Hospitals in the Dallas-Fort Worth region could collectively lose $1.1 billion in funding each year without a Medicaid waiver extension, a healthcare group warned, according to CBS Local.
The group, Texas Essential Healthcare Partnerships, represents 72 hospitals in the Dallas-Fort Worth region, including those operated by Dallas-based Tenet Healthcare and Houston-based Baylor Scott & White Health.
In April, CMS rescinded approval for a Section 1115 waiver to extend reimbursement to Texas hospitals for uncompensated care through September 2030. President Joe Biden’s CMS said that under the previous administration, CMS and Texas failed to adhere to public comment period requirements in the approval process, so it should be rescinded.
Don Lee, Texas Essential Healthcare Partnerships, told CBS he’s concerned about CMS’ decision to rescind the waiver next year and that hospitals could begin feeling the effects in just three months.
“There’s about $330 million of very important mental healthcare funding for mental healthcare services for the poor that will be lost starting in September of this year,” Mr. Lee told CBS Local.
Texas plans to resubmit its application to extend the 1115 waiver soon, according to the report. However, if the new application is not approved, Mr. Lee said that some hospitals in the North Texas region may be forced to close.
“We believe it’d be catastrophic, not just for the hospitals, but for all Texans,” Mr. Lee told CBS Local.
Administrative costs in the US healthcare system are known to be higher than those in any other country, even than other countries with private health insurance systems. There also is widespread agreement the excessive US costs generate little, if any, value, and that they impose a tremendous burden on physicians. With administrative costs even for primary care services approaching $100,000 per year per physician, there is a growing recognition that reducing healthcare-related administrative costs is a policy priority.
Despite the longstanding concerns about these escalating costs, there is little understanding of what generates them and how we can reduce them. To the degree there has been any academic inquiry into administrative costs imposed on US providers, it has compared them to the much lower costs in other countries with nationalized systems. These comparisons are unflattering to the US system and are designed to encourage wholesale healthcare reform.
Our paper published in Health Services Research begins at the retail level, focusing on the specific administrative costs inflicted by our payment system on providers. We examine the complex contractual arrangements between insurers and physicians and measure the efforts that physicians must endure to get paid. It then offers a simulation model to estimate how certain policy reforms would result in nationwide administrative savings.
Currently, each health plan and each physician or physician group (and each hospital) negotiates over a contract for services on a periodic basis. Our analysis examines three separate costs that result from this type of market structure: architectural costs (the enormous number of contracts that are generated annually to provide services to patients), contractual complexity (the difficulty of following all of the requirements of each agreement to receive payment), and compliance costs (the costs of not following the rules in submitting a bill).
Based on this framework, we ask two questions: First, what if physicians entered into simpler contracts with insurers? And second, what if physicians (who accept patients with many kinds of insurance) agreed to a single boilerplate contract with all insurers rather than individualized contracts with each insurer? Put more simply, what if contracts were simpler and standardized?
Our simulation predicts that simplifying contracts would reduce billing costs by nearly 50%, standardizing contracts would reduce those costs by about 30%, and both simplifying and standardizing contracts would reduce those costs by over 60% percent.
We then used the model to estimate administrative cost savings from a single payer “Medicare-for-All” model. Consistent with claims made by advocates for nationalized health insurance, we estimate that a Medicare-for-All plan would reduce administrative costs between 33-53%, largely by standardizing contracts. But these cost savings are less than those generated from standardizing and simplifying contracts within our current system of private health insurance because we modeled that a Medicare-For-All plan would retain Medicare’s complex payment models and have increased compliance costs compared to private payers.
We think this is good news. Though we find that a single-payer system will reduce certain administrative costs, we also find that reforms to our current multi-payer system could generate at least as great a reduction.
There might be benefits to pursuing national health reform, but we can reduce burdensome administrative costs through much simple and less disruptive paths. The even better news from this study is that we can now have a more precise understanding of where administrative costs arise in our health system, and we have the means to evaluate the effects of other kinds of reforms. Understanding is the prerequisite to reforming.
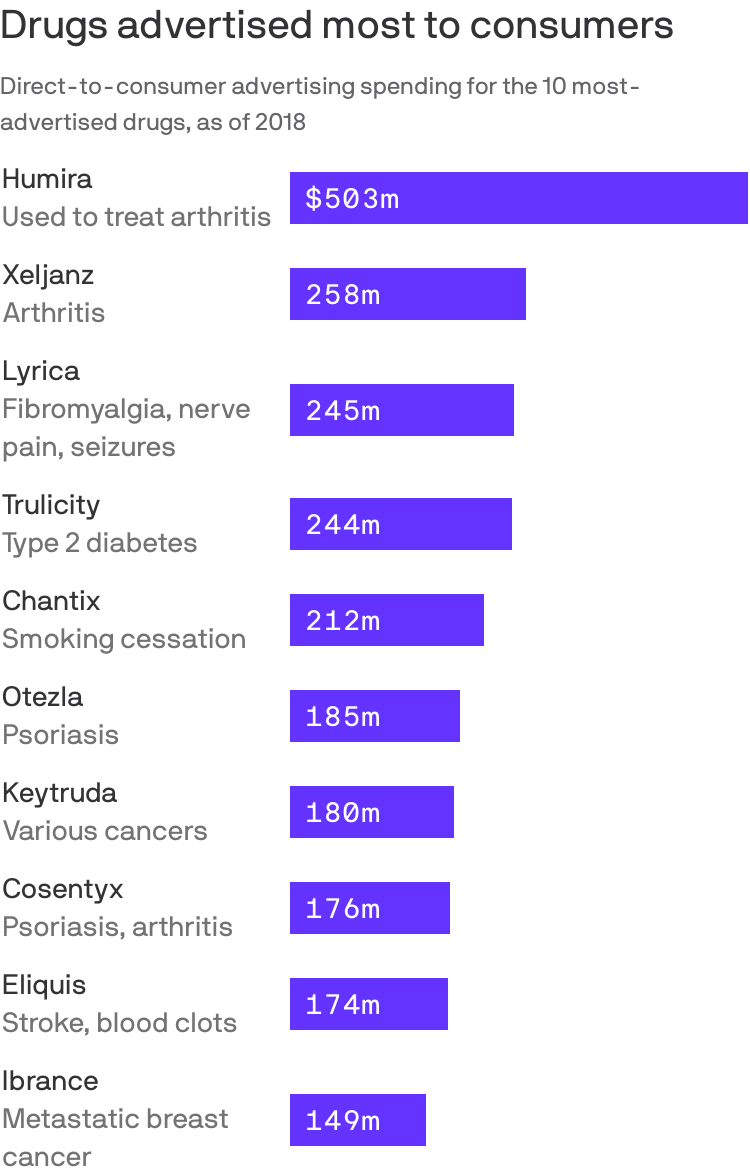
Prescription drugs with some of the highest Medicare spending also had the highest level of direct-to-consumer advertising, a recently-released GAO report found.
By the numbers:The GAO found the Medicare program and its beneficiaries spent nearly $324 billion on prescription drugs advertised to beneficiaries and other consumers between 2016 and 2018.
This amount is more than half(58%) of total Medicare Parts B and D spending on drugs during that time, the most recent data available.
Seven of the top 25 drugs in Part D and two of the top 25 drugs in Part B with the highest spending were also among the top 25 drugs with the highest consumer advertising spending that year.
For example, Trulicity, as well as Lyrica, Eliquis and Humira were among the top 25 drugs in Part D and direct-to-consumer advertising spending.
Keytruda and Botox were among the top 24 drugs in Part B and direct-to-consumer advertising spending.
With a $56,000-a-year price tag, Biogen’s newly approved Alzheimer’s drug Aduhelm is dovetailing into the debate on Capitol Hill over how to lower prescription drug prices.
Why it matters:Democrats may be positioning themselves to push policy measures that assign value to drugs and then price them accordingly — a huge potential blow to the pharmaceutical industry.
To truly address its launch price, policymakers have to grapple with big questions the U.S. system currently avoids: How should we determine the value of a drug, and who gets to make that decision?
President Biden proposed giving an independent review board the power to determine the Medicare rate for new drugs that don’t have any competition.
Democrats’ most prominent drug legislation is a House bill that gives Medicare the power to negotiate drug prices.
Sen. Ron Wyden, the chairman of the Senate Finance Committee, recently called out Aduhelm by name in a document outlining the principles that will guide the Senate’s drug pricing bill, a hint that the Senate’s legislation will take a different direction than the House’s.
The bottom line:“Any kind of process for valuing new drugs like Aduhelm take you immediately into the controversial quagmire of how to quantify improvements in quality of life for people,” said KFF’s Larry Levitt.
It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,”AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
The Biden administration is quietly engineering a series of expansions to Medicaid that may bolster protections for millions of low-income Americans and bring more people into the program.
Biden’s efforts — which have been largely overshadowed by other economic and health initiatives — represent an abrupt reversal of the Trump administration’s moves to scale back the safety-net program.
The changes could further boost Medicaid enrollment — which the pandemic has already pushed to a record 80.5 million. Some of the expansion is funded by the COVID-19 relief bill that passed in March, including coverage for new mothers.
Others who could also gain coverage under Biden are inmates and undocumented immigrants. At the same time, the administration is opening the door to new Medicaid-funded services such as food and housing that the government insurance plan hasn’t traditionally offered.
“There is a paradigm change underway,” said Jennifer Langer Jacobs, Medicaid director in New Jersey, one of a growing number of states trying to expand home-based Medicaid services to keep enrollees out of nursing homes and other institutions.
“We’ve had discussions at the federal level in the last 90 days that are completely different from where we’ve ever been before,” Langer Jacobs said.
Taken together, the Medicaid moves represent some of the most substantive shifts in federal health policy undertaken by the new administration.
“They are taking very bold action,” said Rutgers University political scientist Frank Thompson, an expert on Medicaid history, noting in particular the administration’s swift reversal of Trump policies. “There really isn’t a precedent.”
The Biden administration seems unlikely to achieve what remains the holy grail for Medicaid advocates: getting 12 holdout states, including Texas and Florida, to expand Medicaid coverage to low-income working-age adults through the Affordable Care Act.
And while some of the recent expansions – including for new mothers — were funded by close to $20 billion in new Medicaid funding in the COVID relief bill Biden signed in March, much of that new money will stop in a few years unless Congress appropriates additional money.
The White House strategy has risks. Medicaid, which swelled after enactment of the 2010 health law, has expanded further during the economic downturn caused by the pandemic, pushing enrollment to a record 80.5 million, including those served by the related Children’s Health Insurance Program. That’s up from 70 million before the COVID crisis began.
The programs now cost taxpayers more than $600 billion a year. And although the federal government will cover most of the cost of the Biden-backed expansions, surging Medicaid spending is a growing burden on state budgets.
The costs of expansion are a frequent target of conservative critics, including Trump officials like Seema Verma, the former administrator of the Centers for Medicare & Medicaid Services, who frequently argued for enrollment restrictions and derided Medicaid as low-quality coverage.
But even less partisan experts warn that Medicaid, which was created to provide medical care to low-income Americans, can’t make up for all the inadequacies in government housing, food and education programs.
“Focusing on the social drivers of health … is critically important in improving the health and well-being of Medicaid beneficiaries. But that doesn’t mean that Medicaid can or should be responsible for paying for all of those services,” said Matt Salo, head of the National Association of Medicaid Directors, noting that the program’s financing “is simply not capable of sustaining those investments.”
Restoring federal support
However, after four years of Trump administration efforts to scale back coverage, Biden and his appointees appear intent on not only restoring federal support for Medicaid, but also boosting the program’s reach.
“I think what we learned during the repeal-and-replace debate is just how much people in this country care about the Medicaid program and how it’s a lifeline to millions,” Biden’s new Medicare and Medicaid administrator, Chiquita Brooks-LaSure, told KHN, calling the program a “backbone to our country.“
The Biden administration has already withdrawn permission the Trump administration had granted Arkansas and New Hampshire to place work requirements on some Medicaid enrollees.
In April, Biden blocked a multibillion-dollar Trump administration initiative to prop up Texas hospitals that care for uninsured patients, a policy that many critics said effectively discouraged Texas from expanding Medicaid coverage through the Affordable Care Act, often called Obamacare. Texas has the highest uninsured rate in the nation.
The moves have drawn criticism from Republicans, some of whom accuse the new administration of trampling states’ rights to run their Medicaid programs as they choose.
“Biden is reasserting a larger federal role and not deferring to states,” said Josh Archambault, a senior fellow at the conservative Foundation for Government Accountability.
But Biden’s early initiatives have been widely hailed by patient advocates, public health experts and state officials in many blue states.
“It’s a breath of fresh air,” said Kim Bimestefer, head of Colorado’s Department of Health Care Policy and Financing.
Chuck Ingoglia, head of the National Council for Mental Wellbeing, said: “To be in an environment where people are talking about expanding health care access has made an enormous difference.”
Mounting evidence shows that expanded Medicaid coverage improves enrollees’ health, as surveys and mortality data in recent years have identified greater health improvements in states that expanded Medicaid through the 2010 health law versus states that did not.
Broadening eligibility
In addition to removing Medicaid restrictions imposed by Trump administration officials, the Biden administration has backed a series of expansions to broaden eligibility and add services enrollees can receive.
Biden supported a provision in the COVID relief bill that gives states the option to extend Medicaid to new mothers for up to a year after they give birth. Many experts say such coverage could help reduce the U.S. maternal mortality rate, which is far higher than rates in other wealthy nations.
Several states, including Illinois and New Jersey, had sought permission from the Trump administration for such expanded coverage, but their requests languished.
The COVID relief bill — which passed without Republican support — also provides additional Medicaid money to states to set up mobile crisis services for people facing mental health or substance use emergencies, further broadening Medicaid’s reach.
And states will get billions more to expand so-called home and community-based services such as help with cooking, bathing and other basic activities that can prevent Medicaid enrollees from having to be admitted to expensive nursing homes or other institutions.
Perhaps the most far-reaching Medicaid expansions being considered by the Biden administration would push the government health plan into covering services not traditionally considered health care, such as housing.
This reflects an emerging consensus among health policy experts that investments in some non-medical services can ultimately save Medicaid money by keeping patients out of the hospital.
In recent years, Medicaid officials in red and blue states — including Arizona, California, Illinois, Maryland and Washington — have begun exploring ways to provide rental assistance to select Medicaid enrollees to prevent medical complications linked to homelessness.
The Trump administration took steps to support similar efforts, clearing Medicare Advantage health plans to offer some enrollees non-medical benefits such as food, housing aid and assistance with utilities.
But state officials across the country said the new administration has signaled more support for both expanding current home-based services and adding new ones.
That has made a big difference, said Kate McEvoy, who directs Connecticut’s Medicaid program. “There was a lot of discussion in the Trump administration,” she said, “but not the capital to do it.”
Other states are looking to the new administration to back efforts to expand Medicaid to inmates with mental health conditions and drug addiction so they can connect more easily to treatment once released.
Kentucky health secretary Eric Friedlander said he is hopeful federal officials will sign off on his state’s initiative.
Still other states, such as California, say they are getting a more receptive audience in Washington for proposals to expand coverage to immigrants who are in the country without authorization, a step public health experts say can help improve community health and slow the spread of communicable diseases.
“Covering all Californians is critical to our mission,” said Jacey Cooper, director of California’s Medicaid program, known as Medi-Cal. “We really feel like the new administration is helping us ensure that everyone has access.”
The Trump administration moved to restrict even authorized immigrants’ access to the health care safety net, including the “public charge” rule that allowed immigration authorities to deny green cards to applicants if they used public programs such as Medicaid.In March, Biden abandoned that rule.
We rarely see the impact of policies reflected in data in real time. The COVID-19 pandemic changed that. In the present moment, a range of government, private, and academic sources catalogue household-level health and economic information to enable rapid policy analysis and response. To continue promoting periodic findings, identifying vulnerable populations, and maintaining a focus on public health, frequent national data collection needs to be improved and expanded permanently.
Knowledge accumulates over time, facilitating new advancements and advocacy. While mRNA biotechnology was not usable decades ago, years of public research helped unlock highly effective COVID-19 vaccines. The same can be true for advancing effective socioeconomic policies. More national, standardized data like the Census Bureau’s Household Pulse Survey will accelerate progress. At the same time, there are significant issues with national data sources. For instance, COVID-19 data reported by the CDC faced notable quality issues and inconsistencies between states.
Policymakers can’t address problems that they don’t know exist. Researchers can’t identify problems and solutions without adequate data. We can better study how policies impact population health and inform legislative action with greater federal funding dedicated to wide-ranging, systematized population surveys.
Broader data collection enables more findings and policy development
Evidence-based research is at the core of effective policy action. Surveillance data indicates what problems families face, who is most affected, and which interventions can best promote health and economic well-being. These collections can inform policy responses by reporting information on the demographics disproportionately affected by socioeconomic disruptions. Race and ethnicity, age, gender, sexual orientation, household composition, and work occupation all provide valuable details on who has been left behind by past and present legislative choices.
Since March 2020, COVID-19 cases and deaths, changes in employment, and food and housing security have been tracked periodically with detailed demographic information through surveys like the Both cumulative statistical compilations and representative surveillance polling have been instrumental to analyses. Our team has recorded over 200 state-level policies in the COVID-19 US State Policy (CUSP) database to further research and journalistic investigations. We have learned a number of policy lessons, from the health protections of eviction moratoria to the food security benefits of social insurance expansions. Not to be forgotten is the importance of documented evidence to these insights.
Without this comprehensive tracking, it would be difficult to determine the number of evictions occurring despite active moratoria, what factors contribute to elevated risk of COVID-19, and the value of pandemic unemployment insurance programs in states. The wider number of direct and indirect health outcomes measured have bolstered our understanding of the suffering experienced by different demographic groups. These issues are receiving legislative attention, in no small part due to the broad statistical collection and subsequent analytical research on these topics.
Insufficient data results in inadequate understanding of policy issues
The more high-quality data there is, the better. With the state-level policies present in CUSP, our team and other research groups quantified the impact of larger unemployment insurance benefit sizes, greater minimum wages, mask mandates, and eviction freezes. These analyses have been utilized by state and federal officials. None would have been possible without increased data collection.
However, our policy investigations are constrained by the data availability and quality on state and federal government websites, which may be improved with stimulus funds allocated to modernize our public health data infrastructure. Some of the most consequential decision-making right now relates to vaccine distribution and administration, but it is difficult to disaggregate state-level statistics. Many states lack demographic information on vaccine recipients as well as those that have contracted or died from COVID-19. Even though racial disparities are present in COVID-19 cases, hospitalizations, and deaths nationally, we can’t always determine the extent of these inequities locally. These present issues are a microcosm of pre-existing problems.
Data shortcomings present for years, in areas like occupational safety, are finally being spotlighted due to the pandemic. Minimal national and state workplace health data translated to insufficient COVID-19 surveillance in workplace settings. Studies that show essential workers are facing elevated risk of COVID-19 are often limited in scope to individual states or cities, largely due to the lack of usable and accessible data. More investment is needed going forward beyond the pandemic to better document a Otherwise there will continue to be serious blind spots in the ability to evaluate policy decisions, enforce better workplace standards, and hold leaders accountable for choices.
These are problems with a simple solution: collect more information. Now is not the time to eliminate valuable community surveys and aggregate compilations, but to expand on them. More comprehensive data will provide a spotlight on current and future legislative choices and improve the understanding of policies in new ways. It is our hope that are built upon and become the new norm.
Disclosure: Funding received from Robert Wood Johnson Foundation was used to develop the COVID-19 US State Policy Database.
During Pride Month we feel it’s especially important to shine a light on the significant health disparities faced by transgender and gender-nonconforming individuals.
Transgender healthcare has been under growing attack in recent months; while the Biden administration formally reinstated Affordable Care Act protections for transgender Americans against discrimination in healthcare, 20 states have introduced anti-trans bills since the start of the year, most featuring provisions that bar physicians from providing trans children with gender-affirming care.
The graphic above shows that transgender individuals are twice as likely as the broader LGBTQ+ population to delay care for fear of discrimination. Trans individuals deal with myriad types of medical discrimination, from being misgendered in routine interactions to being denied treatment. And trans people of color report experiencing this mistreatment even more frequently. Transgender people are also more likely to be uninsured or to delay care for financial reasons, in part because their unemployment and uninsured rates are higher than the national average. Even when they do find supportive providers, nearly 40 percent report that their insurance will not cover essential elements of transitional care, such as hormone therapy.
It’s incumbent on doctors and health systems to strengthen their policies for treating trans individuals. Trans-specific training for clinicians and staff is a great place to start. Even simple shifts in operations—like including preferred name and pronouns on patient records and providing equal access to public restrooms—are small but important steps to providing a safer, more inclusive healthcare experience and reducing transgender health disparities.