The State Department issued a global level 3 health advisory late Wednesday advising Americans to “reconsider travel abroad due to the global impact” of the novel coronavirus pandemic.
The big picture: President Trump announced hours earlier European travel to the U.S. will be restricted for 30 days, with some exemptions, and the NBA suspended its season. There are more than 126,000 cases in over 100 countries and territories and more than 4,600 deaths. There are over 1,300 cases in the U.S.
LAST 48 HOURS
- Travel restrictions: The Trump administration’s new rules affect European member states of the Schengen Area, which includes most but not all of the EU. The United Kingdom and Ireland are not in the zone and are not affected by the restrictions.
- In Israel, all travelers entering from any country — including Israeli citizens — are required to self-quarantine for 14 days.
- Travel advisory: “Many areas throughout the world are now experiencing COVID-19 outbreaks and taking action that may limit traveler mobility, including quarantines and border restrictions,” the State Department advisory reads. “Even countries, jurisdictions, or areas where cases have not been reported may restrict travel without notice.”
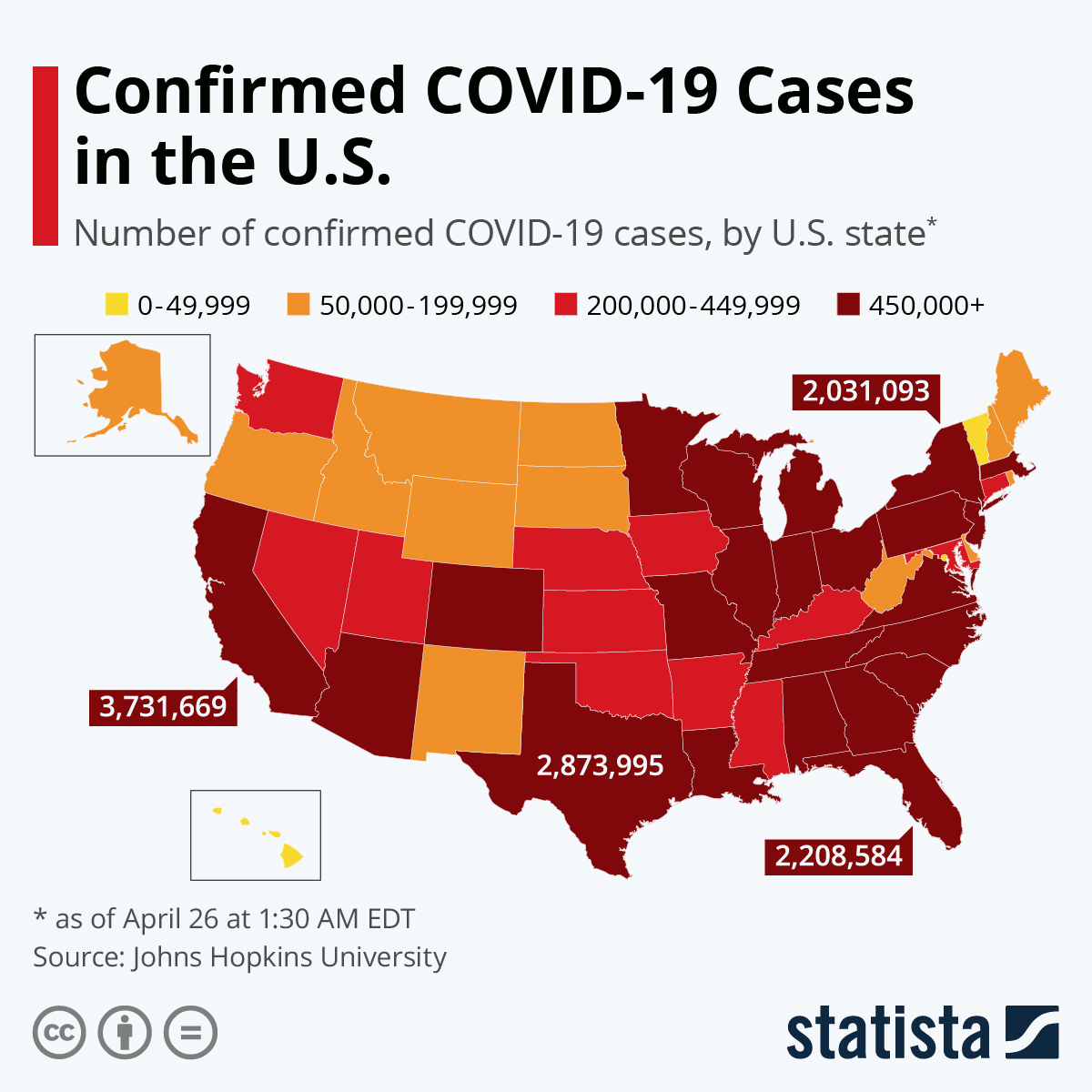
- U.S. cases: Nearly 40 states reported at least 1,220 cases as of Wednesday, and roughly two dozen have declared a state of emergency. The novel coronavirus has now killed at least 30 Americans in five states.
- Washington, D.C., Mayor Muriel Bowser announced a state of emergency Wednesday, as well as six new COVID-19 cases. There are now 10 presumptive cases in D.C. — including person-to-person transmission and at least two individuals who contracted the virus from unknown causes.
- A staffer in the D.C. office of Sen. Maria Cantwell (D-Wash.) has tested positive to the virus — the first known case of a congressional staffer becoming infected with the virus.
- California’s Los Angeles County announced six additional cases on Wednesday — including one that health officials presume is the county’s second case of community spread transmission.
- The state’s health officials now recommend that events larger than 250 people be canceled.
- There are now four deaths in California after Los Angeles County announced Wednesday the death of an “older adult” who “traveled extensively over the past month,” including to South Korea.
- Virginia announced that a teenager in the Chickahominy Health District, who recently traveled internationally, has tested positive for COVID-19 on Wednesday, marking 9 current cases in the state. The affected teen did not attend school.
- The states with the most cases as of Wednesday are: Washington, New York and California — where three TSA officers at Mineta San Jose International Airport were confirmed to have tested positive for the virus Tuesday night.
- Maryland now has 9 confirmed cases after a 70-year-old Montana resident who was visiting Anne Arundel County came in close contact with someone who had contracted the virus, Maryland Gov. Larry Hogan said Wednesday.
- New York Gov. Andrew Cuomo said he planned to deploy the National Guard to the New York City suburb New Rochelle on Tuesday to establish a one-mile “containment zone” and help contain the spread of the novel coronavirus.
- Pandemic classification: The World Health Organization classified the outbreak as a pandemic Wednesday.
- Global impact: Cases continue to surge in Spain, Germany, France and Italy, which is on complete lockdown with more than 12,000 cases — second-highest to China.
- Business: Twitter announced Wednesday night that it instructed all employees globally to work from home.
- Google recommended Tuesday that all its employees in North America work from home until at least April 10 amid the novel coronavirus outbreak, one of the most sweeping cautionary edicts.
- The Securities and Exchange Commission is the first federal agency to direct its staff at its D.C. office to work remotely after an employee with respiratory problems was told they may have the virus.
- IBM is encouraging its employees who live or work in New York City and Westchester County to work from home. Amazon, Facebook, Microsoft and Salesforce have similar practices in place.
- Deloitte has recommended its staff return from areas impacted by COVID-19 to work from home for 14 days from their return date. The consulting firm has asked workers to defer nonessential international and domestic travel.
- Australia: Actor Tom Hanks confirmed Wednesday he and his wife, Rita Wilson, tested positive for the virus while in Australia, which now has 128 cases.
- Federal aid: The Department of Health and Human Services announced Wednesday it is allocating over $560 million to states and local areas to assist with COVID-19 response.
- Cruise ship: Nearly 300 people left the docked Grand Princess ship in Oakland, Calif. on Tuesday, with more than half sent to Travis Air Force base and 98 to Lackland Air Force base in Texas, Gov. Gavin Newsom said Tuesday.
- Community spread warning: Some areas in the U.S. have passed the point of containment and communities should focus on mitigation plans, such as canceling events, CDC director Robert Redfield said Tuesday.
- The Centers for Medicare & Medicaid Services asked nursing homes to limit visitation due to the high amount of deaths and greater risk for people over 60 and/or with underlying health conditions have.
- Seniors should limit unnecessary travel and exposure to large public gatherings, the officials said.
- Conferences and events: Music festival Coachella has been postponed until October. Many international and domestic conferences affecting all businesses, trades and entertainment are being either postponed or canceled.
- Several congressmen are under self-quarantine after they came in contact with a CPAC attendee who tested positive.
- Financial impact: U.S. stocks have taken a toll with various dips and corrections all week. Worries are growing that the outbreak could shrink global GDP and perhaps sink the U.S. dollar.
- Oil: Already struggling with mounting debt and falling market valuations, energy companies are at serious risk for mass bond defaults.
- Diagnostics: Health insurers and regulators are working to ensure coronavirus diagnostic tests are covered — but that doesn’t necessarily mean COVID-19 treatment will be affordable. Concerns linger as to how the health care system can meet the demands of high-volume testing.
- Universities: As colleges cancel classes and boot students off campus because of the coronavirus, they’re creating logistical and financial nightmares that could leave many students in a bind.
- Tourism: White House advisers are looking at policy changes to help relieve the travel and hospitality industry. Tourism and travel operators have had to reprice globally, as airlines, hotels and travel operators see major declines in bookings and revenue.
- Social media: A large part of the problem is the “infodemic,” as stories get shared that are designed to drive fear rather than build understanding about the illness, according to NewsWhip data provided to Axios.