

Cartoon – Actual Results Indicate

A lawsuit filed last week accuses RWJBarnabas Health of “a years-long systemic effort” to hamper competition and monopolize acute care hospital services in northern New Jersey.
The case brought by CarePoint Health to a U.S. District Court accuses the state’s largest integrated healthcare delivery system of “aiming to destroy the three hospitals operated by CarePoint as independent competitors” with the support of healthcare real estate investors and Horizon Blue Cross Blue Shield, the state’s largest health insurer.
CarePoint Health includes the 349-bed Christ Hospital, 224-bed Bayonne Medical and 348-bed Hoboken University Medical Center (HUMC).
The group said RWJBarnabas intended to force the first two hospitals to shut down but acquire the third due to its more profitable payer mix.
“RWJBarnabas Health’s] goal explicitly disregarded the needs of the poor, underinsured and charity care patients which CarePoint serves in its role as the safety net hospital system in Jersey City and surrounding areas,” CarePoint wrote in the lawsuit.
The slew of alleged tactics listed in the lawsuit largely surround RWJBarnabas Health’s “serial acquisitions” of hospitals, providers and real estate that “has gone unchecked by the state and [New Jersey Department of Health],” CarePoint wrote.
This included an alleged bad faith proposal to acquire Christ Hospital and HUMC, the true intent of which CarePoint said was to “gain market knowledge and gather competitive intelligence, and use this newly-acquired information to freeze programmatic growth and any significant hiring or construction at Christ Hospital.” The process had a negative impact on CarePoint’s employee retention and staffing, according to the suit.
The plaintiff also alleged that RWJBarnabas used its political connections to influence whether state departments granted CarePoint Certificates of Need for multiple revenue-generating projects as well as COVID-19 relief funding.
Further, CarePoint accused RWJBarnabas of strategically adjusting its service offerings in competitive markets to drive uninsured or underinsured patients to CarePoint facilities while using its relationships with Horizon and ambulance operators to drive emergency room traffic and well-insured patients, respectively, to competing locations.
These collective actions constitute violations of the Sherman Antitrust Act as well as the New Jersey Antitrust Act, CarePoint wrote.
“The idea that [RWJBarnabas Health] would use its influence to jeopardize the health of that community and the care providers of a competing hospital not only directly contradicts its own vision, but clearly demonstrates that [RWJBarnabas Health] is far more interested in anti-competitive and predatory business activities than serving the New Jersey community,” CarePoint wrote.
RWJBarnabas Health discounted the allegations in an email statement.
“This is yet another in a series of baseless complaints filed by CarePoint, an organization whose leadership apparently prefers to assign blame to others rather than accept responsibility for the unsatisfactory results of their own poor business decisions and actions over the years,” a spokesperson for the system told Fierce Healthcare. “RWJBarnabas Health has a longstanding commitment to serve the residents of Hudson County, and is proud of the significant investments we have made in technology, facilities and clinical teams as we advance our mission.”
RWJBarnabas Health treats over 3 million patients per year and employs 37,000 people. The academic healthcare system runs 12 acute care hospitals and four specialty hospitals alongside other locations and services. It disclosed more than $6.6 billion in total operating revenues across 2021.
The system’s merger and acquisition activity placed it in the federal spotlight this past year after the Federal Trade Commission moved to block its planned integration of New Brunswick-based Saint Peter’s Healthcare System. The deal was called off in June.

However cynical it may seem, Machiavelli’s The Prince has long been recognized as a source of insights for anyone trying run a business or gain power in one. A ferocious little treatise of under 100 pages, The Prince was aimed at Lorenzo de’ Medici, the iron-handed Florentine ruler, by an author hoping to regain the proximity to power that he formerly enjoyed.
But modern corporations aren’t principalities ruled by autocrats. They are, in fact, more like republics, their leaders dependent on the support of directors, employees, customers, investors, and one another. That is why, in turning to Machiavelli for management wisdom, we would be well served to leave aside The Prince in favor of another of his works, one that is less known but perhaps more to the point. Don’t be fooled by the academic-sounding title; Discourses on Livy has a great deal to teach us about leadership in any organization resembling a republic. Chances are, that includes your business.
Published posthumously in 1531, Discourses draws on the ancient Roman historian (among others) to analyze the nature of power in public life. Like The Prince, this is not a handbook for saints. But the author was a brilliant student of human nature, and not one to underestimate the potential of a determined individual. In Discourses, he firmly asserts the importance of an individual founder in establishing or renovating a republic—and by extension, for our purposes, a business. A prudent founder, he writes, “must strive to assume sole authority.”
Yet a single person cannot sustain an enterprise in the long run. That is only possible if the founder’s vision and talents result in an institution supported by stakeholders who can carry the venture into the future. “Kingdoms which depend only upon the exceptional ability of a single man are not long enduring,” Machiavelli writes, “because such talent disappears with the life of the man, and rarely does it happen to be restored in his successor.”
Besides, princes have no monopoly on wisdom. Despite the notorious unpredictability of the mob, the author acknowledged the wisdom of crowds when he asserted that “the multitude is wiser and more constant than a prince.” Machiavelli was also insightful about succession: “After an excellent prince, a weak prince can maintain himself,” he observed with admirable economy in one chapter’s epigraph, “but after a weak prince, no kingdom can be maintained with another weak one.”
Many of the epigraphs are bull’s-eyes of this kind. Take this one, for example: “Whoever wishes to reform a long-established state in a free city should retain at least the appearance of its ancient ways.” This is worth doing even if you make massive changes, because, Machiavelli notes, “men in general live as much by appearances as by realities; indeed, they are often moved more by things as they appear than by things as they really are.”
Honesty may be the best policy, but that is not a maxim ever attributed to Machiavelli. In keeping with the notion that people attend largely to appearances, he says leaders compelled to do something by necessity should consider pretending their course of action was undertaken out of generosity. In another chapter, he argues, “Cunning and deceit will serve a man better than force to rise from a base condition to great fortune.”
Machiavelli, of course, took a hard-headed view of humanity, believing that people act largely out of self-interest, whether to gratify their egos or sate their desire for material wealth, and that, for better or worse, actions tend to be judged by their consequences. Indeed, he was very much what philosophers call a consequentialist, arguing that, in some contexts, bad things must be done to achieve good ends achievable in no other way. This is not to say that law-breaking or other unethical acts are justified—even some of Machiavelli’s contemporaries considered such advice controversial—but every business leader knows that hard decisions must be made, be it the closing of a venerable division or taking a company in a risky new direction, for the long-term good of the enterprise.
Even when advocating something like mercy, Machiavelli did so with consequences in mind. He argued, for example, that failure should not be harshly punished, especially if it arises from ignorance rather than malice. Roman generals, he notes, had difficult and dangerous jobs, and Rome understood that if military leaders had to worry about “examples of Roman commanders who had been crucified or otherwise put to death when they had lost a day’s battles, it would be impossible for that commander, beset by so many suspicions, to make courageous decisions.”
If punishment should not be meted out lightly, neither should rewards be delayed. If you don’t cultivate loyalty and support from others in good times through open-handedness, Machiavelli says, those people certainly won’t have your back when things get rough. Doling out rewards only in the face of tough competition or harsh circumstances will lead subordinates to believe “that they gained this favour not from you but from your adversaries, and since they must fear that after the danger has passed you will take back from them what you have been forced to give them, they will feel no obligation to you whatsoever.”
Republics, in his view, have no choice but to grow, for “it is impossible for a republic to succeed in standing still.” Companies are the same. But acquisitions—whether in battle or by purchase—must be carried out with care, for “conquests made by republics which are not well organized, and which do not proceed according to Roman standards of excellence, bring about their ruin rather than their glorification.”
Finally, Machiavelli was well aware of the risks of advice-giving, so much so that he gave one chapter the title “Of the danger of being prominent in counselling any enterprise, and how that danger increases with the importance of such enterprise.” Consultants, take note. Just don’t let the clients catch you reading Machiavelli.
https://www.washingtonpost.com/business/2022/09/12/minnesota-nurses-strike/

About 15,000 nurses in Minnesota walked off the job Monday to protest understaffing and overwork — marking the largest strike of private-sector nurses in U.S. history.
Slated to last three days, the strike spotlights nationwide nursing shortages exacerbated by the coronavirus pandemic that often result in patients not receiving adequate care. Tensions remain high between nurses and health-care administrators across the country, and there are signs that work stoppages could spread to other states.
Minnesota nurses charge that some units go without a lead nurse on duty and that nurses fresh out of school are delegated assignments typically held by more experienced nurses, across some 16 hospitals where strikes are expected.
The nurses are demanding a role in staffing plans, changes to shift scheduling practices and higher wages.
“I can’t give my patients the care they deserve,” said Chris Rubesch, the vice president of the Minnesota Nurses Association and a nurse at Essentia Health in Duluth. “Call lights go unanswered. Patients should only be waiting for a few seconds or minutes if they’ve soiled themselves or their oxygen came unplugged or they need to go to the bathroom, but that can take 10 minutes or more. Those are things that can’t wait.”
Paul Omodt, a spokesman for the Twin Cities Hospital Group, which represents four hospital systems where nurses are striking in the Minneapolis-St. Paul area, said that the nurses union did not do everything it could to avoid a strike.
“Nurses have steadfastly refused to go to mediation,” Omodt said. “Their choice is to strike. This strike is on the nurses.”
Conny Bergerson, a spokeswoman for Allina Health, another hospital system in the Twin Cities where nurses are on strike, said “rushing to a strike before exhausting all options such as engaging a neutral federal mediator does not benefit our employees, patients or the communities we serve.”
The Minnesota Nurses Association, the nurses union, said hospital administrators have continued to “refuse solutions” on understaffing and safety in contract negotiations. It said nurses have increasingly been asked to take on more patients for bedside care to make up for labor shortages, exacerbating burnout and high turnover.
Some hospitals have offered increased safety protocols for reporting security incidents in negotiations, but have not budged on other safety- and staffing-related demands.
The union has proposed new mechanisms for nurses to have a stronger say in how wards are staffed, including a committee made up of nurses and management at each hospital that would determine appropriate staffing levels. It has also proposed protections against retaliation for nurses who report understaffing. Striking nurses at some hospitals said their shifts are often short five to 10 nurses, forcing nurses to take on more patients than they can handle.
Omodt said that while there was a rise in understaffing reports during the height of covid, conditions have improved, and nurses have made contradictory claims when it comes to staffing at their hospitals since then.
In the lead-up to the strike, Minnesota hospital groups filed unfair labor practices charges against the union for refusing to go to mediation, and asked the National Labor Relations Board to block the strike for a failure to provide enough notice. The NLRB has thrown out at least some of those charges.
Hospitals facing strikes have been recruiting traveling nurses from across the region and plan to maintain staffing levels during the strike, though they are preparing for reduced operations, according to some of the hospital groups facing strike activity.
For years, hospitals in the United States have faced understaffing problems. A surge in demand and increased safety risks for nurses during the pandemic accelerated those trends. The number of health-care workers in the United States has still not recovered to its pre-pandemic levels, down 37,000 workers compared with February 2020.
At the same time, demand for health-care services has steadily increased during the pandemic, with a backlog of people who delayed care now seeking medical attention. During the covid wave that swept across the United States this summer, states such as New York and Florida reported the worst nursing shortages in decades. Research shows that patients are more likely to die because of preventable reasons when health-care providers are overworked.
Nurses, who risked their lives during the pandemic, are quitting and retiring early in droves, because of increased workloads caused by short staffing and demanding schedules that make finding child care and having a life outside of work exceedingly difficult. The understaffing crisis is pronounced in Minnesota in part because of its aging population and its record low unemployment rate.
There are some signs that nurse- and other health-care-worker strikes could spill over to other states in the coming weeks. Four thousand nurses with the Michigan Nurses Association voted earlier this month to authorize a strike related to understaffing concerns, and 7,000 health-care workers in Oregon have also authorized a work stoppage. University of Wisconsin nurses narrowly averted a strike this week. Therapists and clinicians in Hawaii and California are currently in the fourth week of what has become the longest-running mental health care strike, over inadequate staffing levels.
In Minnesota, the Minnesota Nurses Association recorded a 300 percent increase in nurses’ reports of unsafe staffing levels on their shifts since 2014, up to 7,857 reports in 2021.
Kelley Anaas, 37, a nurse who works in the ICU at Abbott Northwestern in Minneapolis said nurses in her unit have been forced to double up on patient assignments and work with lead nurses who have less than a year of experience.
“It eats away at you. If that was my family member in that bed, I wouldn’t want to leave their side,” said Anaas, adding that her workload has increased steadily over her 14 years at Abbott Northwestern.
While the nurses say their main impetus for striking is staffing levels and not pay, they are also at odds with hospitals over wages. The Minnesota Nurses Association has proposed a 30 percent pay increase over the next three years, noting inflation is at a 40-year high, while health-care groups have proposed a pay increase of 10 to 12 percent.
“The union’s wage demands remain at 29 and 30 percent increases over three years, which we’ve told them is unrealistic and unaffordable,” Omodt said, noting that the average Minnesota nurse makes $80,960 a year.
Contracts expired in May and June, and the union has been in negotiations since March.
Nurses said they are frustrated the strike is happening, but the stakes are high for them and their patients.
“We’re really sad and disappointed that it has come to a strike,” said Brianna Hnath, a nurse at North Memorial in Robbinsdale. “But we feel like this is the only thing we can do to show administration how incredibly important a strong nursing core is to a hospital. Hospitals tell us it’s our fault, but we’ve been actively involved and getting nowhere.”
https://mailchi.mp/6a3812741768/the-weekly-gist-september-9-2022?e=d1e747d2d8

We’re fortunate to be privy to many of the big, complex strategic issues being discussed in health system boardrooms and executive meetings these days: care model innovations, new investments in technology, the digital revolution in care, market-shaping partnerships, the future of the healthcare workforce, and on and on. It’s a precarious and strategically critical moment for incumbent systems in many ways. But we’re often reminded that the nuts and bolts of running hospital facilities still demands attention, even at a board level.
Case in point: the perennial discussion about what otherwise seems like a minor issue—parking. You’d be shocked how often parking comes up in board-level discussions (partly because many board members are older, active users of hospital services, who spend significant time looking for a place to park). We’ve been witness to knock-down, drag-out arguments about whether to charge for parking, and why more parking isn’t available for patients, physicians, and others.
At first it seems like a trivial issue, but of course it isn’t. In reality, it’s a tangible example of how much patient experience matters in the design and operation of healthcare delivery. We’ve also found it’s a useful analogy in explaining to leaders why “frictionless access” should be at the heart of digital patient experience as well—a poorly-designed digital “front door” can be just as frustrating as not being able to find an inexpensive and convenient place to park before a medical appointment.
Delivering reliable, affordable, high-quality care is critical, but getting the small experiential details (like parking) right can be incredibly impactful. Next time you visit a medical facility, think about what the parking experience is telling you about how “patient-centered” your provider really is.
https://mailchi.mp/6a3812741768/the-weekly-gist-september-9-2022?e=d1e747d2d8
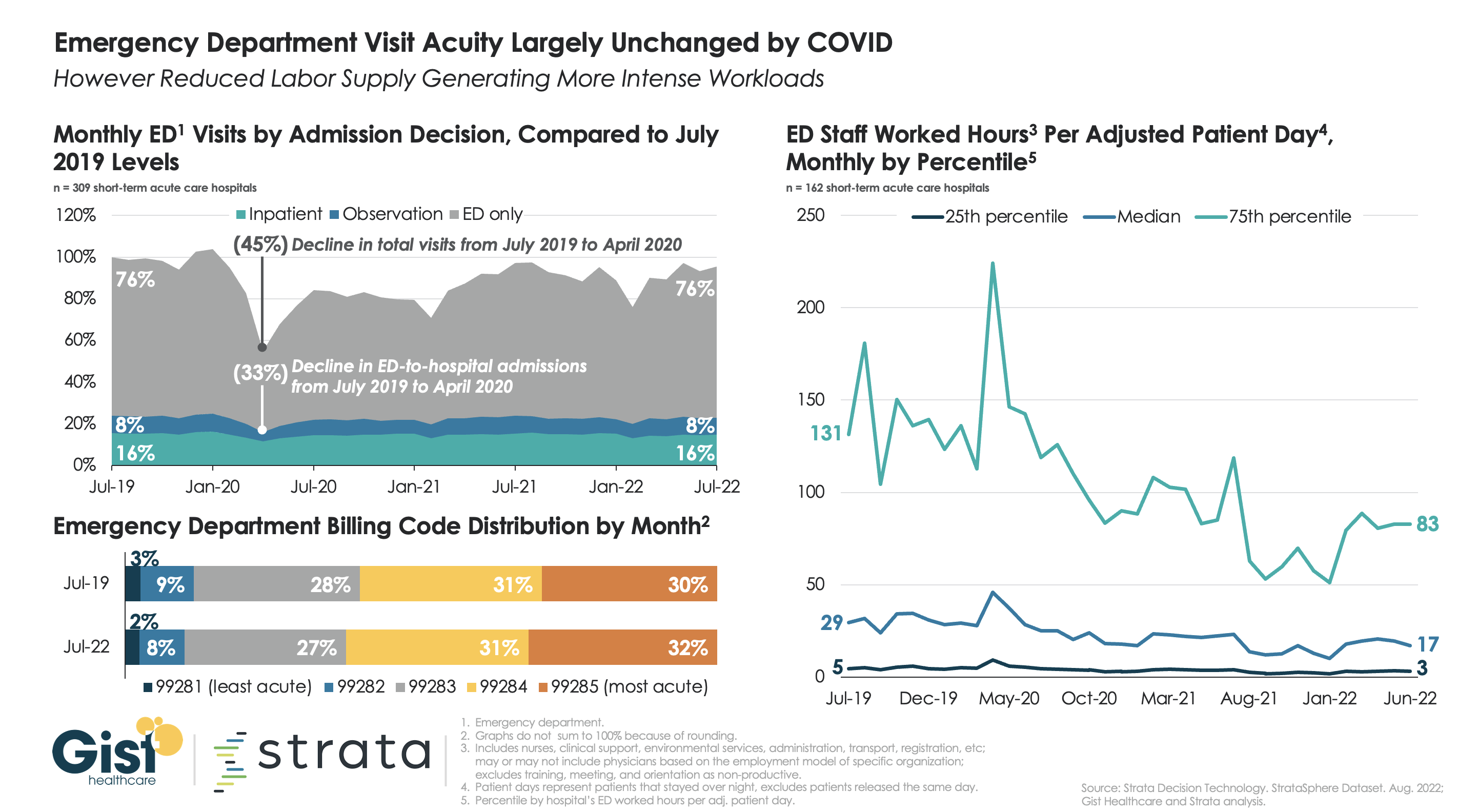
Many health systems are wondering if consumers are now leveraging new access points, including telemedicine, for low-acuity urgent care instead of going to the emergency department (ED), something which many experts are forecasting. For the graphic above, we partnered with healthcare software and analytics firm Strata Decision Technology to try to answer this question.
Using their national StrataSphere dataset for short-term acute care hospitals, we found that ED patient acuity levels in July 2022 were virtually identical to those in July 2019, though 2022 volumes were down by four percent. Admission and observation decisions across the two groups were also largely the same. We’ll be keeping our eye on the data to see if the story changes, as individuals who have delayed care over the last two and a half years now return, presenting to the ED with more advanced disease.
While current ED patients may not be more acute than before, the ongoing shortage of clinical labor may explain why some hospitals tell us that their EDs feel busier than ever. Measured by total worked hours of ED employees per adjusted patient day, the amount of labor dedicated to each patient requiring an overnight ED stay is down around forty percent from 2019 across hospital EDs of all staffing levels. With fewer labor hours to go around, each team member on the floor now has more to do.
https://mailchi.mp/6a3812741768/the-weekly-gist-september-9-2022?e=d1e747d2d8

A recent JAMA study of 578 US dermatology, gastroenterology, and ophthalmology practices acquired by PE firms from 2016 to 2020 found a steady rise in spending in the two years after acquisition, indicating that the average charge per commercial claim increased 20 percent, and the average allowed amount per claim rose 11 percent. It also found that, compared to a large control group with similar patient risk scores, PE-acquired practices saw new patient visits increase by 38 percent and total visit volume increase by 16 percent.
The Gist: While the study’s authors note that these findings could be explained by changes in practice operations or management, they point out they could also be caused by an overutilization of profitable services not tied to an increase in value or benefit to the patient.
We think the latter is likely the case here, and that this study provides evidence of PE-induced overutilization aimed at meeting aggressive growth targets.
But this is just the latest wave of ownership-induced overutilization: 20 years ago the same spotlight was on physician-owned imaging, cardiac, and other outpatient diagnostics, with several studies then documenting higher utilization in these facilities. Nonetheless, this latest trend is an important one to document and quantify, as the number of physicians working in PE-backed organizations continues to rise.
https://mailchi.mp/6a3812741768/the-weekly-gist-september-9-2022?e=d1e747d2d8

The same Texas federal judge who ruled the entire ACA unconstitutional in 2018—a decision overturned by the Supreme Court last year—ruled this week that the ACA cannot require a company to fully cover preventive HIV drugs for its employees, on the grounds that doing so violates owners’ religious freedom. He also asserted that the government’s system for deciding what preventive care services should be covered under the ACA is unconstitutional, a broader declaration that potentially jeopardizes a wide swath of no-cost preventive services enshrined in the ACA for millions of Americans, including screening tests for a variety of cancers, sexually transmitted infections, and diabetes. The ruling did not include an injunction and is likely to be appealed.
The Gist: Fully-covered preventive care services are a cornerstone of the ACA, and have increased access to basic healthcare services for many Americans. While there is still some uncertainty about the scope of this ruling, if it were to stand, millions of Americans would once again have to pay for some of the most common and highest-value healthcare services. That additional financial barrier, along with potential tightening of health plan benefit designs, would create barriers to access that only exacerbate our nation’s already stark healthcare disparities.
