US Supreme Court Agrees to Review Affordable Care Act — for the Third Time

The fate of the Affordable Care Act (ACA) is once again in the hands of the US Supreme Court. On March 2, the court announced that it would hear a case challenging the health law, a wide-ranging measure that “touches the lives of most Americans, from nursing mothers to people eating at chain restaurants,” wrote Reed Abelson, Abby Goodnough, and Robert Pear in the New York Times. This will be the third time the court will rule on the ACA since President Barack Obama signed it on March 23, 2010.
“The justices will review a federal appeals court decision that found part of the law . . . unconstitutional and raised questions about whether the law in its entirety must fall,” reported Robert Barnes in the Washington Post. He noted that it is one of the first cases accepted for the Supreme Court term beginning October 5, which means a decision is not likely until spring or summer of 2021.
Should the court overturn the ACA, many Americans would lose the benefits afforded under the law. As Dylan Scott wrote in Vox, “everything would go: protections for preexisting conditions, subsidies that help people purchase insurance, the Medicaid expansion.”
Let’s break down each of those categories.
Protections for Preexisting Conditions
Before the ACA, people with preexisting conditions, which included common medical conditions like asthma, diabetes, and cancer, were denied health insurance or charged higher insurance premiums. Important benefits like maternity care and mental health services frequently were carved out of the benefit packages in health plans sold in the individual market — that is, outside of employer-sponsored coverage. An issue brief (PDF) by the Department of Health and Human Services estimated that up to 133 million nonelderly Americans have a preexisting condition.
As Andy Slavitt, the former administrator of the Centers for Medicare & Medicaid Services under President Obama, wrote on Twitter, examples of being charged more included “$4,270 more for asthma, $17,060 for pregnancy, and $160,510 for metastatic cancer.”
Under the ACA, insurers are no longer allowed to deny coverage or charge higher prices to people with preexisting conditions. But if the Supreme Court rules against the ACA, these protections would vanish.
Medicaid Expansion
A key provision of the ACA is expanded eligibility for enrollment in Medicaid, a federally funded state option adopted so far by 36 states and the District of Columbia. More than 12 million adults with low incomes have gained Medicaid coverage through this provision, and research comparing expansion and nonexpansion states has linked expanded Medicaid access to better health outcomes.
According to the Urban Institute, if the ACA is repealed, “the uninsurance rate across all expansion states would increase from 9% of the nonelderly under current law to 17% under repeal. In nonexpansion states, the uninsurance rate would increase from 15% of the nonelderly to 21%.” Many of the newly uninsured would be the result of losing the Medicaid coverage the ACA provided.
“The uninsured rate for Black Americans would increase from 11% to 20% without Obamacare,” Scott reported. “There would also be a dramatic spike in uninsurance among Hispanics.”
Subsidies to Help People Purchase Insurance
To expand access to affordable health insurance for those who can’t get it through their jobs, the ACA offers federal subsidies to people with low and moderate incomes who buy insurance through the ACA insurance exchanges. The subsidies take the form of premium tax credits and cost-sharing subsidies.
Approximately 9.2 million Americans receive federal subsidies, reported Abelson, Goodnough, and Pear. “On average, the subsidies covered $525 of a $612 monthly premium for customers in the 39 states that use the federal marketplace,” they wrote.
If the ACA is overturned and the subsidies are eliminated, the cost of health insurance would become unaffordable for many of those 9.2 million people, and the uninsured population would soar.
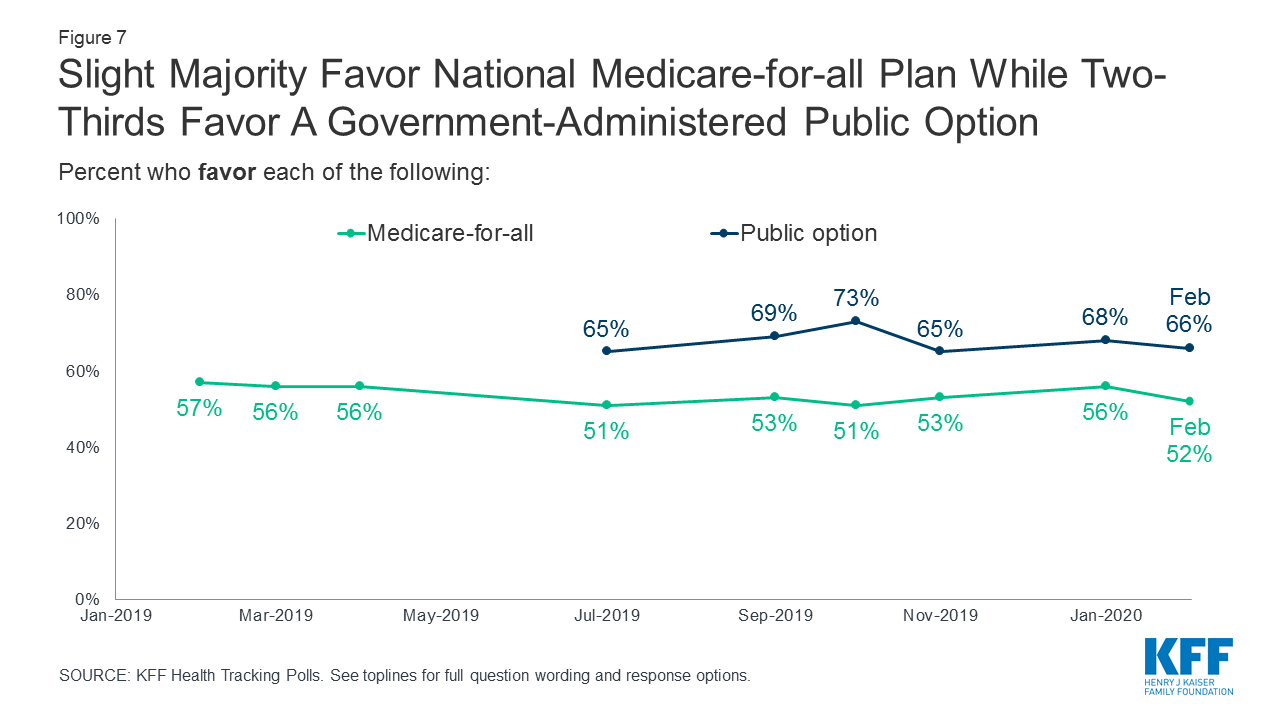
Polls Show Public Support for the ACA
According to the February 2020 KFF Health Tracking Poll, 55% of Americans say they now favor the ACA, a new high compared to approval ratings below 40% as recently as 2016. Today 85% of Democrats express favorable views of the law, compared to 53% of independents and 18% of Republicans.
Though overall support for the health law remains partisan, many of its provisions have broad bipartisan support, KFF staff wrote in Health Affairs. For instance, large majorities of Democrats (94%), independents (88%), and Republicans (77%) have a favorable view of the ACA’s health insurance exchanges, and most Democrats (80%), independents (71%), and Republicans (54%) view the Medicaid expansion favorably.
Rising Health Costs Worsen California’s Coronavirus Threat
The global spread of the novel coronavirus disease known as COVID-19 puts threats to the ACA into perspective. Despite the coverage gains made under the ACA, nearly 28 million Americans remain uninsured, and that number would rise if the law were overturned. As Chris Sloan, associate principal at the consulting firm Avalere Health, told Caitlin Owens in Axios, we “could see uninsured or underinsured patients . . . skipping necessary treatment because they believe they can’t afford it.”
“Some lawmakers are concerned that the tens of millions who are underinsured — Americans with high deductibles or limited insurance — may also be at risk of unexpected expenses as more and more people are exposed to the virus,” Reed Abelson and Sarah Kliff reported in the New York Times.
Kristof Stremikis, director of CHCF’s market analysis and insight team, wrote in a recent blog post, “In an era when the average deductible facing a working family in California now exceeds $2,700, it’s not hard to imagine how many people missed detection and treatment opportunities because they could not afford to pay for them.”
To address some of these concerns, the California Department of Insurance (PDF) and the Department of Managed Health Care (PDF) directed all commercial health plans and Medi-Cal plans to “immediately reduce cost-sharing (including, but not limited to, co-pays, deductibles, or co-insurance) to zero for all medically necessary screening and testing for COVID-19, including hospital, emergency department, urgent care, and provider office visits where the purpose of the visit is to be screened and/or tested for COVID-19.”
Similar policies have been announced by state regulators in Washington and New York, the San Francisco Chronicle reported.












{kind=link}