



Earlier this year, I shattered my elbow in a freak fall, requiring surgery, plates and screws. While I am a US citizen, several years ago I married an Englishman and became a UK resident, entitled to coverage on the British National Health Service. My NHS surgeon was able to schedule me in for the three-hour surgery less than two weeks after my fall, and my physical therapist saw me weekly after the bone was healed to work on my flexion and extension. Both surgery and rehab were free at the point of use, and the only paperwork I completed was my pre-operative release forms.

It’s a mantra from providers to justify the disparate prices charged patients depending on their level of insurance coverage: It’s all in the name of cost shifting to make up for stingy government reimbursement.
The idea is that hospitals bill commercial payers more to make up for low rates from government payers and the costs from treating the uninsured. Providers and payers both insist the practice occurs, but academics are skeptical — and the notion is notoriously difficult to measure.
No one is doubting that the prices are different depending on who is footing the bill. The issue is whether they are dependent on each other.
“What is crystal clear is that there’s a huge unit cost payment differential between government and commercial payers,” John Pickering of Milliman told Healthcare Dive. “What isn’t clear is whether there’s a causal effect between those two.”
Heath economists, doctors and industry executives have been arguing about whether hospitals perform cost shifting for at least 40 years.
Government efforts to tamp down on runaway payments to providers may have sparked the debate. These include Medicare’s shift from strictly fee-for-service reimbursement to the prospective payment system in the 1980s.
Also, the Affordable Care Act attempted to codify efforts to pay providers based on performance with initiatives like the Hospital Readmission Reduction Program and alternative payment models.
Part of the difficulty is untangling factors like differences in geography, quality and market share, said Michael Darden, an associate professor at Carey Business School.
The body of research on healthcare cost shifting is mixed. There is evidence that some hospitals perform cost shifting, but not strong and clear results showing hospitals make such adjustments consistently or what exactly is causing them.
The debate has received some renewed attention as more states approve Medicaid expansion under the ACA and as employers consider offering high-deductible health plans that patients on the hook for more costs, Rick Gundling, senior vice president for healthcare financial practices with the Healthcare Financial Management Association, told Healthcare Dive.
“As folks get more price-sensitive through higher cost-sharing with patients and employers and these types of things — it’s certainly talked about. As it should be,” he said.
The topic may get even more attention as healthcare has come to dominate the early days of the 2020 presidential election, at least among the 20-plus contenders running in the primary.
While still a long way off, a “Medicare for All”-type system seems closer than any time in recent history.
While not all of the proposals explicitly or fully eliminate the private insurance industry, some (including those put forward by Sens. Bernie Sanders, I-Vt., and Elizabeth Warren, D-Mass.,) do, and others would at least severely curtail it. One key question for those plans is whether government rates would have to increase in order to keep hospitals and providers above water, and if so, by how much.
To counter, President Donald Trump and his administration have stepped up their scrutiny of industry billing practices. These efforts include pushing Congress to ban surprise billing and executive orders to revamp kidney care in the country and advance price transparency.
For their part, providers say they’ll be forced to raise other rates if government programs pay less. Insurers will say the phenomenon means they must raise premiums to keep up.
In a statement to Healthcare Dive, America’s Health Insurance Plans pointed the finger at rising hospital prices, spurred in part from provider consolidation. The payer lobby argued health plans do their best to keep out-of-pocket costs affordable for customers through payment negotiations and by offering a number of coverage options.
“However, insurance premiums track directly with the underlying cost of medical care. The rising cost of doctor’s visits, hospital stays, and prescription medications all put upward pressure on premiums,” the group said.
Employers care about this issue as well, especially those that self-insure, said Steve Wojcik, vice president of public policy for the National Business Group on Health. Coverage can get expensive for businesses because they don’t get as good of a deal as government payers, he told Healthcare Dive.
Wojcik suggested more radical change away from fee-for-service payment arranges would be a better way of dealing with the issue. It’s an argument for many who push the healthcare sector’s slow march toward paying for quality and not quantity of treatment.
“I think, ultimately, it’s about driving transformation in healthcare delivery so that there’s more of a global payment for managing someone’s health or the health of a population rather than paying piecemeal for different services, which I think is inflationary,” he said.
Regardless, whether hospitals cost shift isn’t as important as whether they go out of business. “We may be missing the point if we focus on cost shifting,” Christopher Ody, a health economist at Northwestern University’s Kellogg School of Management, told Healthcare Dive.
A paper Darden helped author in the National Bureau of Economic Research found some hospitals that faced payment reductions from value-based Medicare programs did negotiate slightly higher average payments from private payers.
Health economist Austin Frakt noted the ability to negotiate better pricing could be related to quality improvement these hospitals likely undertook, knowing their quality measures would directly affect future payments.
It comes back to determining causality, Frakt, who holds positions with the Department of Veteran’s Affairs, Boston University and Harvard, told Healthcare Dive.
“It’s an important distinction, because the simplest economic model which is consistent with the evidence is that hospitals charge as much as they can to each type of payer,” he said. “So, they can’t really change what they receive from Medicare — those prices are fixed. But they charge private payers whatever the revenue- or profit-maximizing price is.”
Hospitals assert there is causality, but haven’t pointed to evidence that convinced Frakt of their argument. Frakt, for the record, understand why hospitals make the argument to policymakers, however.
“I’m not implying that this, throughout, is just to make a profit,” he said. “I think it’s possible to also have the best interests of patients in mind and to have this argument.”
Grundling said there has to be a breaking point somewhere so long as government rates fail to keep up with medical inflation. Also, hospitals have a federal legal responsibility to stabilize any patient regardless of ability to pay and have other philanthropic investments.
“It just puts a greater pressure on other payers in the system,” he said.
Frakt said the argument providers give for cost shifting doesn’t necessarily make sense for the average consumer. “It’s very strange that people find it intuitive that hospitals can readily cost shift because we don’t talk about any other industry like that,” he said. “Nobody says, well, my theater tickets was so much higher because you paid less.”
The idea that healthcare is vastly different from other industries is enduring, however, he said. “People don’t even want to think of healthcare as having prices,” he said. “How do you put a price on that?”

Insurers in the individual market had asked for 9.2% on average, and DFS trimmed those requests by about one-quarter.
DFS granted Centene’s Fidelis Care, which has the largest market share on the state’s Affordable Care Act marketplace, a 3.9% increase; the insurer had asked for 6.8%.

In the small-group insurance market, insurers were granted an average 7.9% increase in premiums after requesting a 12.2% bump on average.

The percentage increase each New Yorker experiences depends on their insurer, where they live, which product they choose and whether they qualify for income-based subsidies.
The rising premiums reflect increases in the prices of medical care and prescription drugs, said Eric Linzer, president and CEO of the state Health Plan Association.
“Every New Yorker deserves affordable coverage choices that provide them with access to high-quality care,” Linzer said. “Making that a reality requires addressing the underlying factors driving health care costs, particularly the persistent price increases by drug companies and providers.”
The average request of 9.2%, which differs from the 8.4% DFS reported insurers asked for in May, accounts for the inclusion of risk adjustment, a spokeswoman for the department said.
Health Care for All New York, a coalition of patient advocacy groups, said in June that more predictable medical costs in the individual market and excessive increases in past years made insurers’ requests for 2020 unjustified.
The persistent price increases in the individual market, as well as growing out-of-pocket costs for patients, have fueled proponents of a single-payer health system. But the Cuomo administration noted that New Yorkers who don’t get insurance from their employer are still better off than they were before the Affordable Care Act.
The state said that premiums in the individual market are still 55% lower than they were before the implementation of the Affordable Care Act without accounting for income-based tax credits that can lower the cost of insurance.
“This year marks the ninth anniversary of the Affordable Care Act’s passage and the fifth year since implementation, and we continue our strong efforts to support the ACA and combat unjustified federal attacks on the nation’s health care system,” DFS Superintendent Linda Lacewell said in a statement. “By reducing insurers’ rate requests, DFS is ensuring access to affordable health care and helping to maintain a robust, competitive marketplace.”
Elisabeth Benjamin, vice president of health initiatives at the Community Service Society, said state lawmakers must take more aggressive action to make health insurance affordable for New Yorkers. Such action could include price controls, state premium assistance, the creation of a public option or the adoption of a single-payer health system through the New York Health Act, she said.
“I think Superintendent Lacewell and DFS did the best that they could through the administrative tools they have—that is New York’s transparent prior approval process,” Benjamin said. “But at the end of the day, New York needs to do more to address the health care affordability crisis.” —Jonathan LaMantia
As evidence of cannabis’ many benefits mounts, so does the interest from the global pharmaceutical industry, known as Big Pharma. The entrance of such behemoths will radically transform the cannabis industry—once heavily stigmatized, it is now a potentially game-changing source of growth for countless companies.
Today’s infographic comes to us from CB2 Insights, and explores how and why the notorious Big Pharma are interested in the nascent cannabis industry.
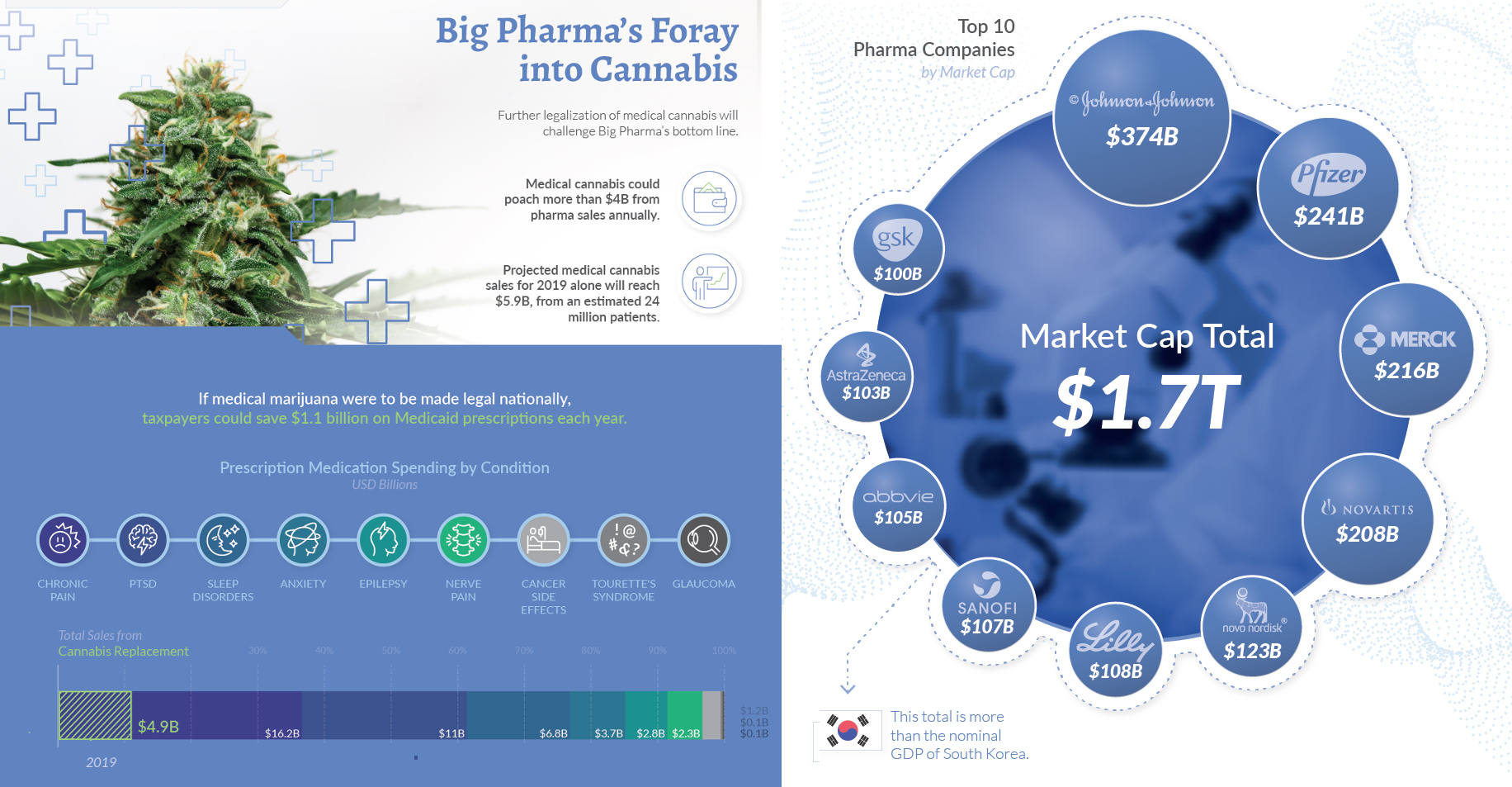
The term refers to some of the largest pharmaceutical companies in the world, considered especially influential as a group. To give a sense of their sheer size, the market cap of the top 10 Big Pharma companies is $1.7 trillion—Johnson & Johnson being the largest, with a market capitalization of $374 billion.
So far, Big Pharma has watched the cannabis industry from the sidelines, deterred by regulatory concerns. What we are seeing now is the sleeping giant’s takeover slowly intensifying as more patents, partnerships, and sponsored clinical trials come to fruition.
The cannabis plant has been used in medicine for 6,000 years. However, there is still considerable debate around the role it plays in healthcare today. There are currently almost 400 active and completed clinical trials worldwide surrounding cannabidiol (CBD), a type of cannabinoid that makes up 40% of the cannabis plant’s extract.
Cannabis relies on CBD’s therapeutic properties, and recent studies suggest it may be useful in combating a variety of health conditions, such as:
As of 2019, 33 states and the District of Columbia have legalized cannabis for medical use. Its potential for pain management has led some experts to recommend it as an alternative to addictive painkillers, with one study of 13 states showing opiate-related deaths decreasing by over 33% in the six years since medical cannabis was legalized.
As the industry evolves, data is becoming increasingly important in understanding the potential of cannabis—both as a viable medical treatment, and as a recreational product. The shift away from anecdotal evidence towards big data will inform future policies, and give rise to a new era of consumer education.
Further legalization of cannabis will challenge Big Pharma’s bottom line, and poach more than $4 billion from pharma sales annually. In fact, medical cannabis sales are projected to reach $5.9 billion in 2019, from an estimated 24 million patients.
Seven of Canada’s top 10 cannabis patent holders are major multinational pharmaceutical companies, a trend that is not unique to Canada.
It comes as no surprise that many pharmaceutical giants have already formed strong partnerships with cannabis companies, such as Novartis and Tilray, who will develop and distribute medical cannabis together in legal jurisdictions around the world.
While the body of knowledge about the many uses of cannabis continue to grow, clinical evidence is key for widespread adoption.
Products backed by data will be a defining criteria for major companies to come into the market en masse. And ultimately, Big Pharma’s entry could accelerate public understanding and confidence in cannabis as a viable option for a range of ailments, and mark the next major milestone for the industry.

The Trump administration wants to drop an Obama-era rule designed to ensure that there are enough doctors to care for Medicaid patients.
State health officials say the rule, which requires states to monitor whether Medicaid reimbursement rates are high enough to keep doctors in the program, forces them to spend a lot of time collecting and analyzing data with little benefit. Health care advocates, though, fear that dropping the regulation would enable states to set those payments at a level that would cause some of the 72 million Americans who rely on Medicaid to scramble for health care. Research shows that when reimbursement rates drop, fewer providers agree to accept low-income Medicaid patients.
Although the Medicaid Access Rule, adopted in 2016, pertains to Medicaid fee-for-service plans, the Trump administration also is seeking to relax requirements on how states determine whether Medicaid managed care organizations have enough providers.
If reimbursement rates are too low, there’s a risk that health care providers would see fewer Medicaid patients or even refuse to treat Medicaid enrollees altogether. That, in turn, could lead to longer wait times to see providers still participating in Medicaid or force patients to travel longer distances to reach providers remaining in the program.
Medicaid, the government health plan for low-income U.S. residents, covers 1 in 5 citizens. It is jointly administered and financed by the federal government and the states.
The rule, the Centers for Medicare and Medicaid Services (CMS) said, “excessively constrains state freedom to administer the program in the manner that is best for the state and Medicaid beneficiaries in the state.”
According to Matt Salo, executive director of the National Association of Medicaid Directors, scrapping it would eliminate a bureaucratic headache for states that, in the end, hasn’t improved patients’ access to providers.
“Nobody is moving the goal of improved access,” Salo said.
Some health care advocates disagree, pointing out that the rule hasn’t been in place very long and that getting rid of it fits the Trump administration’s overall mission of giving states more freedom in operating Medicaid.
“The Trump administration’s approach to Medicaid has been state flexibility, giving states a lot more discretion to do what they want without a lot of attention to what beneficiaries need,” said Abbi Coursolle, a senior attorney with the National Health Law Program, a group based in Washington, D.C., that works to protect access to health care for low-income populations.
CMS last year called for a significant watering down of the Obama rule. Last month, the agency proposed to scrap it altogether. The comment period on elimination of the rule runs through next month, after which CMS will announce its decision.
The initial proposal to weaken the rule generated plenty of opposition. Among those objecting were hospital and physician organizations, groups that advocate for health care access for all, and organizations created to support those living with certain diseases and to raise funds for research into those conditions.
Among the latter was the Epilepsy Foundation, which warned in its public comment that weakening the rule would deprive CMS of information it needed to monitor and enforce Medicaid beneficiaries’ access to care. State reimbursement rates, the foundation said, are crucial to ensuring enough willing providers are available to treat Medicaid beneficiaries.
Shawn Martin, senior vice president of the Academy of Family Physicians, said scrapping the rule would make states more likely to set reimbursement rates too low, prompting practitioners to stop taking Medicaid patients or cut back. “A low reimbursement would affect how many beneficiaries providers are willing to see.”
Just as adamant on the other side, however, are many states that complain that the Obama rule is cumbersome and ineffective at ensuring access for Medicaid beneficiaries.
At the Maryland Department of Health, Tricia Roddy, a research director, said the rule doesn’t do much to help gauge the fees’ effects on access to care.
Similarly, at the Colorado Department of Health Care Policy and Financing, Marc Williams, a spokesman, said his state uses other strategies to ensure Medicaid beneficiaries’ access to the health services they need.
According to Salo of the Medicaid directors group, states of both political stripes, red and blue, are delighted that the Trump administration is moving to abolish the rule.
“It was creating many bureaucratic burdens without accomplishing anything concrete,” Salo said. The rule, he said, “is insanely micro-managed and overly bureaucratic.”
The 1965 law establishing Medicaid has been amended through the years to ensure that enough doctors, nurses and other providers are available to serve beneficiaries. Congress in 1989 passed an amendment making clear states’ obligation to pay providers enough to ensure Medicaid enrollees have access to care.
Medicaid pays doctors about three-fourths as much as Medicare, the government program for senior citizens, according to a 2017 analysis by the Urban Institute, a nonpartisan think tank in Washington, D.C. And Medicare pays much less than private insurers.
When Medicaid and Medicare payments, or reimbursement rates, go down, research shows that patients make fewer doctor’s visits and more trips to the emergency room.
According to a 2017 Kaiser Family Foundation report, only about 70% of office-based physicians accept new Medicaid patients. The results vary from 39% in New Jersey to 97% in Nebraska. By comparison, the study found, 85% of doctors accept new patients with private insurance.
The 2016 rule required states to tell the agency every three years how providers from various geographic regions and specialties were participating in Medicaid, and how reimbursement rates were affecting that participation.

Average total cash compensation for health system executives rose 6.5% from 2018 to 2019, extending a consistent rise in executive pay that governance experts do not expect to slow.
Annual and long-term performance-based incentives have driven pay hikes of 4% to 7% each of the last four years, according to Modern Healthcare’s annual Executive Compensation Survey. Health systems’ ongoing expansions coupled with a highly competitive executive market will continue to drive up their base salaries and bonuses, experts said. But this dynamic is drawing ire from rank-and-file employees who aren’t happy with their pay and from consumers who are spending more on their care. It is also spurring new legislation.
Nevertheless, with baby boomers retiring in large numbers and demand soaring, the pay hikes aren’t going away anytime soon. “Healthcare organizations are becoming more complex and leadership skills are evolving,” which often translates to higher pay, said Bruce Greenblatt, a managing principal at SullivanCotter, the compensation consulting firm that has supplied data for Modern Healthcare’s annual surveys since 2003.
Providers look to select metrics and targets that will shape their organization for years to come. In doing so, they toe a delicate line ensuring their bonuses are attainable to keep executives engaged while not making them out of reach and damaging morale.
With more pay based on performance, there’s greater risk of poor program design, said Steve Sullivan, a managing director at executive compensation consulting firm Pearl Meyer. If you make a mistake, there is a lot of money on the line, he said.
“You don’t want to have giveaways and you don’t want to have plans so egregiously hard that they never have payouts because executives will disengage from the program,” Sullivan said. “You have to strike a balance between responsible compensation and something that is motivating and incenting.”
Health system executives’ average base salaries increased 4.2% and ticked up even higher among organizations with more than $3 billion in revenue based in high-cost cities, according to Modern Healthcare’s 39th Executive Compensation Survey, made up of data aggregated from 1,149 hospitals and 401 health systems. System CEOs earned an average total cash compensation of $1.4 million in 2019, a 6.3% increase.
Executives who saw the highest total cash compensation hikes of 6.6% up to 13.3% were business development officers, administrative officers, internal audit executives, chief financial officers, planning executives, reimbursement executives, chief nursing officers, chief human resources officers and chief operating officers.
Incentives are typically tiered with a minimum threshold, a target and a stretch goal. They are often based on quality, safety and patient experience as well as financial performance. They may be related to ambulatory market share, employee and patient engagement, facilitating access to capital, bolstering physician alignment, inking successful joint partnerships and mergers, emergency department wait times and utilization, population health, shared risk, readmissions, hospital-acquired infections and length of stay, among other metrics.
The types of incentives offered are heavily dependent on the provider and the market. Some hospitals and health systems have stuck to the more traditional financial and market-share-based measurements, while more progressive organizations are targeting outcomes.
The bonuses differ based on short- and long-term goals, the latter becoming more prominent in recent years as boards and compensation committees emphasize the entire organization’s performance. Sometimes there is a trigger, such as operating margin, where executives miss out on all bonuses if it isn’t reached. For instance, Mercy Health, which is now Bon Secours Mercy Health, did not pay executives an incentive in 2016 since the system did not reach its incentive thresholds, the Cincinnati-based Catholic health system said.
“You want to make sure everyone is rolling in the right direction,” said Tom Giella, chairman of healthcare services for executive recruiter Korn Ferry. “You want to do what is right for the system, not an individual hospital or inpatient versus outpatient. It creates an incentive for everyone to work together.”
But even if the baseline isn’t reached, there typically isn’t a penalty, experts said. It will only lower their earning potential. “In some industries there can be a negative adjustment,” Sullivan said. “I haven’t seen that in healthcare. In healthcare, if there is a modifier it is going to be positive.”
Nearly half of larger health systems surveyed report using long-term incentive plans.
Dignity Health said a “substantial portion” of executive compensation is linked to organizational performance related to key clinical-quality and patient-satisfaction measures as well as community health investments and financial performance. Similarly, Kaiser Permanente said a third to half of pay is based on performance, linked to membership growth, expenses, operating income, and clinical and service quality improvements. Bon Secours Mercy said each of its employees are rewarded under the same incentive program, which includes quality, growth, financial and community benefit targets.
More providers are using deferred compensation programs, which can amount to hefty payouts at the end of an executive’s tenure.
In a related Modern Healthcare analysis of more than 2,000 not-for-profit hospitals, the 25 highest-paid not-for-profit health system executives received a combined 33.2% increase in total compensation in 2017, as their compensation rose to $197.9 million from $148.6 million in 2016.
The pay increases have spawned rallies and protests from more than 1,000 employees at Beaumont Health and Providence St. Joseph Health, both of which had chief executives in the top 25. Beaumont and Providence said in prepared statements that their CEO pay are not outliers compared to their peers.
California policymakers introduced a bill, recently passed by a state Senate subcommittee, that aims to boost not-for-profit health systems’ public disclosure requirements for executives’ deferred compensation.
“What surprises people I think as compensation becomes very generous because it is a competitive market, some think a hospital administrator shouldn’t expect to make more than the average physician,” said Paul Keckley, an industry consultant and managing editor of the Keckley Report. “Those days are long gone.”
Executives’ pay along with their respective C-suites are growing as health systems expand. New C-suite positions in 2019 included reimbursement executive, communications executive, academic affairs executive and operations executive, according to SullivanCotter’s data.
Physician leaders continue to be in high demand as providers look to influence clinical delivery redesign, population heath activities and quality improvement, said Tom Pavlik, a managing principal at SullivanCotter. Administrative roles in finance, consumer experience, IT, marketing and human resources are being filled by healthcare industry outsiders, he said.
“There is a lot of change as organizations are realigning to be operationally efficient and integrate clinical care delivery,” Pavlik said.
Among hospital executives, average base salaries rose 3.7% for hospitals that exceeded $300 million in revenue compared to 3.2% for smaller facilities. System-owned hospitals saw slightly lower base salary hikes than independent ones.
Average total compensation increased 5.3%, while CEOs of independent hospitals took home the highest raises at 9.2%, followed by chief financial officers of independent hospitals (6.5%), chief operating officers of system-owned hospitals (5.8%) and chief financial officers of system-owned hospitals (5.3%). Independent hospital CEOs earned an average of $758,300.
Providers rely on third-party consultants for accurate portrayals of market-based compensation reports that inform their compensation structures. But some of Pearl Meyer’s prospective clients are concerned about how their current adviser is interpreting the market, Sullivan said.
“With all the M&A, you have to create larger peer groups to generate a bigger sample,” he said.
This is a relatively new dynamic as the number of megasystems have swelled, Giella said.
“There is a war for talent and a big demand as systems have amalgamated so quickly,” he said. “They are getting through these growing pains where they have never dealt with this scale before, so it’s hard to look at historical trends. It’s very fluid so it’s hard to tell if you are paying someone fair compensation.”
One of Keckley’s regional health system clients told him that they are trying to figure out the most efficient and lean model.
“When I asked him what is keeping him awake, he said, ‘I want to be sure we are market-focused and that we are not just busy moving the deck chairs around.’ ”
DATA: Executive Compensation: 2019

Opponents of the public option have funded an analysis that warns more rural hospitals may close if Americans leave commercial plans for Medicare.
With the focus on rural hospitals, the Partnership for America’s Health Care Future brings a sensitive issue for politicians into its fight against a Medicare buy-in. The policy has gone mainstream among Democratic presidential candidates and many Democratic lawmakers.
The estimate assumed Medicaid wouldn’t lose anyone to Medicare, and plotted out various scenarios where up to half of the commercial market would shift to Medicare.
The analysis was commissioned by the Partnership for America’s Health Care Future, a coalition of hospitals, insurers and pharmaceutical companies fighting public option and single-payer proposals.
In their most drastic scenario of commercial insurance losses, co-authors Jeff Goldsmith and Jeff Leibach predict more than 55% of rural hospitals could risk closure, up from 21% who risk closure today according to their previous studies.
Leibach said the analysis was tailored to individual hospitals, accounting for hospitals that wouldn’t see cuts since they don’t have many commercially insured patients.
The spotlight on rural hospitals in the debate on who should pay for healthcare is common these days, particularly as politicians or the executive branch eye policies that could cut hospital or physician pay.
On Wednesday, Sen. Elizabeth Warren (D-Mass.) seemingly acknowledged this when she published her own proposal to raise Medicare rates for rural hospitals as part of her goal to implement single payer, or Medicare for All. She is running for the Democratic nomination for president for the 2020 election.
“Medicare already has special designations available to rural hospitals, but they must be updated to match the reality of rural areas,” Warren said in a post announcing a rural strategy as part of her campaign platform. “I will create a new designation that reimburses rural hospitals at a higher rate, relieves distance requirements and offers flexibility of services by assessing the needs of their communities.”
Warren is a co-sponsor of the Medicare for All legislation by Sen. Bernie Sanders (I-Vt.), who is credited with the party’s leftward shift on the healthcare coverage question. But she is trying to differentiate herself from Sanders, and the criticisms about the potentially drastic pay cuts to hospitals have dogged single-payer debates.
Most experts acknowledge the need for a significant policy overhaul that lets rural hospitals adjust their business models. Those providers tend to have aging and sick patients; high rates of uninsured and public pay patients over those covered by commercial insurance; and fewer patients overall than their urban counterparts.
But lawmakers in Washington aren’t likely to act during this Congress. The major recent changes have mostly been driven by the Trump administration, where officials just last week finalized an overhaul of the Medicare wage index to help rural hospitals.
As political rhetoric around the public option or single payer has gone mainstream this presidential primary season, rural hospitals will likely remain a talking point in the ideas to overhaul or reorganize the U.S.’s $3.3 trillion healthcare industry.
This was in evidence in May, when the House Budget Committee convened a hearing on Medicare for All to investigate some of the fiscal impacts. One Congressional Budget Office official said rural hospitals with mostly Medicaid, Medicare and uninsured patients could actually see a boost in a redistribution of doctor and hospital pay.
But the CBO didn’t analyze specific legislation and offered a vague overview of how a single-payer system might look, rather than giving exact numbers.
The plight of rural hospitals has been used in lobbying tactics throughout this year — in Congress’ fight over how to end surprise medical bills as well as opposition to hospital contracting reforms proposed in the Senate.
And it has worked to some extent. Both House and Senate committees have made concessions to their surprise billing proposals to mollify some lawmakers’ worries.

The ranking member of the Senate health committee has complained for months about the Trump administration’s failure to look into Medicaid contractors that have reaped big profits while sometimes failing to provide crucial patient services.
So last week, Sen. Bob Casey, D-Pa., called in the top boss of Centene, the nation’s largest Medicaid managed care company. He wanted to question the company about reports that its Texas subsidiary denied life-sustaining care to sick and disabled children — in one case, leaving a baby in foster care to suffer a catastrophic brain injury.
The meeting with longtime Centene CEO Michael Neidorff did not go well, according to Casey.
“I thought they would try to persuade me that they were going to do better, but they didn’t seem interested in that at all,” Casey told ProPublica and The Dallas Morning News in an interview. “I just couldn’t believe it.”
Casey said the Centene official denied providing inadequate care and cast blame for failures on foster parents and nurses.
Centene declined to make Neidorff available for an interview and emailed a brief statement in response to questions about the meeting with Casey.
“Centene and its subsidiaries care deeply about each and every member we serve,” the email read. “We work tirelessly to ensure we provide the appropriate level of care for our members.”
Under Neidorff, Centene has grown from a tiny health network in the Midwest into a $60-billion-a-year health care empire, backed almost entirely with taxpayer money. The company cares for more than 8.5 million Medicaid patients.
The company came under criticism last year after an eight-part investigation published in the Morning News examined whether Centene and other Medicaid managed care companies were skimping on care to bolster profits. The series raised questions about Centene’s Texas subsidiary, Superior HealthPlan, and its handling of the case of D’ashon Morris, a Texas toddler who was born with severe defects and was living in a foster home.
The series, titled “Pain & Profit,” reported that D’ashon was denied 24/7 nursing care and suffered brain damage after a medical incident that occurred while he did not have his nurse around. (Read the full story here.)
The Morning News reported that state health officials had found the Centene subsidiary in violation of state and federal Medicaid rules and recommended the company face steep fines for what happened to the child. But top Texas health officials never assessed those fines, the Morning News reported.
D’ashon’s adoptive mother sued the Centene subsidiary in Texas state court. That case is tied up in the Texas appeals court, where the Centene subsidiary has argued that the lawsuit should be dismissed because D’ashon and his mother are stifling the company’s right to free speech.
During hearings in the state Capitol, Superior representatives denied that the company’s refusal to provide 24/7 nursing was improper.
After his meeting with the Centene official, Casey sent a strongly worded letter to Seema Verma, a former health consultant appointed by President Donald Trump to run the Centers for Medicare and Medicaid Services.
In the letter, Casey called Centene’s response to questions about D’ashon’s case “callous.”
He also asked Medicaid officials to dig further into Centene’s business practices and to provide documentation on any response to the Morning News investigation.
“It’s another indication that the regulatory approach here by the administration is, at best, suspect,” Casey said.
A CMS spokesman said that Texas officials have shared with the agency an “action plan they intended to take to address the concerns raised,” adding that CMS is in regular communication to ensure the state improves.
“CMS has received Sen. Casey’s letter and will respond to his office directly,” spokesman Brian Leshak said in an email.
Casey’s position as the top Democrat on two Senate panels overseeing federal health programs gives him the standing to raise questions about the Medicaid managed care system.
It’s not unusual for company officials facing a federal audit or investigation to meet with members of Congress to address concerns, but it is unusual for such meetings to spill into public view.
Casey said he sent the letter to CMS because of what he called Centene’s “cold and clinical” defense of what happened in D’ashon’s case. He said it gave him concern about how the company cares for other patients — and what, if anything, regulators are doing when things go wrong.
Last month, more than a year after the Morning News story was published, Centene officials provided Casey’s office with a one-page rebuttal titled: “The Dallas Morning News got it wrong.”
The company’s explanations include that D’ashon’s foster mother was a trained nurse. But, as the Morning News reported, she was on an approved vacation at the time of D’ashon’s injury, and he had been placed in a different foster home.
The company also said D’ashon’s foster mother should have restrained the baby, but the Morning News previously reported that Texas foster care officials confirmed restraints would have required a doctor’s order, which she did not have.
“It was all blame shifting and pointing to other factors,” Casey said of Centene’s letter.
Casey said the meeting left him wondering why federal regulators weren’t doing more.
“It might even be worse than asleep at the wheel,” he said of CMS under Verma’s watch.
“They may be awake at the wheel but choosing consciously to say, ‘We’re going the other direction.’”
Without commenting on specific cases, the CMS spokesman said the agency routinely monitors states and intervenes when necessary.
Problems with this privatized Medicaid model have grabbed headlines in other states, too. And advocates in those states said they haven’t heard much from CMS, which they say is a shift from the Obama administration.
In Iowa, for instance, The Des Moines Register reported failures to provide care and chronicled patients who had been caught in that state’s broken medical appeals system.
Rob Sand, Iowa’s state auditor, wrote to state officials in June that two large managed care companies had “significantly harmed” two paraplegic patients by refusing to provide services they needed.
Mary Nelle Trefz, of Iowa’s Child and Family Policy Center, said she’s been shocked to hear nothing about that from CMS.
“I don’t feel, or can’t observe, or point to anything, where CMS has stepped in to provide that oversight and accountability,” she said.
In March, California’s state auditor found that millions of children in that state’s privatized Medicaid system weren’t being provided services that taxpayers had paid for. Auditor Elaine Howle blamed California health officials’ “deficient oversight of the managed care plans.”
Andy Schneider, a researcher at Georgetown’s Center for Children and Families, and a former top adviser to CMS under the Obama administration, said these episodes come at an inconvenient time for the Trump administration, which is focused on reducing regulation and creating additional eligibility hurdles like work requirements.
CMS has taken a hands-off approach compared with the previous administration, he said.
“These are reports coming from reputable media sources,” he said. “They’re very concerning, they have to do with the operation of the program, they suggest that something is wrong.”
