
Cartoon – Competition is Killing Me



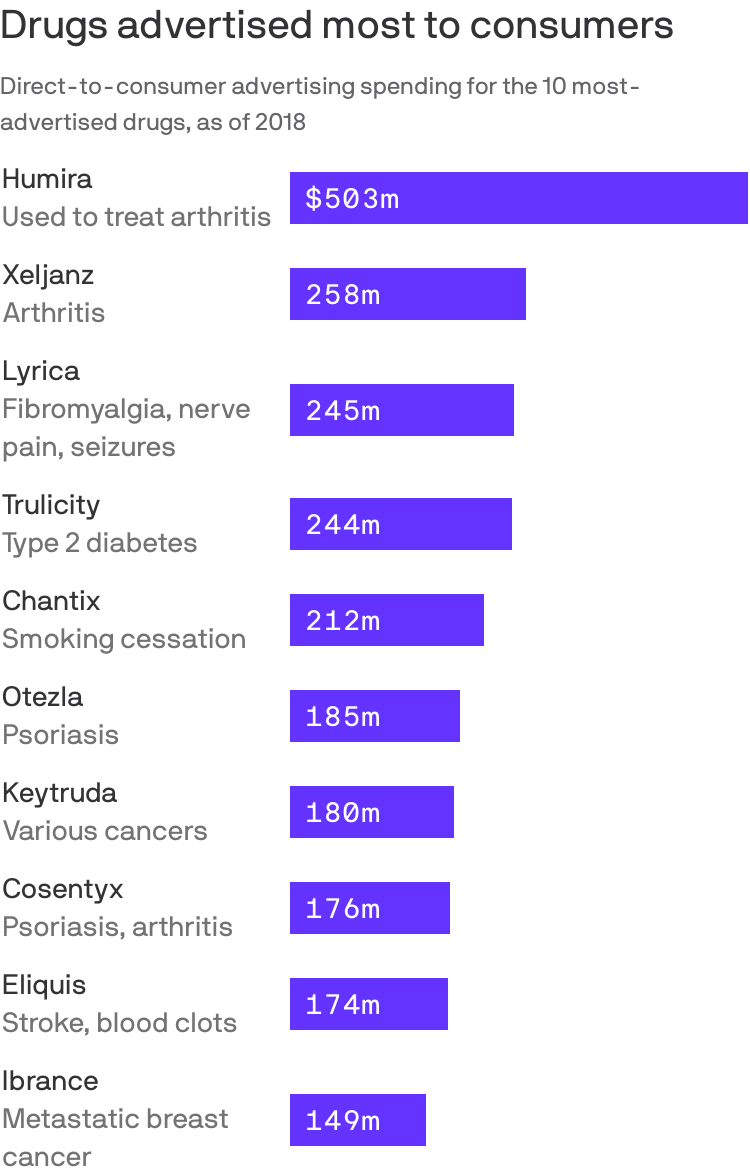
Prescription drugs with some of the highest Medicare spending also had the highest level of direct-to-consumer advertising, a recently-released GAO report found.
By the numbers: The GAO found the Medicare program and its beneficiaries spent nearly $324 billion on prescription drugs advertised to beneficiaries and other consumers between 2016 and 2018.
This amount is more than half (58%) of total Medicare Parts B and D spending on drugs during that time, the most recent data available.

With a $56,000-a-year price tag, Biogen’s newly approved Alzheimer’s drug Aduhelm is dovetailing into the debate on Capitol Hill over how to lower prescription drug prices.
Why it matters: Democrats may be positioning themselves to push policy measures that assign value to drugs and then price them accordingly — a huge potential blow to the pharmaceutical industry.
To truly address its launch price, policymakers have to grapple with big questions the U.S. system currently avoids: How should we determine the value of a drug, and who gets to make that decision?
The bottom line: “Any kind of process for valuing new drugs like Aduhelm take you immediately into the controversial quagmire of how to quantify improvements in quality of life for people,” said KFF’s Larry Levitt.

It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Leading systems will do it soon.
Laggards will get there eventually.
Joining the growing tide of vaccine mandates are a variety of systems and hospitals, including Mass General Brigham in Boston, BJC Healthcare in St. Louis and Inova Health System in Virginia.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,” AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
As the delta variant of the coronavirus spreads, especially among the unvaccinated, the Biden administration is gearing up for a new push to vaccinate the so-called “movable middle”—and some public health experts say FDA could advance that goal by fully approving Covid-19 vaccines.
According to an analysis by the Associated Press, nearly all recent Covid-19 deaths have occurred in unvaccinated individuals.
The AP analysis is based on data from CDC, although CDC has not itself released estimates of the share of Covid-19 deaths among unvaccinated patients.
According to the AP analysis, just 0.8% of Covid-19 deaths in May were among the fully vaccinated. Meanwhile, the share of hospitalized patients who were fully vaccinated was just 0.1% in May, with fewer than 1,200 fully vaccinated people hospitalized out of more than 853,000 hospitalizations.
Meanwhile, according to CDC, 54% of the U.S. population, including 66% of American adults, have received at least one dose of a Covid-19 vaccine, while 46.1% of the total population and 56.8% of American adults have received all required doses.
In many places across the United States, COVID-19 feels over. Unmasked citizens run rampant. New York City is planning an August mega-concert in Central Park. I’m as hopeful as the rest of us, but I think we may be suffering from memory loss.
Let’s start from this time last year, when many Americans were exuberantly returning to newly reopened beaches, parks and restaurants after a seemingly eternal three months—three whole months!—of quarantine. Universal observance of safety guidelines was surely going to be sufficient to limit viral spread.
We know how that turned out. By mid-June 2020, there were already signs that our bleary-eyed re-emergence was premature. On June 22, 2020, the number of new daily cases of COVID-19 (33,485) surpassed the high-water mark hit on the worst day of the horrific first surge, when that figure peaked at just over 32,000.
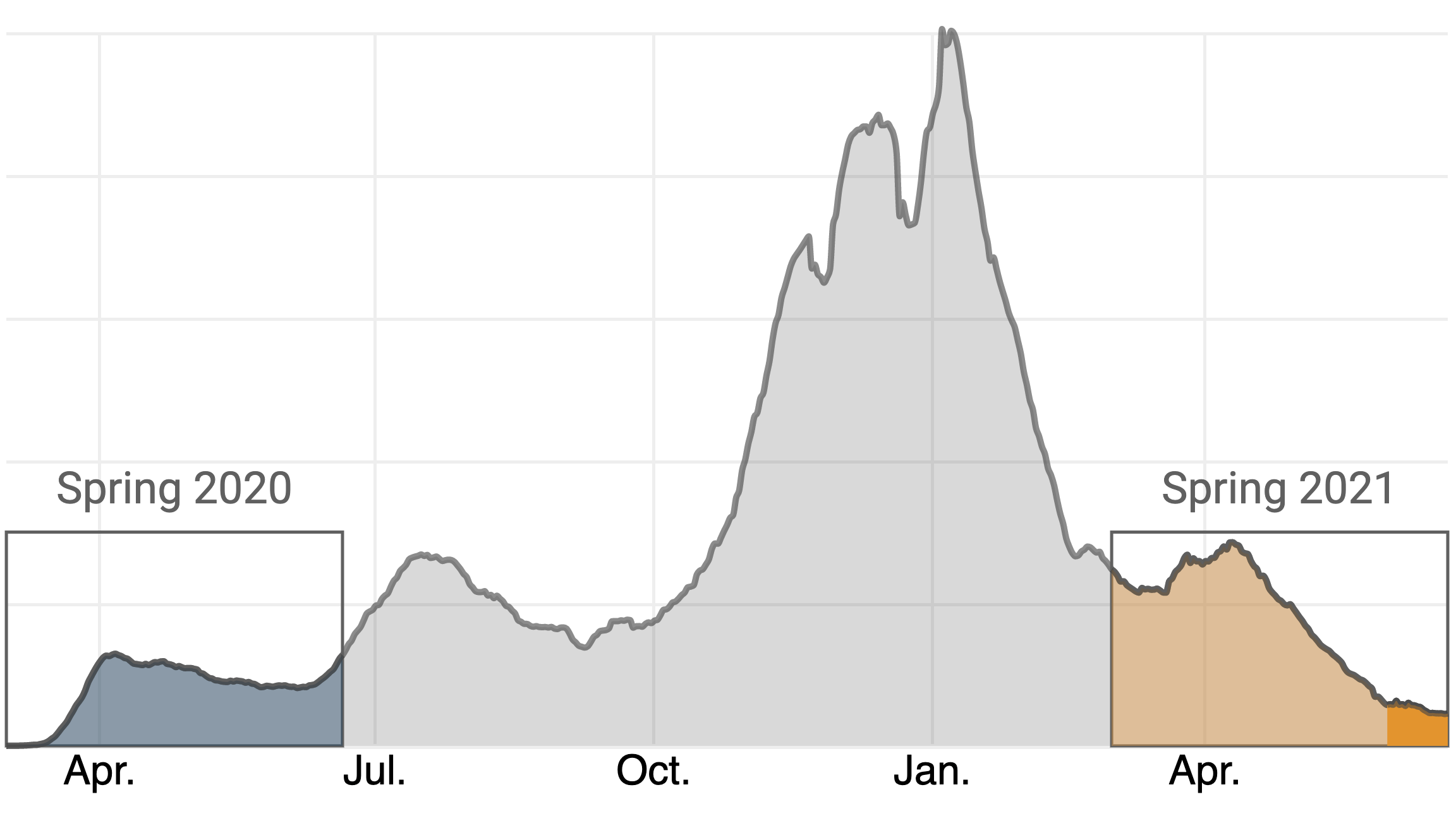
A year later, the daily case count is not as foreboding—nor is it nearly as low it may appear.
You’ll notice that this graph covers only the past 12 weeks, while virtually every chart you’ll find (including the one on TIME’s dashboard) graphs COVID-19 cases from the beginning of the outbreak. This is intentional. The toll of the pandemic in the U.S. has persisted for so long, and reached such catastrophic heights in the first weeks of 2021, that patterns such as this one are nearly impossible to see on the typical chart. Here’s what the same graph looks like against that backdrop:
My fear is that the pandemic remains much more deadly than how it looks on the page. Yes, deaths remain on a steady decline, having recently sunk below 300 people a day on average for the first time since March 24, 2020, right around the time that many offices were shuttering. But a surge in cases, particularly among the large number of unvaccinated Americans, could quickly reverse that decline.
As you can see, it has been less than a month since the 2021 case count sunk below the year-over-year figure, on May 26. The massive nationwide vaccine rollout is undoubtedly a major factor, but it’s difficult to quantify the impact of vaccination on the currently low case and death figures. There are only weak correlations between states’ vaccination rates and some key indicators, like the rate at which cases have risen or fallen in recent weeks.
What we can quantify is that, in the 27 days since the lines crossed, the vaccination rate in the U.S. has only crawled upward, from 39.7% to 45.3% of Americans who have received a complete dosage. While the official vaccination rate applies to the entire population, data from the U.S. Centers for Disease Control and Prevention (CDC) also includes percentages for several age groups. By TIME’s calculations, there are 97.4 million adults age 18 and over who have been eligible for vaccination for two months but who have not yet received even a first dose. This group trends heavily younger, with those 65 and over representing only 7.8% of the unvaccinated population. (These figures do no include those under 18, who constitute a small portion of the eligible population.)
On May 13, two weeks before daily case numbers in 2021 fell below the year-over-year figures from the same day in 2020, the CDC issued guidance liberating fully vaccinated individuals from wearing masks in many scenarios. I do not have conclusive proof that any of the country’s 97.4 million unvaccinated adults have abused this privilege. All I can state with confidence is that, based on the number of people I’ve seen not wearing a mask in places like stores, which often have signs imploring those who are not fully vaccinated to continue to mask up, it is mathematically almost certain that more than a few have done so.
Which is to say: the situation today, if one can momentarily rewind to Memorial Day of 2020, feels very familiar. There appears to be a lambent light at the end of the tunnel, yet cavalier attitudes towards the pandemic, particularly among younger people who, as a group, are under-vaccinated, resembles what we saw last summer just before the second wave.
Watching these trends, I grow more concerned every day that the country is positioned for yet another surge in cases, despite our defensive upgrades in the off-season. I hope I’m wrong, but the numbers are not nearly as comforting as they first look. The fact that the Delta variant, which is both more transmissible and appears to cause more severe disease, is on pace to become the dominant form of COVID-19 in the U.S. in the coming months is further reason for alarm. Moreover, some states have significantly higher vaccination rates than others, leaving those with less protection more vulnerable to future spikes.
Forgive me for being a buzzkill, but unless we can institute a functional vaccine passport system, which appears unlikely, I do not think it is wise to assume that every unmasked individual is fully dosed. Short of a passport system, and with dangerous variants competing for dominance and the duration of vaccine protection still unclear, we ought to continue to ration physical space in public areas—a policy that is hastily being relaxed at places like Major League Baseball parks. I love baseball and eagerly look forward to buzzing up to Philadelphia to take in a game at Citizen’s Bank Park, which is operating at full capacity. But not while the policy is that “Unvaccinated fans are strongly encouraged to wear their masks in all indoor and outdoor areas in and around the ballpark.”
I also think there might be a backdoor to a digital passport system. Based on polling data, it appears there is a substantial population of people who aren’t categorically opposed to vaccination, just unmotivated to get around to it—what we’ve termed vaccine “meh-sitance,” not hesitance. My proposal is that bars, restaurants and other popular venues merely require each person who enters to verbally affirm that they are fully vaccinated.
This might sound about as effective as asking passengers in the exit row to individually verify that they listened to the instructions. But while it’s one thing to ignore a sign at the grocery store, it’s another to lie in front of your friends. Peer pressure is a powerful motivator, and if even a fraction of the unvaccinated would take the time to resolve that dissonance, or risk missing out on trivia night, it could substantially push up the percentages. I call this the “FOMO method,” and though we are still a long, long way from eliminating the disease altogether, it could help us avert a fourth wave this summer.

The Biden administration is quietly engineering a series of expansions to Medicaid that may bolster protections for millions of low-income Americans and bring more people into the program.
Biden’s efforts — which have been largely overshadowed by other economic and health initiatives — represent an abrupt reversal of the Trump administration’s moves to scale back the safety-net program.
The changes could further boost Medicaid enrollment — which the pandemic has already pushed to a record 80.5 million. Some of the expansion is funded by the COVID-19 relief bill that passed in March, including coverage for new mothers.
Others who could also gain coverage under Biden are inmates and undocumented immigrants. At the same time, the administration is opening the door to new Medicaid-funded services such as food and housing that the government insurance plan hasn’t traditionally offered.
“There is a paradigm change underway,” said Jennifer Langer Jacobs, Medicaid director in New Jersey, one of a growing number of states trying to expand home-based Medicaid services to keep enrollees out of nursing homes and other institutions.
“We’ve had discussions at the federal level in the last 90 days that are completely different from where we’ve ever been before,” Langer Jacobs said.
Taken together, the Medicaid moves represent some of the most substantive shifts in federal health policy undertaken by the new administration.
“They are taking very bold action,” said Rutgers University political scientist Frank Thompson, an expert on Medicaid history, noting in particular the administration’s swift reversal of Trump policies. “There really isn’t a precedent.”
The Biden administration seems unlikely to achieve what remains the holy grail for Medicaid advocates: getting 12 holdout states, including Texas and Florida, to expand Medicaid coverage to low-income working-age adults through the Affordable Care Act.
And while some of the recent expansions – including for new mothers — were funded by close to $20 billion in new Medicaid funding in the COVID relief bill Biden signed in March, much of that new money will stop in a few years unless Congress appropriates additional money.
The White House strategy has risks. Medicaid, which swelled after enactment of the 2010 health law, has expanded further during the economic downturn caused by the pandemic, pushing enrollment to a record 80.5 million, including those served by the related Children’s Health Insurance Program. That’s up from 70 million before the COVID crisis began.
The programs now cost taxpayers more than $600 billion a year. And although the federal government will cover most of the cost of the Biden-backed expansions, surging Medicaid spending is a growing burden on state budgets.
The costs of expansion are a frequent target of conservative critics, including Trump officials like Seema Verma, the former administrator of the Centers for Medicare & Medicaid Services, who frequently argued for enrollment restrictions and derided Medicaid as low-quality coverage.
But even less partisan experts warn that Medicaid, which was created to provide medical care to low-income Americans, can’t make up for all the inadequacies in government housing, food and education programs.
“Focusing on the social drivers of health … is critically important in improving the health and well-being of Medicaid beneficiaries. But that doesn’t mean that Medicaid can or should be responsible for paying for all of those services,” said Matt Salo, head of the National Association of Medicaid Directors, noting that the program’s financing “is simply not capable of sustaining those investments.”
Restoring federal support
However, after four years of Trump administration efforts to scale back coverage, Biden and his appointees appear intent on not only restoring federal support for Medicaid, but also boosting the program’s reach.
“I think what we learned during the repeal-and-replace debate is just how much people in this country care about the Medicaid program and how it’s a lifeline to millions,” Biden’s new Medicare and Medicaid administrator, Chiquita Brooks-LaSure, told KHN, calling the program a “backbone to our country.“
The Biden administration has already withdrawn permission the Trump administration had granted Arkansas and New Hampshire to place work requirements on some Medicaid enrollees.
In April, Biden blocked a multibillion-dollar Trump administration initiative to prop up Texas hospitals that care for uninsured patients, a policy that many critics said effectively discouraged Texas from expanding Medicaid coverage through the Affordable Care Act, often called Obamacare. Texas has the highest uninsured rate in the nation.
The moves have drawn criticism from Republicans, some of whom accuse the new administration of trampling states’ rights to run their Medicaid programs as they choose.
“Biden is reasserting a larger federal role and not deferring to states,” said Josh Archambault, a senior fellow at the conservative Foundation for Government Accountability.
But Biden’s early initiatives have been widely hailed by patient advocates, public health experts and state officials in many blue states.
“It’s a breath of fresh air,” said Kim Bimestefer, head of Colorado’s Department of Health Care Policy and Financing.
Chuck Ingoglia, head of the National Council for Mental Wellbeing, said: “To be in an environment where people are talking about expanding health care access has made an enormous difference.”
Mounting evidence shows that expanded Medicaid coverage improves enrollees’ health, as surveys and mortality data in recent years have identified greater health improvements in states that expanded Medicaid through the 2010 health law versus states that did not.
Broadening eligibility
In addition to removing Medicaid restrictions imposed by Trump administration officials, the Biden administration has backed a series of expansions to broaden eligibility and add services enrollees can receive.
Biden supported a provision in the COVID relief bill that gives states the option to extend Medicaid to new mothers for up to a year after they give birth. Many experts say such coverage could help reduce the U.S. maternal mortality rate, which is far higher than rates in other wealthy nations.
Several states, including Illinois and New Jersey, had sought permission from the Trump administration for such expanded coverage, but their requests languished.
The COVID relief bill — which passed without Republican support — also provides additional Medicaid money to states to set up mobile crisis services for people facing mental health or substance use emergencies, further broadening Medicaid’s reach.
And states will get billions more to expand so-called home and community-based services such as help with cooking, bathing and other basic activities that can prevent Medicaid enrollees from having to be admitted to expensive nursing homes or other institutions.
Perhaps the most far-reaching Medicaid expansions being considered by the Biden administration would push the government health plan into covering services not traditionally considered health care, such as housing.
This reflects an emerging consensus among health policy experts that investments in some non-medical services can ultimately save Medicaid money by keeping patients out of the hospital.
In recent years, Medicaid officials in red and blue states — including Arizona, California, Illinois, Maryland and Washington — have begun exploring ways to provide rental assistance to select Medicaid enrollees to prevent medical complications linked to homelessness.
The Trump administration took steps to support similar efforts, clearing Medicare Advantage health plans to offer some enrollees non-medical benefits such as food, housing aid and assistance with utilities.
But state officials across the country said the new administration has signaled more support for both expanding current home-based services and adding new ones.
That has made a big difference, said Kate McEvoy, who directs Connecticut’s Medicaid program. “There was a lot of discussion in the Trump administration,” she said, “but not the capital to do it.”
Other states are looking to the new administration to back efforts to expand Medicaid to inmates with mental health conditions and drug addiction so they can connect more easily to treatment once released.
Kentucky health secretary Eric Friedlander said he is hopeful federal officials will sign off on his state’s initiative.
Still other states, such as California, say they are getting a more receptive audience in Washington for proposals to expand coverage to immigrants who are in the country without authorization, a step public health experts say can help improve community health and slow the spread of communicable diseases.
“Covering all Californians is critical to our mission,” said Jacey Cooper, director of California’s Medicaid program, known as Medi-Cal. “We really feel like the new administration is helping us ensure that everyone has access.”
The Trump administration moved to restrict even authorized immigrants’ access to the health care safety net, including the “public charge” rule that allowed immigration authorities to deny green cards to applicants if they used public programs such as Medicaid. In March, Biden abandoned that rule.
