Cartoon – Some Ethical Roadblocks
The sudden uncertainty surrounding the future of the Affordable Care Act could be an enormous political liability for Republicans in key states come November.
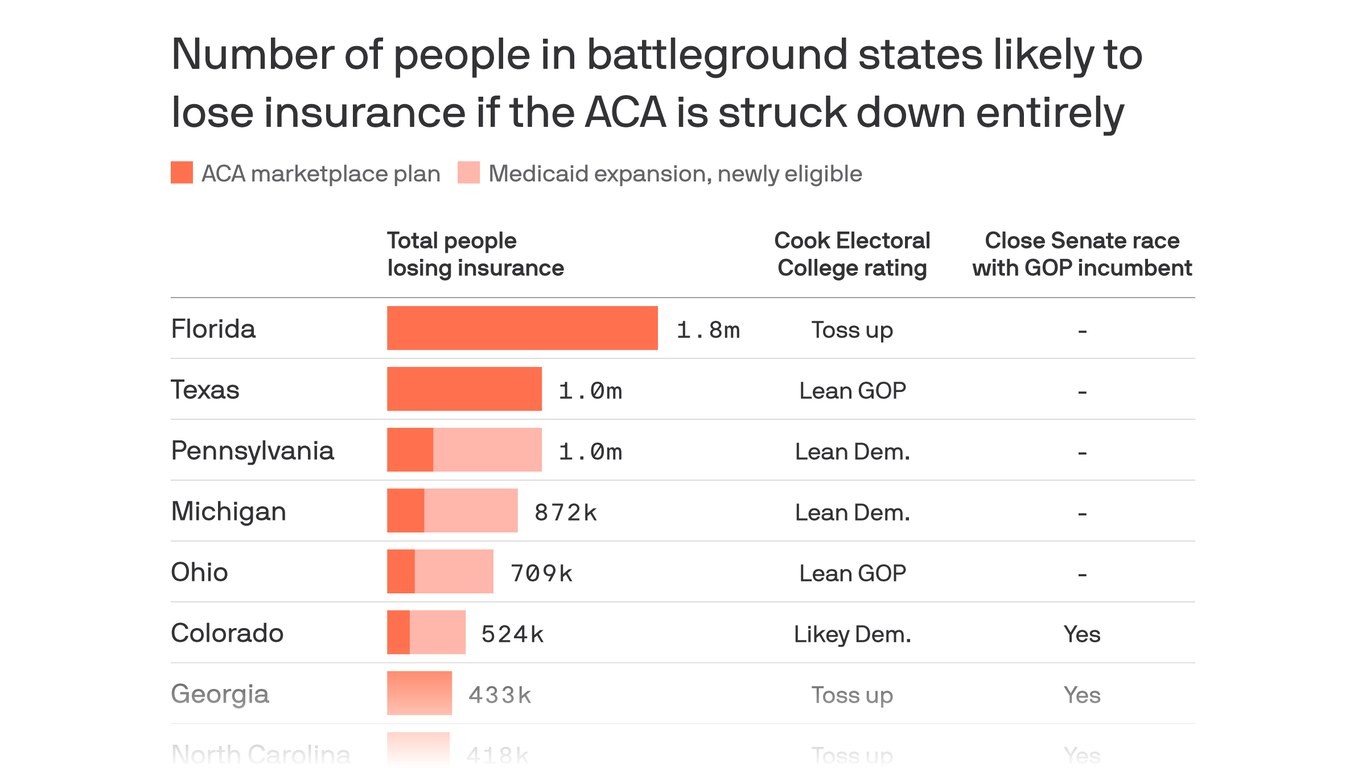
Between the lines: Millions of people in crucial presidential and Senate battlegrounds would lose their health care coverage if the Supreme Court strikes down the law, as the Trump administration is urging it to.
The chart above shows the number of people enrolled in the ACA’s insurance marketplaces or covered through its Medicaid expansion.
The big picture: Republicans paid a steep electoral price for trying to repeal parts of the ACA in 2017. Republicans’ lawsuit against the health care law, if it succeeds, would boot even more people off of their coverage and undo even more of the ACA’s regulations.
What to watch: Several vulnerable Republicans, including Sens. Susan Collins, Martha McSally, and Cory Gardner, represent purple states that expanded Medicaid and would therefore see steep coverage losses. And the broader fight over the Supreme Court has made it impossible to ignore those stakes.

The flag-draped casket of Justice Ruth Bader Ginsburg lies in repose under the Portico at the top of the front steps of the US Supreme Court. Ginsburg died at 87 on September 18 after serving on the high court for 27 years.
When news broke of Justice Ruth Bader Ginsburg’s death on September 18, the outpouring of grief and gratitude for the accomplishments of the feminist icon was quickly followed by speculation over how her passing will affect the legal challenge to the Affordable Care Act (ACA) now before the US Supreme Court.
The landmark health law survived high court rulings in 2012 and again in 2015. In each case, Chief Justice John Roberts voted with the court’s liberal bloc, including Ginsburg, to uphold the ACA. President Donald Trump has nominated conservative Judge Amy Coney Barrett of the Seventh Circuit of the US Court of Appeals to fill Ginsburg’s seat. Because oral arguments for California v. Texas are set for one week after Election Day, supporters of the law are uneasy.
“If the suit had a trivial chance of success yesterday, it has a new lease on life,” University of Michigan law professor Nicholas Bagley told Amy Goldstein in the Washington Post after learning of Ginsburg’s death. “The ACA has become part of the basic plumbing of the US health care system. Ripping it out at this point would create enormous problems.”
If the ACA is overturned, the consequences could be severe. At this point, the nation remains mired in the coronavirus pandemic, which has metastasized into one of the greatest public health crises in a century. Last week, the US reached the horrific milestones of more than 7 million people infected and 200,000 dead from COVID-19. ACA protections for people with preexisting conditions would disappear if the health law is struck down, and more than 12 million adults who have gained health coverage through the ACA’s Medicaid expansion could lose it. More than 9 million others would lose access to subsidized premiums for private health insurance.
Still, the worst-case scenario is just one of many. Here is a review of the lawsuit, what’s at stake, and the potential outcomes.
California v. Texas originated from a consortium of Republican state attorneys general led by Texas. A California-led coalition of 20 states and Washington, DC, is defending the ACA. The Texas coalition argues that the ACA is unconstitutional in its entirety because Congress in 2017 zeroed out one provision of the lengthy law, the individual mandate. If that part of the ACA is invalid, they argue, then the rest is too.
Many legal experts find this position unpersuasive. The arguments “have been roundly criticized by conservative legal scholars, the Wall Street Journal editorial board, the National Review editorial board, health care stakeholders, and some Republican members of Congress and state officials,” ACA expert Katie Keith, JD, MPH, wrote on the Health Affairs Blog. The Supreme Court is scheduled to hear oral arguments in the case on November 10, one week after the election.
Thanks to the 10-year-old ACA, millions of Americans have gained health coverage. This has proved to be essential during the global pandemic. But if the health law is struck down, about 21 million people who buy health insurance through the ACA exchanges or who gained coverage through Medicaid expansion would be at serious risk of becoming uninsured.
California enthusiastically leaned into the ACA from the start and saw the biggest decline in uninsured residents — 3.7 million — of any state. As the California uninsured rate fell, racial disparities in coverage were also reduced. By 2016, the ACA had produced historic declines in racial disparities in health coverage rates for Californians. (Learn more about the impact of the ACA in California with this collection of resources.)
Nationwide, nearly 133 million people with preexisting conditions could be denied coverage or be required to pay more for a health insurance policy if the ACA is eliminated. “Contracting the [coronavirus] is the ultimate preexisting condition,” Andy Slavitt, former administrator of the Centers for Medicare & Medicaid Services under President Barack Obama, and Bagley wrote in the New York Times. “The disease can bring with it mysterious complications and affect virtually every organ system, the immune system, and even the limbs. Young, otherwise healthy people may find themselves uninsurable if the Affordable Care Act is struck down.”
A lawsuit that once seemed like a long shot now has a much more reasonable chance at success — and that means 20 million people’s health coverage really could be in the balance.
—Sam Baker, Axios
Also at risk are essential health benefits that the ACA requires all health plans to cover, including maternity care, mental health services, and substance use disorder treatment. If the law is overturned, they could disappear from insurance plans.
“Other popular provisions hang in the balance, including those that guarantee preventive care with no out-of-pocket payments; end lifetime caps; allow kids to stay on their parents’ insurance through age 26; and make vaccines free to patients. Even some key improvements to Medicare — including a reduction in prescription drug costs for beneficiaries — would be gone,” Slavitt and Bagley wrote.
The ACA’s impacts reach far beyond health care consumers. “Insurance companies, drug companies, hospitals, and doctors have all changed the way they do business because of incentives and penalties in the health law,” Julie Rovner wrote in Kaiser Health News. “If it’s struck down, many of the ‘rules of the road’ would literally be wiped away, including billing and payment mechanisms.”
If the Republican Senate votes to confirm Barrett before the oral arguments for California v. Texas, the ACA faces a tougher battle, though it could be narrowly upheld. Although Barrett has not participated in any cases regarding the ACA on the Seventh Circuit, “her academic writing and public action offer glimpses into her views” opposing the health law, Goldstein and Alice Crites reported in the Washington Post.
If Barrett misses the oral arguments, she will not participate in the case. The Supreme Court could choose to postpone the arguments or proceed with eight justices, which is “far from unprecedented,” Keith wrote. Should that result in a 4-4 ruling, the lower court’s decision would stand, and the case would be remanded to a federal district court judge to decide which other provisions of the law must fall along with the individual mandate. Other provisions on the chopping block “could include the law’s rules banning insurers from denying people coverage or charging them higher premiums because of their medical history,” Dylan Scott wrote in Vox. Litigation could continue for years, during which the ACA would remain the law of the land, according to Keith.
This is not an exhaustive list of potential outcomes. For example, an eight-judge court could narrowly rule in favor of the ACA.
As Sam Baker wrote in Axios, “A lawsuit that once seemed like a long shot now has a much more reasonable chance at success — and that means 20 million people’s health coverage really could be in the balance.”

39 health systems in 45 states and Washington, DC have committed to addressing racism and the public health disparities caused by racism. Read the full statement below or download the PDF.
As members and leaders of many healthcare organizations across the nation addressing the disproportionate Black and Brown mortality of the COVID-19 pandemic, we say without hesitation that Black Lives Matter.
No person of decency can look at the images of George Floyd’s killing without feelings of rage, horror, shame, and grief. The deaths of George Floyd, Rayshard Brooks, Ahmaud Arbery, Breonna Taylor — and too many others — are unjust and unconscionable.
We must double down on our efforts. Systemic racism poses a real threat to the health of our patients, families, and communities. We stand with all of those who have raised their voices to capture the attention of people across the nation with a clear call for action.
The health systems we represent are deeply woven into the fabric of the communities we serve, live, and work in, and we stand united as frontline organizations against racism, injustice, and inaction.
Systemic racism results in generational trauma and poverty, while also unquestionably causing higher rates of illness and death in Black and Indigenous communities and communities of color. We have seen — in its rawest form — how the trauma of systemic racism adds to the historical injustices that have disproportionately affected communities of color. Health systems across the nation work to provide high-quality, compassionate care in the face of health disparities and poor outcomes resulting from social and economic inequities. In rural areas, where resources are spread out across larger geographies, we have seen healthcare organizations and community partners adapt to the shifting conditions with ingenuity and purpose.
These social determinants of health include poverty, inadequate housing, underperforming schools, police brutality, mass incarceration, food deserts, joblessness and underemployment, poor access to healthcare, and violence. All of these factors contribute to health inequities in our communities. And they serve as a recipe for pain, suffering, premature mortality — and civil unrest.
In our communities, there is also resilience, innovation, a tradition of faith, and a spirit of unity that manages to thrive even under the weight of this systemic burden. Imagine the potential for our communities with dramatically improved social and economic conditions and health outcomes.
It’s time to fully realize this potential. It’s time for action. We will work more intentionally with community-based partners in building and sustaining the sweeping change that is needed to ensure health equity across the country, and particularly in our most under-resourced communities.
As healthcare organizations, we are committed to being part of the solution, both within our organizations and in partnership with local community groups. We are focused on improving access to care and eliminating systemic racism, which contributes to poor health outcomes.
We have come together as health systems from all across the country as part of the Healthcare Anchor Network, a health system-led collaboration working to improve community health and well-being by leveraging all our assets, including hiring, purchasing, and investment for equitable, local economic impact. Here are some of the steps we are or will be taking to help overcome the healthcare disparities in the communities we serve:
We also are committed to continue working to address racism and the healthcare disparities it creates.
We commit to …
Our society only truly thrives when everyone has an opportunity to succeed and live a healthy life. We are committed to moving forward together. By harnessing the collective strengths of our organizations, we will help serve our communities as agents of change.
The healthcare systems that have signed onto this statement are: Advocate Aurora Health, Alameda Health System, AMITA Health, Baystate Health, BJC HealthCare, Bon Secours Mercy Health, Boston Children’s Hospital, Boston Medical Center, Children’s Hospital of Philadelphia, ChristianaCare, Cleveland Clinic, CommonSpirit Health, Cone Health, Dartmouth-Hitchcock Health, Denver Health, Einstein Healthcare Network, Franciscan Missionaries Of Our Lady Health System, Gundersen Health System, Kaiser Permanente, Lurie Children’s, M Health Fairview, Maimonides Medical Center, Mass General Brigham, Northwell Health, ProMedica, Providence St. Joseph Health, Rush University Medical Center, RWJBarnabas Health, San Mateo County Health, Seattle Children’s, Spectrum Health, The MetroHealth System, Trinity Health, UC San Francisco, UMass Memorial Health, University Hospitals, University of Utah Health, VCU Health, and Yale New Haven Health.
President Donald Trump and former Vice President and Democratic presidential nominee Joe Biden sparred over the future of the ACA, the COVID-19 pandemic and health insurance during a 90-minute debate in Cleveland Sept. 29.
Seven takeaways for healthcare leaders:
The ACA
1. Moderator and Fox News host Chris Wallace opened the debate with the topic of President Trump’s nomination of Judge Amy Coney Barrett of the U.S. Court of Appeals for the 7th Circuit to the U.S. Supreme Court. In the first few minutes of the debate, the discussion turned to the future of the ACA should Ms. Coney Barrett join the Supreme Court. A week after the November presidential election, the Supreme Court is set to hear a lawsuit, supported by the Trump administration, that seeks to overturn the ACA.
2. If the Supreme Court overturns the ACA, Mr. Biden said 22 million Americans would lose insurance and 100 million would lose protections for preexisting conditions. HHS said in 2017 as many as 133 million Americans have preexisting conditions, and a KFF analysis estimates 54 million Americans have conditions serious enough to lead to coverage denials if the ACA is overturned.
3. Mr. Wallace questioned the president about his promise to repeal and replace the ACA, adding that President Trump hadn’t released a comprehensive plan to replace the health law despite pledges to do so. The president disagreed with that, saying he had gotten rid of the individual mandate. Mr. Wallace said eliminating the mandate was not a comprehensive plan. Mr. Wallace called President Trump’s recent executive orders on preexisting conditions and surprise billing “largely symbolic.” President Trump disagreed, but did not tell how the executive orders would be implemented.
Drug prices
4. The president said drug prices would be coming down “80 or 90 percent.” The president highlighted insulin, which he said he’s getting so inexpensively, “it’s like water.” Insulin continues to retail for about $300 per vial, according to STAT, but cheaper insulin prices could be coming for some seniors. CMS recently said it is expanding the number of Medicare Advantage plans that provide insulin for a $35 or less monthly copay.
Public option
5. In an exchange with Mr. Biden, President Trump accused the Democratic Party of wanting “socialist medicine,” and claimed Mr. Biden wants to end private insurance. Mr. Biden denied those claims and said his health plan, which includes expanded ACA subsidies and a public option, would allow employees to keep their private health insurance. He has not supported Medicare-for-All proposals.
COVID-19
6. On the topic of the pandemic, Mr. Wallace asked President Trump about differing timelines for a vaccine that have been presented by him versus federal scientists like CDC Director Robert Redfield, MD. The president said he has spoken with Pfizer, Moderna and Johnson & Johnson, who’ve said “they can go faster” on a vaccine, but “it’s a very political thing.” He added that the military is already set up to distribute vaccines. Mr. Biden questioned Americans’ trust in the process. A Sept. 29 poll from the Axios/Ipsos Coronavirus Index found 8 in 10 Americans wouldn’t likely get a first generation COVID-19 vaccine if the president said it was safe.
7. President Trump and Mr. Biden took different stances on masks. Mr. Biden cited Dr. Redfield’s renewed call to wear masks, and said masking up and social distancing would save 100,000 lives between now and January. President Trump responded by saying, “They’ve said the opposite.” He alluded to early in the pandemic when public health experts, including Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, were slow to recommend widespread mask-wearing before scientists better understood how the virus spreads. The CDC currently recommends that every American wear a mask.
https://www.webmd.com/lung/news/20200925/us-still-in-first-wave-of-covid-19-fauci-says

Anthony Fauci, MD, says talk about a second wave of the coronavirus is premature because the United States is still dealing with the first one.
The idea of a second wave is based on the 1918 flu pandemic, when many cases were seen in the spring, he says. The spring cases “literally disappeared” and were followed by a spike in flu cases in the fall, he told CNN’s Sanjay Gupta, MD, on Thursday in an online conversation organized by Emory University.
“Rather than say, ‘A second wave,’ why don’t we say, ‘Are we prepared for the challenge of the fall and the winter?’” said Fauci, director of the National Institute of Allergy and Infectious Diseases and a member of the White House coronavirus task force.
Flu shots are an important measure to help the U.S. get through the winter, he said.
He and other health care professionals have observed that the Southern Hemisphere has had a very light flu season, probably because measures to curb the coronavirus, such as social distancing and mask-wearing, have limited the spread of the flu.
“If we listen to the public health measures, not only would we diminish the effect of COVID-19, we might get away with a very, very light flu season if we combine that with getting the flu vaccine,” Fauci said.
In a separate interview, he said the arrival of the coronavirus vaccine will not stop the need for tried-and-true measures such as mask-wearing, hand-washing, and social distancing.
In a Facebook Live conversation with New Jersey Gov. Phil Murphy, Fauci said the coronavirus vaccine will not be 100% effective and won’t be taken by the entire population. That means the virus could still spread.
“So when a vaccine comes, we look at it as an important tool to supplement the public health measures that we do,” he said. “It will allow us to more quickly and with less stringency get back to some degree of normal. But it is not going to eliminate the need to be prudent and careful with our public health measures.”
Fauci said that vaccinating 75% to 80% of the population “would be a really good accomplishment.” He expects 700 million doses to be produced by the end of this year or early 2021.
President Trump presented his “America First Healthcare Plan” during a speech to healthcare professionals in Charlotte, North Carolina, on Thursday — a plan that mentioned preexisting condition coverage protections and surprise billing but did not seem to include comprehensive changes to the healthcare system.
“Under the America First Healthcare Plan, we will ensure the highest standard of care anywhere in the world, cutting-edge treatments, state-of-the-art medicine, groundbreaking cures, and true health security for you and your loved ones,” Trump said. “And we will do it rapidly, and it’s in very good order, and some of it has already been implemented.”
Executive Order Provisions
The president signed an executive order outlining the plan, but the order contained initiatives in only a few areas, including:
Trump also announced another initiative, this one aimed at seniors. “Under my plan, 33 million Medicare beneficiaries will soon receive a card in the mail containing $200 that they can use to help pay for prescription drugs … The cards will be mailed out in coming weeks,” Trump said. The $6.6 billion cost of the cards will be paid for under the auspices of a Medicare demonstration program. These funds are ostensibly available via savings generated through Trump’s “most favored nation” executive order allowing Medicare to pay no more for certain prescription drugs than the price paid by other developed countries, a White House official said. That executive order has not yet been implemented, however, and court challenges are expected.
Final Rule Issued on Drug Importation
Trump also noted that the FDA issued a final rule on Thursday implementing the president’s July executive order earlier this month to allow for importation of certain less expensive prescription drugs from Canada. “This means a state or whatever — can go to Canada and buy drugs for a fraction of the price that they’re charging right now,” he said.
He also highlighted individual actions his administration had taken that mostly affected particular groups, including lowering insulin prices for certain Medicare beneficiaries, investing in childhood cancer research, and expanding health reimbursement accounts that employers can use to reimburse employees for medical expenses. The COVID-19 pandemic received scant mention other than a reference to slashing red tape to accelerate development of treatments for the disease, and a sentence about how the pandemic had greatly increased the use of telehealth.
During a telephone briefing with reporters Thursday afternoon, HHS Secretary Alex Azar highlighted the surprise billing provision. “The President is saying that all the relevant players — hospitals, doctors, insurance companies — had better get their act together and get legislation passed through Congress that protects patients against surprise medical bills from anybody — hospitals or doctors, doesn’t matter,” he said.
“Those special interest groups need to sort it out and figure out how that would work,” he continued. “There have been legislative packages that have come quite close on the Hill that are bipartisan, but…. the president is saying the time is now. And if they do not get legislation passed by January 1st, he is instructing me to use the full regulatory power of the U.S. government to protect patients against surprise medical bills.”
Sen. Lamar Alexander (R-Tenn.), outgoing chairman of the Senate Health, Education, Labor, & Pensions (HELP) Committee, praised the surprise billing announcement. “The president is right to call on Congress to pass legislation this year to end surprise medical billing,” Alexander said in a statement, adding that a bill currently going through the House and Senate addresses the issue effectively. “Ending surprise medical bills is a problem that requires a permanent solution passed by Congress this year. The American people can’t afford to wait any longer.”
Preexisting Condition Provision Panned
The preexisting condition provision drew scorn from Democratic legislators. The provision “offers no protection not already available through the existing Affordable Care Act (ACA) and no protection for millions of Americans with preexisting conditions if Trump is successful in packing the Supreme Court to destroy the ACA,” Rep. Lloyd Doggett (D-Texas), chairman of the House Ways & Means Health Subcommittee, said in a statement.
But Azar said during the briefing that the ACA’s clause requiring insurers to cover preexisting conditions does no good if people aren’t able to afford insurance in the first place. “If you’re a couple, aged 55, living in Missouri, making $70,000 a year, Obamacare is going to cost you $30,000 in premiums and a $12,000 deductible,” he said.
Azar promised that the administration “will work with Congress or otherwise to ensure” that people with pre-existing conditions are protected, but he did not indicate how that would be made affordable to individuals without government subsidies of the sort Republicans have long opposed.
Bob Laszewski, president of Health Policy and Strategy Associates in Alexandria, Virginia, questioned how much good the executive order’s preexisting condition provision would do. “Trump and the Republicans couldn’t pass an alternative to Obamacare in 2017 when they controlled the White House and both houses of Congress,” he wrote in a blog post. “But, now he can just sign an executive order and everything is fixed? He has signed a number of healthcare-related executive orders and just about all of them are tied up in the byzantine federal regulatory process, or have faded away. This is just an election-year gimmick in an attempt to persuade voters that Trump has healthcare policy under control. There are a lot of governments in the world that operate by executive fiat. Ours is not one of them.”