figure base compensation and rich benefits awarded by board compensation committees.
It’s a flawed presumption. It’s the unintended consequence of a system designed around sick care for the elderly that working age populations are obliged to fund. Healthcare organizations should pivot because this view is a relic of healthcare’s past. Consider:
- Most consumers think the health system is fundamentally flawed because it prioritizes its business interests above their concerns and problems.
- Most think technologies—monitoring devices, AI, et al– will enable them to own their medical records, self-diagnose and monitor their health independently.
- And most –especially young and middle age consumers—think their healthcare spending should be predictable and prices transparent.
In response, most organizations in healthcare take cautious approaches i.e. “affordability” is opined as a concern but defined explicitly by few if any. “Value” is promised but left to vague, self-serving context and conditions. “Quality” is about affiliations, capabilities and processes for which compliance can be measured but results (outcomes, diagnostic accuracy, efficacy, savings, coverage adequacy, et al) — hardly accessible. And so on.
For starters, the industry must address its prices, costs and affordability in the broader context of household discretionary spending. Healthcare’s insiders are prone to mistaken notions that the household healthcare spend is somehow insulated from outside forces: that’s wrong. Household healthcare expenditures constitute 8.3% of the monthly consumer price index (CPI); housing is 35.4%, food is 13.6% and energy is 6.4%. In the last 12 months, the overall CPI increased 2.9%, healthcare services increased 4.2%, housing increased 3.6%, food increased 3.2% and energy costs increased only 0.2%. In that same period, private industry wages increased 1.0% and government wages increased 1.2%. Household financial pressures are real and pervasive. Thus, healthcare services costs are complicit in mounting household financial anxiety.
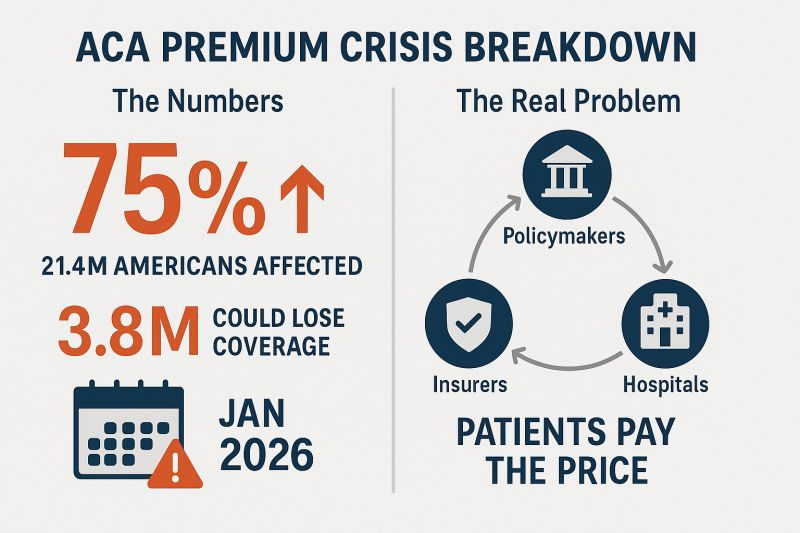
The pending loss of marketplace subsidies and escalating insurance premiums means households will be expected to spend more for healthcare. Housing market instability that hits younger and lower-middle income households hardest poses an even larger threat to household financial security and looms large in coming months. Utilization of healthcare products and services in households during economic downturns shrinks some, but discretionary spending for health services—visits, procedures, tests, premiums, OTC et al—shrinks substantially as those bills take a back seat to groceries, fuel, car payments, student loan debt, rent/mortgage payments and utilities in most households.
Healthcare organizations must rethink their orientations to patients, enrollees and users. All must embrace consumer-facing technologies that empower individuals and households to shop for healthcare products and services deliberately. In this regard, some insurers and employers seem more inclined than providers and suppliers, but solutions are not widely available. And incentives to stimulate households to choose “high value” options are illusory. Data show carrots to make prudent choices work some, but sticks seem to stimulate shopping for most preference-sensitive products and services.
The point is this: the U.S. economy is slowing. Inflation is a concern and prices for household goods and necessary services are going up. The U.S. health industry can ill-afford to take a business-as-usual approach to how our prices are set and communicated, consumer debt collection (aka “rev cycle”) is managed and how capital and programmatic priorities are evaluated.
Net Promoter Scores, Top 100 Recognition and Star Ratings matter: how organizations address household financial pressures impacts these directly and quickly. And, as never before, consumer sentiment toward healthcare’s responsiveness to their financial pressures is at an all-time low. It’s the imperative that can’t be neglected.