The White House is taking a new position on the coronavirus pandemic: a daily count of 750 deaths is a testament to the federal government’s successful pandemic response.
On Wednesday, when U.S. health officials reported nearly 27,000 new Covid-19 cases, President Trump said in a television interview that the virus was “dying out.” He brushed off concerns about an upcoming rally in Tulsa, Okla., because the number of cases there is “very miniscule,” despite the state’s surging infection rate. In a Wall Street Journal interview Wednesday, Trump argued coronavirus testing was “overrated” because it reveals large numbers of new Covid-19 cases, which in turn “makes us look bad,” and suggested that some Americans who wear masks do so not only to guard against the virus, but perhaps to display their anti-Trump animus.
But a range of public health experts told STAT that this messaging not only diverts attention from a pandemic that has already caused 120,000 U.S. deaths, but has more practical implications: It could make it difficult for local governments to enlist the public in the mitigation measures necessary to reduce the continued spread of the virus.
“The science behind how people process public warnings in a crisis supports this: You have to have people speaking with one voice,” said Monica Schoch-Spana, a medical anthropologist at the Johns Hopkins Center for Health Security. “You need a chorus.”
Conflicting directives can make it more difficult for recommendations coming from state and local leaders to have an impact, said Sara Bleich, a professor of public health policy at Harvard’s T.H. Chan School of Public Health.
“It sends a mixed message, which is confusing, particularly because while many people will get infected, most will not get severely sick, so it’s easy to say this won’t happen to me,” she said. “And it’s that sort of attitude that will keep us in this situation for a very long time.”
While the president has for weeks, if not months, underplayed the pandemic, his sharp and repeated remarks this week represent a remarkable attempt from the leader of American government to effectively declare the U.S. Covid-19 epidemic over.
The president’s rhetoric comes at a time that his coronavirus task force, which once conducted daily briefings, has not addressed the public since May. The president’s resumption of campaign rallies flouts federal guidance that encourages mask use (Trump’s campaign will hand out masks and hand sanitizer at the rally, but has not said it will require attendees to use them) and discourages large indoor gatherings. And the president has repeatedly claimed, misleadingly, that persistently high U.S. case totals are simply the result of increased testing.
Health experts say that political leaders preaching caution and modeling proper behavior — such as wearing a mask and demonstrating proper hand hygiene — can send a powerful signal to people that these steps can not only protect them, but their communities. They say that, essentially, national and state leaders need to walk the walk in a situation when individual behavior, like staying home when sick and cooperating with contact tracing, can make a large impact in curbing contagion.
Trump’s counterproductive behavior, Schoch-Spana said, extends far beyond the consistently dismissive tone he has taken toward the health risks of Covid-19. With few exceptions, the president has refused to wear a mask in public, and has insisted on continuing in-person briefings and White House events that effectively defy federal health guidance about gathering indoors in large groups.
“It’s not just words, it’s actions,” she said. “So when you have the nation’s top executive refusing to wear a mask, holding meetings where people are shoulder to shoulder, where he’s signing executive orders — that is also a form of communication.”
Experts also say continued federal commitments to combating the virus are crucial as the public grows tired of abatement measures. Instead, Trump has only elevated his monthslong campaign of downplaying the virus.
And Vice President Mike Pence, in a Wall Street Journal op-ed, framed the declines in cases and deaths since April as “testament to the leadership of President Trump” — even as hundreds of Americans are still dying every day and cases are not dropping further.
Rep. Donna Shalala (D-Fla.), who served as health secretary during the Clinton administration, said she hoped Americans would listen to public health guidance from local officials, not Trump and Pence.
“The president of the United States is dangerous to the health of the people of my district, because he’s giving out misinformation and false hope,” she said. “For those that believe him, they’re putting themselves and their families at risk.”
Public health experts have raised a number of issues with the administration’s messaging.
For one, a plateau of cases and deaths should not be celebrated, they say. While some countries in Europe and Asia have not only flattened their curve but driven them down, that hasn’t happened in the United States. Daily cases and deaths dipped from the peak in April, but have averaged about 20,000 and 800, respectively, for weeks.
Beyond those numbers representing real people getting sick and dying, there are other problems with sustained high levels of spread. The more cases there are, the more difficult it is for the surveillance system, including contact tracing, to keep up. It’s also more likely that some of the cases will spiral into explosive spread; 20,000 cases can turn into 40,000 a lot faster than one case can turn into 20,000.
Plus, a failure to suppress spread now could lead to more prolonged disruptions to daily life. If transmission rates come fall are still what they are now in certain communities, that makes it harder to reopen schools, for example.
Experts also point to evidence suggesting that the daily case and death numbers won’t stay flat for long. While new cases in the Northeast and Midwest are declining, a number of states in the West and South — Arizona, Texas, Florida, California, and Oregon among them — have reported record number of new cases this week. What worries public health officials is that, without measures to stem those increases, those outbreaks could keep growing. Those thousands of new cases also signal that, in a week or two, some portion of those people will show up in the hospital, and, about a week after that, a number of them will be dead, even as clinicians have learned more about treating severe Covid-19.
Some states in the South and West are already reporting record hospitalizations from Covid-19.
The White House’s shrug has been echoed by some governors, who insist, like Pence and Trump, that increased testing explains away the rise in cases. That is certainly one reason; testing has become more widespread, so states are capturing a more accurate reading of their true case burden.
But experts say increased testing can only account for some of the data states are reporting. Other metrics — including rising hospitalizations, filling ICUs, and the increasing rate of tests that are positive for the virus — signal broader spread.
Until Wednesday, leaders of Texas and Arizonaalso bristled at efforts from city and county officials to institute mask requirements, but acceded to growing pressure even as they have not ordered statewide mandates.
Cameron Wolfe, an infectious disease expert at Duke University, said he was seeing a growing “fatigue” among the public to keep up with precautionary steps like physical distancing and mask wearing. People letting down their guard was coinciding with an increase of cases in states, including North Carolina.
He said medical experts and health workers needed to model proper behavior to show others that the coronavirus epidemic was still something that required action. But, he added, “that also comes from political leaders buying into this.”
Federal and state authorities, he said, need to be “taking this to heart. That has not yet happened. That needs to change if we’re going to get people to buy into this.”
Some state and local leaders are softening their resistance to issuing public masking requirements as emerging research shows face coverings can slow the spread of COVID-19, even as others are doubling down on their opposition.
The debate over whether to require face coverings in public has become increasingly politicized in recent weeks, even as COVID-19 cases have increased in the Sun Belt and some other parts of the country as lockdowns across the country have greatly eased.
Governors in southern, conservative states have been reluctant to issue statewide mandates on public mask-wearing, and in some cases have prevented local governments from taking stronger actions.
“We want to make sure that individual liberty is not infringed upon by government and hence government cannot require individuals to wear a mask,” Texas Gov. Greg Abbott (R) said Wednesday in an interview with Waco television station KWTX.
Abbott, who frequently recommends mask-wearing, has resisted calls from local leaders to require it, and has also prohibited them from enforcing local orders with civil or criminal penalties on individuals.
However, two Texas counties on Wednesday announced businesses must impose a mask rule on staff and customers or face fines of up to $1,000, which Abbott said would be allowed under his executive order.
“Businesses … they’ve always had the opportunity and the ability, just like they can require people to wear shoes and shirts, these businesses can require people to wear face masks if they come into their businesses. Now local officials are just now realizing that that was authorized,” he said.
Texas has experienced a rapid increase in COVID-19 cases that experts say is likely related to the state’s decision to lift lockdown measures ahead of Memorial Day. The state reported 3,129 new COVID-19 cases Wednesday, its largest single-day increase. Nearly 2,800 people were hospitalized with COVID-19 as of Wednesday, a new high for the state.
In Arizona, which has also seen a surge in cases, Gov. Doug Ducey (R) on Wednesday again resisted calls to issue a statewide masking requirement, but in a reversal, said he would allow local governments to take their own actions. Larger cities including Phoenix and Tucson plan to do so.
“Every Arizonan should wear a face mask,” he said at a Wednesday press conference. “This is an issue of personal responsibility, and we’re asking Arizonans to make responsible decisions to protect the most vulnerable in our communities.”
While a number of coastal states and cities led by Democrats have strict mask requirements when in public settings such as grocery stores, where staying six feet away from others may not be possible, some Republicans appear to see it as a restriction on freedom and have emphasized individual responsibility.
Trump has almost exclusively declined to wear a mask, and has criticized his political rival Joe Biden, the Democratic candidate for president, for wearing one.
“I see Biden. It’s like his whole face is covered,” Trump said in an interview published Thursday in The Wall Street Journal. “It’s like he put a knapsack over his face. He probably likes it that way. He feels good that way because he does. He seems to feel good in a mask, you know, feels better than he does without the mask, which is a strange situation.”
The debate of whether to wear masks has sparked division on Capitol Hill, where two Republicans this week refused to follow a new directive from House Speaker Nancy Pelosi (D-Calif.)
“I consider masks much more effective at spreading panic and much less effective at stopping a virus,” said Rep. Tom McClintock (R-Calif.), during a hearing yesterday. He later put on a mask.
Polls have shown Democrats are more likely to wear masks in public than Republicans; a Gallup poll conducted in April found 75 percent of Democrats have worn a mask in public, compared to half of Republicans.
However, emerging evidence shows face coverings can slow the transmission of COVID-19. A study published in Health Affairs this week found that mandated use of face masks in public was associated with a reduction in the daily COVID-19 growth rate in 15 states and Washington, D.C., compared to states that did not have such requirements.
Governors of other states experiencing outbreaks, including Henry McMaster (R) of South Carolina, have recommended but don’t require people to wear face masks in public. City council members in Columbia, S.C., however, are reportedly considering a requirement for the state’s largest city.
Alabama Gov. Kay Ivey (R) hasn’t issued a statewide mask requirement for the public, but employees of certain businesses are required to wear them while working.
In Montgomery, Ala., which has the largest COVID-19 outbreak in the state, Mayor Steven Reed (D) issued an executive order Wednesday requiring face coverings be worn in public after a similar ordinance failed to pass the city’s council.
Florida Gov. Ron DeSantis (R) has also resisted a statewide mask requirement, though localities can require their use in public. On Tuesday, he encouraged people to wear masks when social distancing isn’t possible but said it would not be a requirement.
“In terms of forcing that under penalty of criminal law, we’re not going to be doing that. I think it would be applied unevenly and I just don’t think it would end up working,” DeSantis said at a press conference.
The state is also seeing an increase in cases, which DeSantis ties to increased testing. However, public health experts note that the percentage of tests coming back positive is also increasing, a sign of ongoing community transmission.
In Nebraska, where the rate of COVID-19 transmission has been declining, Gov. Pete Ricketts (R) encourages the use of masks in public but has threatened to withhold federal relief funding from localities that require their use in government buildings.
“The governor encourages people to wear a mask but does not believe that failure to wear a mask should be the basis for denying taxpayers’ services,” spokesman Taylor Gage told the Omaha World-Herald.
Not all Republican governors have resisted masking mandates. Maryland Gov. Larry Hogan and Massachusetts Gov. Charlie Baker were early to issue wide-ranging mask requirements in their states.
Meanwhile, Democratic governors are mandating mask requirements or say they are seriously considering it.
As cases continue to climb in North Carolina, Gov. Roy Cooper (D) said this state leaders are considering making mask-wearing in public settings mandatory but has not done so yet.
Oregon Gov. Kate Brown (D) announced Wednesday that people living in seven of the state’s counties will have to wear masks in public beginning June 24 as the state sees an increase in cases.
Democratic governors of states hit hard early in the pandemic including New York, Washington and New Jersey have required the use of face coverings in public for several weeks.
California Gov. Gavin Newsom (D) issued a statewide mask order Thursday amid an increase in COVID-19 cases in his state.
“Science shows that face coverings and masks work,” Newsom said Thursday. “They are critical to keeping those who are around you safe, keeping businesses open and restarting our economy.”
As coronavirus cases surge in states across the South and West of the United States, health experts in countries with falling case numbers are watching with a growing sense of alarm and disbelief, with many wondering why virus-stricken U.S. states continue to reopen and why the advice of scientists is often ignored.
“It really does feel like the U.S. has given up,” said Siouxsie Wiles, an infectious-diseases specialist at the University of Auckland in New Zealand — a country that has confirmed only three new cases over the last three weeks and where citizens have now largely returned to their pre-coronavirus routines.
“I can’t imagine what it must be like having to go to work knowing it’s unsafe,” Wiles said of the U.S.-wide economic reopening. “It’s hard to see how this ends. There are just going to be more and more people infected, and more and more deaths. It’s heartbreaking.”
China’s actions over the past week stand in stark contrast to those of the United States. In the wake of a new cluster of more than 150 new cases that emerged in Beijing, authorities sealed off neighborhoods, launched a mass testing campaign and imposed travel restrictions.
Meanwhile, President Trump maintains that the United States will not shut down a second time, although a surge in cases has convinced governors in some states, including Arizona, to walk back their opposition to mandatory face coverings in public.
Commentators and experts in Europe, where cases have continued to decline, voiced concerns over the state of the U.S. response. A headline on the website of Germany’s public broadcaster read: “Has the U.S. given up its fight against coronavirus?” Switzerland’s conservative Neue Zürcher Zeitung newspaper concluded, “U.S. increasingly accepts rising covid-19 numbers.”
“The only thing one can say with certainty: There’s nothing surprising about this development,” a journalist wrote in the paper, referring to crowded U.S. beaches and pools during Memorial Day weekend in May.
Some European health experts fear that the rising U.S. caseloads are rooted in a White House response that has at times deviated from the conclusions of leading scientists.
“Many scientists appeared to have reached an adequate assessment of the situation early on [in the United States], but this didn’t translate into a political action plan,” said Thomas Gerlinger, a professor of health sciences at the University of Bielefeld in Germany. For instance, it took a long time for the United States to ramp up testing capacity.
Whereas the U.S. response to the crisis has at times appeared disconnected from American scientists’ publicly available findings, U.S. researchers’ conclusions informed the actions of foreign governments.
“A large portion of [Germany’s] measures that proved effective was based on studies by leading U.S. research institutes,” said Karl Lauterbach, a Harvard-educated epidemiologist who is a member of the German parliament for the Social Democrats, who are part of the coalition government. Lauterbach advised the German parliament and the government during the pandemic.
Despite its far older population, Germany has confirmed fewer than 9,000 coronavirus-linked deaths, compared to almost 120,000 in the United States. (Germany has about one-fourth of the United States’ population.)
Lauterbach cited in particular the work of Marc Lipsitch, a professor of epidemiology at Harvard University, whose research with colleagues recently suggested that forms of social distancing may have to remain in place into 2022. Lipsitch’s work, Lauterbach said, helped him to convince German Vice Chancellor Olaf Scholz that the pandemic will be “the new normal” for the time being, and it impacted German officials’ thinking on how long their strategy should be in place.
Regarding the effectiveness of face masks, Lauterbach added, “we almost entirely relied on U.S. studies.” Germany was among the first major European countries to make face masks mandatory on public transport and in supermarkets.
Lipsitch said Thursday that he was not previously aware of the impact of his research on German decision-making, but added that he has spoken to representatives of several other foreign governments in recent weeks, including Israeli Prime Minister Benjamin Netanyahu and officials or advisers from Canada, New Zealand and South Korea.
Even though Lipsitch cautioned it was impossible for him to say how or if his conversations influenced foreign governments’ thinking, he credited the overall European response as “science-based and a sincere effort to find out what experts in the field believe is a range of possible scenarios and consequences of decisions.”
Lipsitch said he presented some of his research to a White House group in the early stages of the U.S. outbreak but said the Trump administration’s response to the pandemic did not reflect his conclusions. “I think they have cherry-picked models that at each point looked the most rosy, and fundamentally not engaged with the magnitude of the problem,” he said.
The White House has defended its approach as science-based. After a study by Imperial College London predicted 510,000 deaths in Britain and 2.2 million in the United States if the pandemic remained fully uncontrolled, for instance, the Trump administration indicated that it was taking the research into account.
“If we didn’t act quickly and smartly, we would have had, in my opinion and in the opinion of others, anywhere from 10 to 20 and maybe even 25 times the number of deaths,” Trump said two months later,
But European researchers dispute that the U.S. government’s reliance on scientists to inform decision-making comes anywhere near the degree to which many European policymakers have relied on researchers.
After consulting U.S. research and German studies, for instance, German leaders agreed to make reopening dependent on case numbers, meaning restrictions snap back or reopening gets put on hold if the case numbers in a given region exceed a certain threshold.
Meanwhile, several U.S. states have reopened despite rising case numbers.
“I don’t understand that logic,” said Reinhard Busse, a health management professor a the Technical University of Berlin.
Lauterbach said that while most Germans disapproved of Trump before the pandemic, even his staunchest critics in Germany were surprised by how even respected U.S. institutions including the Centers for Disease Control and Prevention (CDC) struggled to respond to the crisis.
The CDC, for instance, initially botched the rollout of test kits in the early stages of the outbreak.
“Like many other aspects of our country, the CDC’s ability to function well is being severely handicapped by the interference coming from the White House,” said Harvard epidemiologist Lipsitch. “All of us in public health very much hope that this is not a permanent condition of the CDC.”
Some observers fear the damage will be difficult to reverse. “I’ve always thought of the CDC as a reliable and trusted source of information,” said Wiles, the New Zealand specialist. “Not anymore.”
About 1.5 million people filed for state unemployment benefits last week, the Department of Labor announced Thursday, bringing the 13-week total for first-time claims to more than 45 million. Another 760,000 filed new claims for Pandemic Unemployment Assistance, a temporary program for workers such as independent contractors who ordinarily do not qualify for unemployment payments.
While new jobless claims continue to decline, falling for the 11th straight week, the numbers remain startlingly high relative to previous recessions, and some economists have expressed concerns that the labor market is not healing as rapidly as they had hoped.
“It’s not clear why claims are still so high,” said Ian Shepherdson, chief economist at Pantheon Macroeconomics, in a note to clients. “[I]s it the initial shock still working its way up through businesses away from the consumer-facing jobs lost in the first wave, or is it businesses which thought they could survive now throwing in the towel, or both? Either way, these are disappointing numbers and serve to emphasize that a full recovery is going to take a long time.”
With recent flare-up in neighboring counties, L.A.-area hospital leaders want the county to work with the state to keep surge hospitals open.
Healthcare officials on Tuesday called for Los Angeles County leaders to work with the state to reopen its “surge” hospital and recommended that another in Long Beach swing open its doors, citing the need to fully reopen medical centers while also dealing with an expected surge in coronavirus cases.
The state-funded Los Angeles Surge Hospital, which opened on April 13 at the former site of the St. Vincent Medical Center amid heightened concern about having enough beds to deal with Covid-19 patients, has closed.
But Dr. Hector Flores, an Adventist Health White Memorial physician, told the county’s Board of Supervisors and his fellow members on the county’s Economic Resiliency Task Force that county officials should work to bring it back online. He also recommended that Long Beach Community Hospital — which has long been on the cusp of reopening — become a surge hospital.
The context in June is different, however, than it was in March and April, when public health officials were intensely concerned that the county’s hospital capacity would be overwhelmed by a never-before-seen virus that was spreading and killing exponentially.
Along with many other businesses, hospitals, too, shut down many services in an effort to grow bed capacity for COVID-19 patients. But those services were essential for many hospitals’ bottom line — everything from elective procedures to vital surgeries. Couple that with patients who were delaying or outright canceling vital non-coronavirus visits, and in the first 90 days of the pandemic in L.A. County, hospitals — typically among the largest employers — were shedding jobs and occupancy (which fell to about 40% collectively, according to Flores).
“Hospitals are like hotels. If they are not fully occupied they are losing money,” said Flores, who heads a working group on the county’s task force.
Ultimately, the industry took an estimated $15 billion hit, he said, and only now, in the past two weeks is it starting to recover as health orders are eased and 15,000 doctors and medical support staffs make their way back to their once-shuttered practices.
Flores, and his committee of healthcare leaders have been devising a framework for recovery in the healthcare sector of the county’s economy. They want to maintain those jobs in the $100-billion-a-year healthcare industry.
It’s a larger goal among county leaders, who started the resiliency task force to figure out how several of the region’s economic sectors can recover after being shut down for months.
But there’s a looming concern: A second wave of the virus.
Flores said recent coronavirus spikes in Orange and Ventura counties — which saw large crowds gathering at beaches over the Memorial Day holiday — are giving him pause.
And that’s prompted Flores and others to call for the county to work with state officials to reopen and keep surge hospitals open. The move would help regular hospitals keep their non-COVID business going but allow for more capacity, if needed.
As it stands, non-COVID patients are coming back. Hospitals over the last two to three weeks have gone from 40% to 85% occupancy rates.
“What that tells us is that if there is a surge there won’t be the same capacity that we had for the first 90 days (of the pandemic),” he said. “We’re concerned about the uptick we see in Ventura and Orange County, since on Memorial Day weekend they opened beaches, hiking trails and parks. Sadly, many people took advantage of that open environment without protection of masks and often congregating in clusters. We’re also waiting to see the impact of the protests in two weeks.”
State and local officials have repeatedly said that public health data will guide local decisions, and have held out the possibility that public health orders could be re-tightened.
During Tuesday’s meeting, Supervisor Sheila Kuehl questioned whether Flores meant the county should keep surge hospitals “available” or actually open them.
Flores said as hospitals reopen and perform essential surgeries, they need “safe units” where patients can recover from an operation without the threat of being infected by the virus. And to do that, they need more space, he said.
“As we see a smaller number of beds available in hospitals, we are eventually going to rely on surge hospitals … because we anticipate there is quite likely going to be another surge if the patterns we see in Ventura and Orange counties come to play in Los Angeles,” Flores said.
The shuttered St. Vincent’s hospital, on a 10-acre campus in the Westlake District near Downtown Los Angeles, seemed essential when it was pressed into duty on April 13 after being closed in January. It quickly became part of the state’s plan to outfit roughly 50,000 more hospital beds to handle a surge of infected patients.
Ultimately, though, that surge never came. The hospital treated 65 people at a cost to taxpayers of nearly $15 million, the Southern California News Group reported.
It may very well stay that way. A spokesperson for the hospital said Tuesday that the hospital is “officially closed at the present time, there are no plans to reopen.”
Long Beach Community Hospital, too, was eyed. City leaders and officials from Molina, Wu, Network, Inc. — the hospital’s new operator — scurried to reopen it in the early COVID-19 days.
MWN said in late March that the facility was “days away” from opening, as Long Beach looked for capacity. That never came. Plus, the U.S. Navy hospital ship Mercy, which arrived in Los Angeles in late March to help treat non-coronavirus patients, returned to San Diego after treating just 77 patients.
Meanwhile, regular hospitals were scambling to find room for the expected surge of COVID patients. But between that and the March “Safer-at-Home” order, hospitals suffered the unintended consequence of furlough and layoffs related to a shortage of “non-essential” medical work.
The county’s Department of Health Services says the decision to reopen the St. Vincent’s property lies with the state, which in consultation with Dignity Health and Kaiser, closed down operations as its contract was due to run out by the end of June.
Could it come back online?
“The opinion of the County is that a) currently we project having sufficient overall beds in the county to meet demand (with the exception of ICU which can be resolved by flexing bed types within existing hospitals) and b) surging our existing hospitals,” according to a statement.
Officials say adding beds at existing hospitals is a “better approach” because it makes use of the existing infrastructure. County health services officials add that all hospitals have the ability “to surge patients at least 20% above their normal capacity.”
As for Long Beach Community Hospital, health officials noted that it has not yet been approved to operate by licensing through the state.
“We would welcome LBCH coming on line as an additional acute care hospital, but need for them to meet state licensing criteria,” according to the statement.
L.A. County Public Health officials predict that with no change in the transmission rate of the disease, the demand for hospital beds will remain relatively stable, with some slight “up-trending” because of the easing of health-order restrictions.
Hospitalizations across the county were down to 1,285 as of Monday from a peak of nearly 2,000 in late April. While the numbers have been down considerably, some hospitals have experienced a slight uptick in recent days. Whether that increase is the result of an oncoming surge has yet to be seen, according to Molly Lawson, spokeswoman for Centinela Hospital Medical Center in Inglewood.
“It’s really too early to tell,” Lawson said. “This week we had anticipated seeing the community impact of some of the protests and marches and all the activities happening of late.”
Centinela Hospital, which according to Lawson had one of the higher levels of hospitalization rates, treated about 70 COVID-19 patients in late April and early May. Patients occupied two full units, Lawson said. As of Tuesday, the hospital had 17 patients, just half a unit.
At Torrance Memorial Medical Center, which saw a peak of about 55 patients just as “Safer-at-Home” orders went into effect in late March, the hospital has been treating 15 to 21 patients for the past several weeks, according to spokeswoman Sandy Rodriguez. The lowest number of COVID-19 patients the hospital had admitted was 11.
“We have seen some intermittent increases, but no surge,” Rodriguez said.
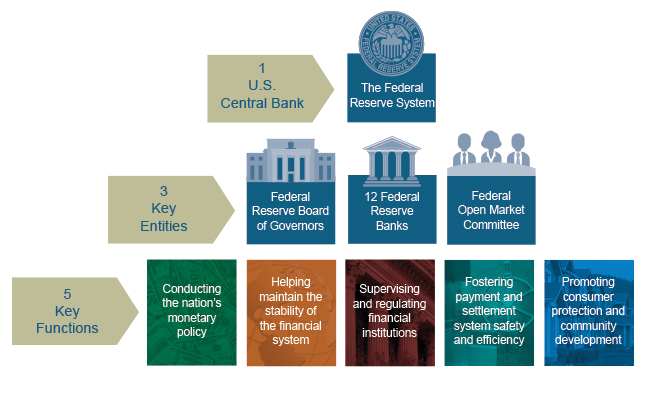
Chair Powell submitted identical remarks to the Committee on Financial Services, U.S. House of Representatives, Washington, D.C., on June 17, 2020.
Chairman Crapo, Ranking Member Brown, and other members of the Committee, thank you for the opportunity to present the Federal Reserve’s semiannual Monetary Policy Report.
Our country continues to face a difficult and challenging time, as the pandemic is causing tremendous hardship here in the United States and around the world. The coronavirus outbreak is, first and foremost, a public health crisis. The most important response has come from our health-care workers. On behalf of the Federal Reserve, I want to express our sincere gratitude to these dedicated individuals who put themselves at risk, day after day, in service to others and to our nation.
Current Economic Situation and Outlook
Beginning in mid-March, economic activity fell at an unprecedented speed in response to the outbreak of the virus and the measures taken to control its spread. Even after the unexpectedly positive May employment report, nearly 20 million jobs have been lost on net since February, and the reported unemployment rate has risen about 10 percentage points, to 13.3 percent. The decline in real gross domestic product (GDP) this quarter is likely to be the most severe on record. The burden of the downturn has not fallen equally on all Americans. Instead, those least able to withstand the downturn have been affected most. As discussed in the June Monetary Policy Report, low-income households have experienced, by far, the sharpest drop in employment, while job losses of African Americans, Hispanics, and women have been greater than that of other groups. If not contained and reversed, the downturn could further widen gaps in economic well-being that the long expansion had made some progress in closing.
Recently, some indicators have pointed to a stabilization, and in some areas a modest rebound, in economic activity. With an easing of restrictions on mobility and commerce and the extension of federal loans and grants, some businesses are opening up, while stimulus checks and unemployment benefits are supporting household incomes and spending. As a result, employment moved higher in May. That said, the levels of output and employment remain far below their pre-pandemic levels, and significant uncertainty remains about the timing and strength of the recovery. Much of that economic uncertainty comes from uncertainty about the path of the disease and the effects of measures to contain it. Until the public is confident that the disease is contained, a full recovery is unlikely.
Moreover, the longer the downturn lasts, the greater the potential for longer-term damage from permanent job loss and business closures. Long periods of unemployment can erode workers’ skills and hurt their future job prospects. Persistent unemployment can also negate the gains made by many disadvantaged Americans during the long expansion and described to us at our Fed Listens events. The pandemic is presenting acute risks to small businesses, as discussed in the Monetary Policy Report. If a small or medium-sized business becomes insolvent because the economy recovers too slowly, we lose more than just that business. These businesses are the heart of our economy and often embody the work of generations.
With weak demand and large price declines for some goods and services—such as apparel, gasoline, air travel, and hotels—consumer price inflation has dropped noticeably in recent months. But indicators of longer-term inflation expectations have been fairly steady. As output stabilizes and the recovery moves ahead, inflation should stabilize and then gradually move back up over time closer to our symmetric 2 percent objective. Inflation is nonetheless likely to remain below our objective for some time.
Monetary Policy and Federal Reserve Actions to Support the Flow of Credit
The Federal Reserve’s response to this extraordinary period is guided by our mandate to promote maximum employment and stable prices for the American people, along with our responsibilities to promote the stability of the financial system. We are committed to using our full range of tools to support the economy in this challenging time.
In March, we quickly lowered our policy interest rate to near zero, reflecting the effects of COVID-19 on economic activity, employment, and inflation, and the heightened risks to the outlook. We expect to maintain interest rates at this level until we are confident that the economy has weathered recent events and is on track to achieve our maximum-employment and price-stability goals.
We have also been taking broad and forceful actions to support the flow of credit in the economy. Since March, we have been purchasing sizable quantities of Treasury securities and agency mortgage-backed securities in order to support the smooth functioning of these markets, which are vital to the flow of credit in the economy. As described in the June Monetary Policy Report, these purchases have helped restore orderly market conditions and have fostered more accommodative financial conditions. As market functioning has improved since the strains experienced in March, we have gradually reduced the pace of these purchases. To sustain smooth market functioning and thereby foster the effective transmission of monetary policy to broader financial conditions, we will increase our holdings of Treasury securities and agency mortgage-backed securities over coming months at least at the current pace. We will closely monitor developments and are prepared to adjust our plans as appropriate to support our goals.
To provide stability to the financial system and support the flow of credit to households, businesses, and state and local governments, the Federal Reserve, with the approval of the Secretary of the Treasury, established 11 credit and liquidity facilities under section 13(3) of the Federal Reserve Act. The June Monetary Policy Report provides details on these facilities, which fall into two categories: stabilizing short-term funding markets and providing more-direct support for credit across the economy.
To help stabilize short-term funding markets, the Federal Reserve set up the Commercial Paper Funding Facility and the Money Market Liquidity Facility to stem rapid outflows from prime money market funds. The Fed also established the Primary Dealer Credit Facility, which provides loans against good collateral to primary dealers that are critical intermediaries in short-term funding markets.
To more directly support the flow of credit to households, businesses, and state and local governments, the Federal Reserve established a number of facilities. To support the small business sector, we established the Paycheck Protection Program Liquidity Facility to bolster the effectiveness of the Coronavirus Aid, Relief, and Economic Security Act’s (CARES Act) Paycheck Protection Program. Our Main Street Lending Program, which we are in the process of launching, supports lending to both small and midsized businesses. The Term Asset-Backed Securities Loan Facility supports lending to both businesses and consumers. To support the employment and spending of investment-grade businesses, we established two corporate credit facilities. And to help U.S. state and local governments manage cash flow pressures and serve their communities, we set up the Municipal Liquidity Facility.
The tools that the Federal Reserve is using under its 13(3) authority are appropriately reserved for times of emergency. When this crisis is behind us, we will put them away. The June Monetary Policy Report reviews the implications of these tools for the Federal Reserve’s balance sheet.
Many of these facilities have been supported by funding from the CARES Act. We will be disclosing, on a monthly basis, names and details of participants in each such facility; amounts borrowed and interest rate charged; and overall costs, revenues, and fees for each facility. We embrace our responsibility to the American people to be as transparent as possible, and we appreciate that the need for transparency is heightened when we are called upon to use our emergency powers.
We recognize that our actions are only part of a broader public-sector response. Congress’s passage of the CARES Act was critical in enabling the Federal Reserve and the Treasury Department to establish many of the lending programs. The CARES Act and other legislation provide direct help to people, businesses, and communities. This direct support can make a critical difference not just in helping families and businesses in a time of need, but also in limiting long-lasting damage to our economy.
I want to end by acknowledging the tragic events that have again put a spotlight on the pain of racial injustice in this country. The Federal Reserve serves the entire nation. We operate in, and are part of, many of the communities across the country where Americans are grappling with and expressing themselves on issues of racial equality. I speak for my colleagues throughout the Federal Reserve System when I say, there is no place at the Federal Reserve for racism and there should be no place for it in our society. Everyone deserves the opportunity to participate fully in our society and in our economy.
We understand that the work of the Federal Reserve touches communities, families, and businesses across the country. Everything we do is in service to our public mission. We are committed to using our full range of tools to support the economy and to help assure that the recovery from this difficult period will be as robust as possible.
China is moving rapidly to seal off its capital of 22 million residents by canceling flights and trains amid growing fears that a potential second wave of covid-19 is gathering strength in Beijing and could spread to the rest of the country.
Authorities on Wednesday canceled 1,200 flights in and out of Beijing’s two airports and sharply reduced long-distance bus services. Beijingers were banned from making nonessential trips outside the city and required to take nucleic tests before they leave, municipal officials said at a briefing where they announced 31 new cases of the novel coronavirus.
While Beijing’s case numbers are low by global standards, they are vexing Chinese authorities who had touted their success in quickly stamping out the coronavirus and had taken pains to ensure it would not infect the seat of the ruling Communist Party. Government officials announced “wartime” measures on Saturday after dozens of cases were discovered at the Xinfadi wholesale market in southwest Beijing, which carried worrying echoes of the original outbreak in Wuhan late last year.
In the days since, Beijing has steadily reintroduced stricter measures, potentially foreshadowing the difficulty that many governments could face in warding off future waves of covid-19.
After classes resumed just a month ago, Beijing’s schools were again shut on Wednesday, as were some gyms, swimming pools and public attractions. The city raised its emergency response to the second-highest level, and entry and exit checkpoints and temperature checks returned to neighborhoods in the city center. The scenes were reminiscent of those during the outbreak’s peak in February and March, albeit with less-strict lockdown measures.
The risk of people in Beijing traveling in and out of the city and spreading infections countrywide is “severe,” acknowledged Chen Bei, Beijing’s deputy party chief. “We need to take decisive action . . . resolutely control this gathering epidemic and resolutely curb its spread inside and outside the city,” Chen said.
Officials said Beijing has tested 3.56 million people since June 13, underscoring the extent of their concern.
Adding to a sense of frustration with the virus’s reemergence, Chinese experts said it may have been lurking undetected for weeks.
“The Beijing outbreak very likely didn’t start in June, or May, but a month before that,” Gao Fu, head of the Chinese Center for Disease Control and Prevention, told reporters in Shanghai. “There can only be so many cases around us now if there were already many people with no symptoms or light symptoms back then. This is our current speculation, but we need to verify it.”
Chinese researchers say they are examining how the coronavirus made a sudden comeback. Fears that shipped livestock and produce could carry the virus — with potentially worrisome implications for international trade — began circulating this week after it was found at the Xinfadi market on cutting boards used for salmon, which is imported from Europe. The genetic material of viruses found at the market and in patients in Beijing also matched sequences typically found in patients in Europe.
Although the theory was fanned this week by nationalist media outlets including the party-run Global Times — which seized the opportunity to question whether the entire pandemic originated last year in Europe instead of China — Chinese and international experts, including the U.S. Food and Drug Administration, say there is relatively scant evidence that the virus is transmitted on food and packaging.
Wu Zunyou, the Chinese CDC’s top epidemiologist, said Tuesday that the virus was also found throughout the hall of the Xinfadi market, suggesting that the salmon was not necessarily the source. The strain of the virus found in Xinfadi is also prevalent in the United States, Wu added.
Michael Ryan, executive director of the World Health Organization’s Health Emergencies Program, also played down concerns about shipped food as a viral vector, saying the matter requires more study. “I’d be reticent to be in the position where all packaging and other things would need to be systematically tested,” Ryan said. “I don’t think it’s the primary hypothesis, but it needs to be explored.”
Meanwhile, supermarkets and restaurants in Beijing are not taking chances and have stopped selling salmon. The Beijing government said Wednesday it would carry out nucleic testing on all close contacts of people who visited the Xinfadi market, as well as workers in the city’s restaurants, which could number hundreds of thousands of people.
Cases in Beijing are expected to keep rising in the coming days because Xinfadi, which spans an area the size of 250 football fields, is such a large and central part of Beijing’s food distribution network, city officials warned.
As the capital fell again into quasi-lockdown this week, other Chinese cities, including Shanghai, began issuing quarantine requirements and restrictions for travelers from Beijing — a sudden reversal for residents who in normal times enjoy a privileged status.
Officials and state media have called for understanding and cooperation from Beijing residents while rallying citizens nationwide behind the city.
“Go Beijing! Go Zhajiang noodles!” said one popular meme on social media, referring to a classic Beijing dish.
ProPublica deputy managing editor Charles Ornstein wanted to know why experts were wrong when they said U.S. hospitals would be overwhelmed by COVID-19 patients. Here’s what he learned, including what hospitals can do before the next wave.
The prediction from New York Gov. Andrew Cuomo was grim.
In late March, as the number of COVID-19 cases was growing exponentially in the state, Cuomo said New York hospitals might need twice as many beds as they normally have. Otherwise there could be no space to treat patients seriously ill with the new coronavirus.
“We have 53,000 hospital beds available,” Cuomo, a Democrat, said at a briefing on March 22. “Right now, the curve suggests we could need 110,000 hospital beds, and that is an obvious problem and that’s what we’re dealing with.”
The governor required all hospitals to submit plans to increase their capacity by at least 50%, with a goal of doubling their bed count. Hospitals converted operating rooms into intensive care units, and at least one replaced the seats in a large auditorium with beds. The state worked with the federal government to open field hospitals around New York City, including a large one at the Jacob K. Javits Convention Center.
But when New York hit its peak in early April, fewer than 19,000 people were hospitalized with COVID-19. Some hospitals ran out of beds and were forced to transfer patients elsewhere. Other hospitals had to care for patients in rooms that had never been used for that purpose before. Supplies, medications and staff ran low. And, as The Wall Street Journal reported on Thursday, many New York hospitals were ill prepared and made a number of serious missteps.
All told, more than 30,000 New York state residents have died of COVID-19. It’s a toll worse than any scourge in recent memory and way worse than the flu, but, overall, the health care system didn’t run out of beds.
“All of those models were based on assumptions, then we were smacked in the face with reality,” said Robyn Gershon, a clinical professor of epidemiology at the NYU School of Global Public Health, who was not involved in the models New York used. “We were working without situational awareness, which is a tenet in disaster preparedness and response. We simply did not have that.”
Cuomo’s office did not return emails seeking comment, but at a press briefing on April 10, the governor defended the models and those who created them. “In fairness to the experts, nobody has been here before. Nobody. So everyone is trying to figure it out the best they can,” he said. “Second, the big variable was, what policies do you put in place? And the bigger variable was, does anybody listen to the policies you put in place?”
So, why were the projections so wrong? And how can political leaders and hospitals learn from the experience in the event there is a second wave of the coronavirus this year? Doctors, hospital officials and public health experts shared their perspectives.
The Models Overstated How Many People Would Need Hospital Care
The models used to calculate the number of people who would need hospitalization were based on assumptions that didn’t prove out.
Early data from the U.S. Centers for Disease Control and Prevention suggested that for every person who died of COVID-19, more than 11 would be hospitalized. But that ratio was far too high and decreased markedly over time, said Dr. Christopher J.L. Murray, director of the Institute for Health Metrics and Evaluation at the University of Washington. IHME’s earliest models on hospitalizations were based on that CDC data and predicted that many states would quickly run out of hospital beds.
A subsequent model, released in early April, assumed about seven hospitalizations per death, reducing the predicted surge. Currently, Murray said, the ratio is about four hospital admissions per death.
“Initially what was happening and probably what we saw in the CDC data is doctors were admitting anybody they thought had COVID,” Murray said. “With time they started admitting only very sick people who needed oxygen or more aggressive care like mechanical ventilation.”
A patient with COVID-19 is taken into Mount Sinai Hospital in New York on May 3. (Alexi Rosenfeld/Getty Images)
A model created by the Harvard Global Health Institute made a different assumption that also turned out to be too high. Data from Wuhan, China, suggested that about 20% of those known to be infected with COVID-19 were hospitalized. Harvard’s model, which ProPublica used to build a data visualization, assumed a hospitalization rate in the United States of 19% for those under 65 who were infected and 28.5% for those older than 65.
But in the U.S., that percentage proved much too high. Official hospitalization rates vary dramatically among states, from as low as 6% to more than 20%, according to data gathered from states by The COVID Tracking Project. (States with higher rates may not have an accurate tally of those infected because testing was so limited in the early weeks of the pandemic.) As testing increases and doctors learn how to treat coronavirus patients out of the hospital, the average hospitalization rate continues to drop.
New York state’s testing showed that by mid-April, approximately 20% of the adult population in New York City had antibodies to COVID-19. Given the number hospitalized in the city and adjusting for the time needed for the body to produce antibodies, this means that the city’s hospitalization rate was closer to 2%, said Dr. Nathaniel Hupert, an associate professor at Weill Cornell Medicine and co-director of the Cornell Institute for Disease and Disaster Preparedness.
Dr. Ashish Jha, director of the Harvard Global Health Institute, and his team also assumed that between 20% and 60% of the population would be infected with COVID-19 over six to 18 months. That was before stay-at-home orders took effect nationwide, which slowed the virus’s spread. Outside of New York City, a far lower percentage of the population has been infected. Granted, we’re not even six months into the pandemic.
A number of factors go into disease models, including the attack rate (the percentage of the entire population that eventually becomes infected), the symptomatic rate (how many people are going to show symptoms), the hospitalization rate for different age groups, the fraction of those hospitalized that will need intensive care and how much care they will need, as well as how the disease travels through the population over time (what is known as “the shape of the epidemic curve”), Hupert said.
Before mid-March, Hupert’s best estimate of the impact of COVID-19 in New York state was that it would lead to a peak hospital occupancy of between 13,800 to 61,000 patients in both regular medical wards and intensive care. He shared his work with state officials.
David Muhlestein, chief strategy and chief research officer at Leavitt Partners, a health care consulting firm, said one takeaway from COVID-19 is that models can’t try to predict too far into the future. His firm has created its own projection tool for hospital capacity that looks ahead three weeks, which Muhlestein said is most realistic given the available data.
“If we were held to our very initial projection of what was going to happen, everybody would be very wrong in every direction,” he said.
Hospitals Proved Surprisingly Adept at Adding Beds
When calculating whether hospitals would run out of beds, experts used as their baseline the number of beds in use in each hospital, region and state. That makes sense in normal times because hospitals have to meet stringent rules before they are able to add regular beds or intensive care units.
Workers prepare dozens of extra beds that were delivered to Mount Sinai on March 31. (Spencer Platt/Getty Images)
But in the early weeks of the pandemic, state health departments waived many rules and hospitals responded by increasing their capacity, sometimes dramatically. “Just because you only have six ICU beds doesn’t mean they will only have six ICU beds next week,” Muhlestein said. “They can really ramp that up. That’s one of the things we’re learning.”
Take Northwell Health, a chain of 17 acute-care hospitals in New York. Typically, the system has 4,000 beds, not including maternity beds, neonatal intensive care unit beds and psychiatric beds. The system grew to 6,000 beds within two weeks. At its peak, on April 7, the hospitals had about 5,500 patients, of which 3,425 had COVID-19.
The system erected tents, placed patients in lobbies and conference rooms, and its largest hospital, North Shore University Hospital, removed the chairs from its 300-seat auditorium and replaced them with a unit capable of treating about 50 patients. “We were pulling out all the stops at that point,” Senior Vice President Terence Lynam said. “It was unclear if the trend was going to go the other way. We did not end up needing them all.”
Northwell went from treating 49 COVID-19 inpatients on March 16 to 3,425 on April 7. “I don’t think anybody had a clear handle on what the ceiling was going to be,” Lynam said. As of Wednesday, the system was still caring for 367 COVID-19 patients in its hospitals.
As hospitals found ways to expand, government leaders worked with the Army Corps of Engineers to build dozens of field hospitals across the country, such as the one at the Javits Center. According to an analysis of federal spending by NPR, those efforts cost at least $660 million. “But nearly four months into the pandemic, most of these facilities haven’t treated a single patient,” NPR reported. As they began to come online, stay-at-home orders started producing results, with fewer positive cases and fewer hospitalizations.
Demand for Non-COVID-19 Care Plummeted More Than Expected
Hospitals across the country canceled elective surgeries, from hip replacements to kidney transplants. That greatly reduced the number of non-COVID-19 patients they had to treat. “We generated a lot more capacity by getting rid of elective procedures than any of us thought was possible,” Harvard’s Jha said.
Northwell canceled elective surgeries on March 16, and over the span of the next week and a half, its hospitals discharged several thousand patients in anticipation of the coming surge. “In retrospect, it was a wise move,” Lynam said. “It just ballooned after that. If we had not discharged those patients in time, there would have been a severe bottleneck.”
What’s more, experts say, it’s clear that some patients with true emergencies also stayed home. A recent report from the CDC said that emergency room visits dropped by 42% in the early weeks of the pandemic. In 2019, some 2.1 million people visited ERs each week from late March to late April. This year, that dropped to 1.2 million per week. That was especially true for children, women and people who live in the Northeast.
In New York City, emergency room visits for asthma practically ceased entirely at the peak, Cornell’s Hupert said. “You wouldn’t imagine that asthma would just disappear,” he said. “Why did it go away? … Nobody has seen anything like that.”
Undoubtedly some people experienced heart attacks and strokes and didn’t go to the hospital because they were fearful of getting COVID-19. “I didn’t expect that,” Jha said. A draft research paper available on a preprint server, before it is reviewed and published in an academic journal, found that heart disease deaths in Massachusetts were unchanged in the early weeks of the pandemic compared to the same period in 2019. What that may mean is that those people died at home.
The Coronavirus Attacked Every Region at a Different Pace
Some initial models forecast that COVID-19 would hit different regions in similar ways. That has not been the case. New York was hit hard early; California was not, at least initially.
In recent weeks, hospitals in Montgomery, Alabama, saw a lot of patients. Arizona’s health director has told hospitals in the state to “fully activate” their emergency plans in light of a spike in cases there. The Washington Post reported on Tuesday that hospitalizations in at least nine states have been rising since Memorial Day.
St. Luke’s, a closed hospital in Phoenix, is prepared to receive overflow patients on April 23. Arizona initially wasn’t hit hard, but cases are now spiking. (Ross D. Franklin/AP Photo)
Dr. Mark Rupp, medical director of the Department of Infection Control and Epidemiology at the University of Nebraska Medical Center in Omaha, said his region hasn’t seen a tidal wave like New York. “What we’ve seen is a rising tide, a steady increase in the number of cases.” Initially that was associated with outbreaks at specific locations like meatpacking and food processing plants and to some degree long-term care facilities.
But since then, “it has just plateaued,” he said. “That has me concerned. This is a time when I feel like we should be working as hard as we can to push these numbers as low as possible.”
Rupp’s hospital has been caring for 50 to 60 COVID-19 patients on any given day. The hospital has started to perform surgeries and procedures that had been on hold because “elective cases stay elective for only so long.”
The hospital’s general medical/surgical beds are 70% to 80% filled, and its ICU beds are 80% to 90% full. “We don’t have a big cushion.”
Even in New York City, the virus hit boroughs differently. Queens and the Bronx were hard hit; Manhattan, Brooklyn and Staten Island less so. “Maybe we can’t even model a city as big as New York,” Hupert said. “Each neighborhood seemed to have a different type of outbreak.”
That needs further study but could be attributable to both social and demographic conditions and the type of jobs residents of the neighborhoods had, among other factors.
What We Can Learn From Coronavirus “Round One”
While hospitals were able to add beds more quickly than experts realized they could, some other resources were harder to come by. Masks, gowns and other personal protective equipment were tough to get. So were ventilators. Anesthesia agents and dialysis medications were in short supply. And every additional bed meant the need for more doctors, nurses and respiratory therapists.
In early February, before any cases were discovered in New York, Northwell purchased $5 million in PPE, ventilators and lab supplies just in case, Lynam said. “It turned out to be a wise move,” he said. “What’s clear is that you can never have enough.”
Northwell has spent $42 million on PPE alone. “We were going through 10,000 N95 masks a day, just a crazy amount,” he said. “One of the lessons learned is you have to stockpile the PPE. There’s got to be a better procurement process in place.”
If there’s one thing the system could have done differently, Lynam said, it’s bringing in more temporary nurses earlier. Northwell brought in 500 nurses from staffing agencies. “They came in a week later than they should have.”
Dr. Robert Wachter, chair of the department of medicine at the University of California, San Francisco, agreed. “I’ve helped run services in hospitals for 25 years,” he said. “I’ve probably given two minutes of thought to the notions of supply chains and PPE. You realize that is absolutely central to your preparedness. That’s a lesson.”
Experts and hospital leaders agree that everyone can do better if another wave hits. Here’s what that entails:
Having testing readily available, as it now is, to more quickly spot a resurgence of the virus.
Stocking up now on PPE and other supplies. “We definitely have to stockpile PPE by the fall,” Gershon of NYU said. “We have to. … [Hospitals and health departments] have to really get those contracts nailed down now. They should have been doing this, of course, all the time, but no one expected this kind of event.”
Being able to quickly move personnel and equipment from one hot spot to the next.
Planning for how to care for those with other medical ailments but who are scared of contracting COVID-19. “We have to have some sort of a mechanism by which we can offer people assurance that if they come in, they won’t get sick,” Jha said. “We can’t repeat in the fall what we just did in the spring. It’s terrible for hospitals. It’s terrible for patients.”
Providing mental health resources for front-line caregivers who have been deeply affected by their work. The intensity of the work, combined with watching patients suffer and die alone, was immensely taxing.
Coming up with ways to allow visitors in the hospital. Wachter said the visitor bans in place at many hospitals, though well intentioned, may have backfired. “When all hell was breaking loose and we were just doing the best we could in the face of a tsunami, it was reasonable to just keep everybody out,” he said. “We didn’t fully understand how important that was for patients, how much it might be contributing to some people not coming in for care when they really should have.”
Lynam of Northwell said he’s worried about what lies ahead. “You look back on the 1918 Spanish flu and the majority of victims from that died in the second wave. … We don’t know what’s coming on the second wave. There may be some folks who say you’re paranoid, but you’ve got to be prepared for the worst.”
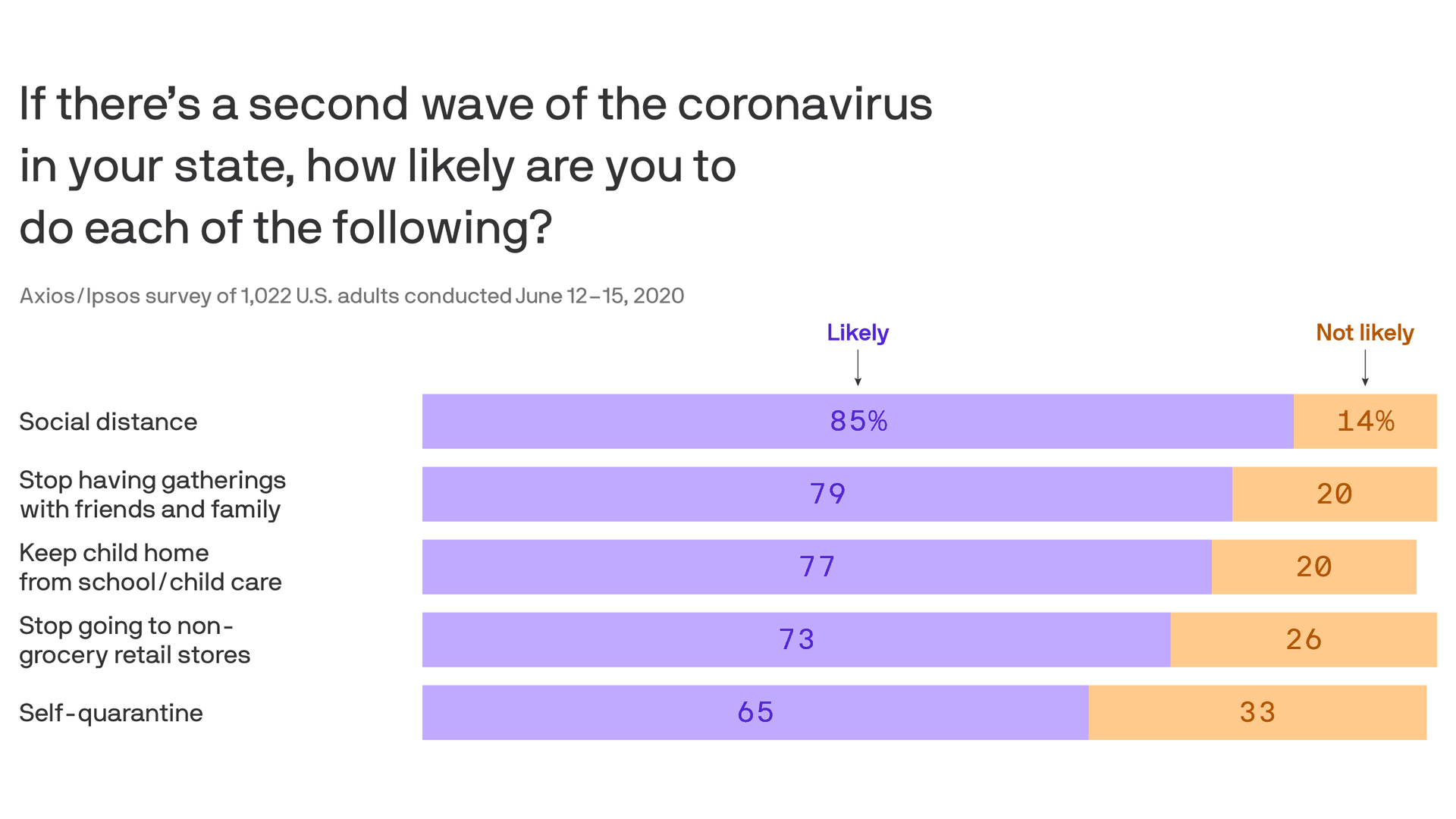
Eight in 10 Americans are worried about a second wave of the coronavirus, with large majorities saying they’ll resume social distancing, dial back shopping and keep their kids out of school if it happens, in Week 13 of the Axios-Ipsos Coronavirus Index.
Why it matters: Businesses and schools around the country are trying to assess how quickly and fully they should reopen based in part on what Americans will demand and tolerate. These findings underscore the challenges in predicting how they should proceed.
But getting Americans to swallow a second round of 14-day self-quarantining could be tougher than getting them to go back to social distancing, with one in three saying they likely won’t do it.
The biggest factor is partisan identification, with 81% of Democrats but only 49% of Republicans saying they’ll self-quarantine if a second wave hits.
The big picture: The latest installment of our national weekly survey shows a renewed sense of risk following reports of new hospitalizations since states began lifting stay-at-home orders — but quarantine fatigue is still driving people to take their chances.
People’s assessment of large or moderate risk grew last week for each of these categories: returning to their normal workplace, dining out, retail shopping, going to the hair salon or participating in protests.
But the share of those going out to eat rose from 31% to 41%. Those visiting friends or relatives rose from 56% to 60%. Those getting their hair done rose from 26% to 31%. Those attending demonstrations rose from 11% to 14%.
What they’re saying: “People are starting to be concerned about it again,” said pollster Chris Jackson, senior vice president for Ipsos Public Affairs. “We’re not yet seeing changes in the patterns of their behavior yet, though.”
“Their behaviors are not really catching up to their concern level.”
By the numbers: 81% say they’re concerned about a second wave — including those who are extremely (30%), very (26%) or somewhat (24%) concerned.
64% of those surveyed say returning to their normal pre-coronavirus life represents a large or moderate risk, up from 57% a week ago.
The share of people extremely or very concerned about getting sick rose from 32% to 40% last week. Those fearing U.S. economic collapse rose from 48% to 54%.
There also were upticks in people’s concerns about job security and the government’s response to the outbreak.
Americans’ ability to afford household goods also decreased.
One in 10 surveyed say they’ve been collecting unemployment benefits in recent weeks.
35% of Americans now know someone who’s tested positive, a new high for the survey.
Between the lines: The survey suggests an evolving understanding of the racial disparities in the pandemic.
The share of those saying they are extremely or very concerned that the coronavirus is doing greater damage to people of color rose from 36% to 42%.
The share of those extremely or very concerned that official responses are biased against certain groups also rose from 36% to 42%.