While many hospitals face financial hardships and rising expenses from the COVID-19 pandemic, several large health systems ended 2021 with profits above $1 billion.
These big health systems attributed the financial performance to several factors, including bigger investment gains and higher-acuity patients.
Seven health systems that posted net income of $1 billion last year:
1. Pittsburgh-based UPMC, an integrated delivery system with 40 hospitals, recorded a net income of $1.1 billion in 2021, driven by an operating income of $843 million and nonoperating gains of $810 million.
2. AdventHealth, a 48-hospital system based in Altamonte Springs, Fla., recorded a net income of $1.5 billion in 2021. The net income included an operating income of $994.6 million and investment gains of $517.7 million. In 2020, the health system’s net income was $914.8 million.
3. Cleveland Clinicreported a 66.7 percent increase in net income for the 12 months ended Dec. 31. The 19-hospital system saw its net income hit $2.2 billion, including an operating income of $746.3 million and investment gains of $1.4 billion.
4. Rochester, Minn.-based Mayo Clinic’s net income for 2021 was $3.6 billion, up from $2.5 billion a year earlier. The results included an operating income of $1.2 billion.
5. Driven by strong investment gains, Oakland, Calif.-based Kaiser Permanenterecorded a net income of $8.1 billion in 2021, an increase of $1.7 billion from 2020. The sharp rise in net income from the integrated delivery system with 39 hospitals included $7.5 billion in other income, including investment gains, and $611 million in operating income for 2021.
6. Nashville, Tenn.-based HCA Healthcare, a 182-hospital system, reported a net income of $7.7 billion in 2021, including investment gains and operating profits.
7. Tenet Healthcare, a 60-hospital system based in Dallas, reported net income of $1.5 billion on revenues of $19.5 billion in 2021. Tenet ended the 12-month period with an operating income of $2.9 billion, up from $2 billion recorded one year before. It also recorded losses on nonoperating activities and said its results for the year ending Dec. 31 included a pretax gain of $406 million associated with the divestiture of five Miami area hospitals, as well as stimulus funds totaling $205 million.
In our recent conversations with executives, we’ve heard that the workforce crisis continues to be the most urgent issue confronting health systems.
It’s a many-sided problem: early retirements hitting the nursing staff, leading to an overall loss of experience; early and mid-career nurses choosing to work for temporary staffing agencies for much higher pay, resulting in increased labor costs and resentment among remaining nurses; and a rising vacancy rate made more challenging by difficulty competing for talent against others offering higher pay and less stressful work environments.
But one factor undermining frontline nurse engagement hadn’t occurred to us, until we heard a chief nursing officer describe it this week. The lingering supply chain crisis is forcing hospitals to change where they purchase basic items—think IV tubing and bags, surgery kits, some basic drugs—which in turn forces nurses to adapt to using unfamiliar supplies on the fly, making for a less predictable work environment. On a busy and staff-constrained nursing unit, even small changes to standard procedures can be incredibly frustrating for nurses, and even lead to patient safety issues. Just another way in which the current environment is creating unprecedented pressure on healthcare workers, with little prospect for improvement anytime soon.
Healthcare professionals in Oklahoma who have cared for COVID-19 patients throughout the pandemic are now facing a facility lockdown due to threats made against them.
Mercy Hospital Oklahoma City upped its security and locked down its intensive care unit following online threats against the facility and its staff, mostly revolving around COVID treatments and conspiracy theories, Becker’s Hospital Review reported.
Claims made during a recent protest outside the facility and online included that the hospital had a “Fauci protocol,” and that it received government vouchers for using certain medications or treatments for COVID patients, which Mercy Hospital denied, according to Becker’s.
Hospital officials released a statement to staff on Friday, which they shared with MedPage Today. “There is truly nothing more important to us than your safety. We have a team monitoring these online attacks in real time. Every level of our ministry is deeply concerned and committed to doing whatever it takes to protect our co-workers against these baseless attacks,” they said.
“We are proud to serve with you,” they added. “We know you are tired and weary, but please try your best to put these baseless claims out of your mind. Remember, you are called to serve our patients and each other. We are praying for peace and protection over each of you, as well as the protection of all our patients and visitors, while we take action on your behalf.”
Late last week, the hospital filed a restraining order against the founder and director of an Oklahoma church group that has been protesting outside the facility and making threats against its staff online, Oklahoma’s KFOR reported.
In a recent press release, the church group, known as Ekklesia Oklahoma, called Mercy Hospital an “evil Marxist controlled death camp.”
Court documents stated that the founder of the group called one of the hospital’s doctors a “murderer,” noting that members even posted the doctor’s home address online, according to KFOR.
Hospital officials told KFOR that they are thankful for local police departments that are providing extra security for staff and patients.
Other hospitals across the U.S. have also received threats to the safety of healthcare workers in recent days.
Last week, the Massachusetts Medical Society said it was “angered” over the recent neo-Nazi protest outside Brigham and Women’s Hospital in Boston that targeted two doctors whose work focuses on health equity.
Carole Allen, MD, MBA, president of the society, told MedPage Today that the protest outside Brigham and Women’s was a threat to healthcare workers who were just trying to do their jobs, as well as to patients, and was so disruptive that it “could endanger healthcare in general.”
House Republicans are demanding the Biden administration starts winding down the COVID-19 public health emergency, while hospital lobbying groups are pressing it to do the opposite.
A group of more than 70 House Republicans wrote Thursday to Department of Health and Human Services (HHS) Secretary Xavier Becerra asking to start the process to wind down the COVID-19 public health emergency (PHE), which was recently extended until April. At the same time, several hospital advocacy groups are hoping the agency keeps the PHE beyond this spring and wants a 60-day notice as to when it will end.
“Although the PHE was certainly necessary at the outset of the pandemic, it was always meant to be temporary,” according to the GOP letter led by Rep. Cathy McMorris Rodgers, R-Washington, ranking member of the House Energy and Commerce Committee.
Republicans want HHS to release a concrete timeline for when the agency plans to exit the PHE.
“We recognize that the PHE cannot end overnight, and that certain actions must be taken to avoid significant disruption to patients and healthcare providers, including working with Congress to extend certain policies like maintaining access to telehealth services for our nation’s seniors,” the letter added.
The PHE granted major flexibilities for providers to get reimbursed by Medicare for telehealth, but those powers will go away after the PHE. It also gave flexibility on several reporting requirements and eased other regulatory burdens.
Another major issue is that states are going to be able to start eligibility redeterminations for Medicaid, which have been paused since the PHE went into effect in January 2020. State Medicaid directors are seeking a heads-up on when the emergency will go away, as states can start to disenroll ineligible beneficiaries after the PHE expires.
Republicans also want Becerra to cite any programs that should be made permanent, and they want “swift action” to lift all COVID-19 vaccine mandates.
The Supreme Court upheld the Biden administration’s healthcare worker vaccine mandate, overturning a lower court’s stay that affected half of the country. The Centers for Medicare & Medicaid Services has deadlines for states to comply with the vaccination mandate, and facilities that don’t fully comply could risk losing participation in Medicare and Medicaid.
The Republicans charge that the mandates have not “stopped the spread of COVID-19 but have alienated many Americans and have caused staff shortages at hospitals and other healthcare facilities.”
Key drivers of the staff shortages, however, have been a massive surge of the virus overwhelming facilities caused by the omicron variant along with increased expenses facilities have faced for temporary nursing staff. Those lingering expenses are the reason hospital groups are pressing for HHS to do the opposite and extend the PHE beyond April.
The Federation of American Hospitals (FAH) also wrote to Becerra Thursday (PDF) seeking to continue to extend the PHE “well beyond its current expiration date in April 2022.” Even though the omicron surge appears to be easing, the virus is still creating major operational challenges for providers, FAH said.
It also wants the administration to give hospitals a 60-day heads-up when it plans to end the PHE.
“Unwinding the complex web of PHE waiver-authorized operations, programs and procedures—which will have been in place and relied on for more than two years—is a major undertaking that, if rushed, risks destabilizing fragile healthcare networks that patients rely on for care,” the letter said.
The American Hospital Association also wrote to congressional leaders Tuesday seeking for more relief from Congress to help systems overcome staffing shortages that have exacerbated due to the omicron surge.
“The financial pressures hospitals and health systems faced at the beginning of the public health emergency continue, with, for example, ongoing delays in non-emergent procedures, in addition to increased expenses for supplies, medicine, testing and protective equipment,” the letter said.
FAH President Chip Kahn told Fierce Healthcare on Friday that the issues Republicans address in the letter are different from the priorities of the FAH, namely that the association doesn’t focus on mask or vaccine mandates.
“What we are saying is that the PHE has many aspects to it, and so … we think [it] should be extended, but if you don’t then we need to have a lengthy or carefully thought through transition,” Kahn said.
He added that Becerra’s predecessor, acting Secretary Eric Hargan, told providers that they would get a 60-day notice before the end of the PHE. That deadline for such a 60-day notice is Feb. 15.
Kahn said he understands the administration may be under political pressure to end the emergency, but prior notice is absolutely needed.
“I don’t know how they will respond but if they do choose to pull out, we just want to make sure that it doesn’t leave anything behind,” he said.
The Mayo Clinic in Minnesota is no longer scheduling appointments for patients in most Medicare Advantage plans, and has been gradually notifying patients throughout the year, in a move that could have consequences for insurers operating plans in the area, according to a Mayo Clinic spokesperson.
Some insurers, such as UnitedHealthcare, have been negotiating with the Mayo Clinic to bring them in-network for Medicare Advantage, in some cases asking them to outline their requested terms, but Mayo to date has yet to send out proposals.
Mayo has long been out of network for most Medicare Advantage plans, but has historically treated out-of-network MA patients and accepted their benefits, according to Mayo Clinic spokesperson Karl Oestreich.
According to the Star Tribune, the change occurred because Mayo saw a significant increase in patients covered by “non-contract” MA insurers. That increase, officials said, threatens to crowd out patients covered by in-network insurers.
Non-contract MA plans are those in which insurance companies have not negotiated payment rates for services with Mayo.
UnitedHealthcare, which has been out of network, is negotiating to bring Mayo in-network for MA members, according to Dustin Clark, vice president for communications at UHC.
“We have asked Mayo Clinic to outline requested terms to join our network for Medicare Advantage and haven’t received a proposal,” he told Healthcare Finance News. “We are committed to reaching an agreement at an affordable cost for the people we serve. We stand at the ready to work with Mayo to end this disruption.”
For UHC, it’s especially important that MA patients who traditionally received care at Mayo can continue to do so in the future.
“Although Mayo Clinic does not participate in our network for Medicare Advantage, many of our members have received treatment from its physicians as part of their out-of-network benefits,” said Clark. “We understand how difficult this situation is for some of our members, which is why we are working with Mayo to ensure our Medicare Advantage members who are currently undergoing treatment or have an established relationship with the clinic can continue to see their physician.”
Mayo Clinic spokesperson Karl Oestreich said that medical need is the primary criteria for obtaining an appointment.
“In situations where medical need does not apply and to ensure appointments remain available for our Mayo Clinic patients, we no longer schedule routine visits for those whose coverage does not include Mayo Clinic,” he said. “Continuity of care and relationships with existing local and regional patients won’t be compromised.”
The primary issue, said Oestreich, is capacity, not reimbursement. He said Mayo doesn’t have the capacity to serve an ever-increasing number of patients, and needs to remain a good steward with its contracted plans.
“There was not a policy change, but a shift in enforcement to ensure Mayo has access for our contracted plans (not just Medicare) and those who truly need Mayo’s medical expertise,” he said. “This long-standing policy applies to all payers, not just Medicare Advantage.”
“The impact is to non-contract Medicare Advantage plans,” said Oestrich. “Mayo does not have contracts with these plans. Mayo is open to entering new contracts, but also must keep in mind the impact on capacity to ensure that we can continue to see those patients (regardless of payer) who are in the greatest need of the care Mayo provides.
“We understand that affected patients may be disappointed and frustrated. Patients should always ask their brokers and insurers whether their plans specifically have in-network coverage at Mayo Clinic.”
THE LARGER TREND
UnitedHealthcare, which already has significant market control with its MA plans, said it will strengthen its foothold in the space by expanding its MA plans in 2022, adding a potential 3.1 million members and reaching 94% of Medicare-eligible consumers in the U.S.
While UnitedHealthcare has a massive foothold in the Medicare Advantage space, it underwent scrutiny from the federal government earlier this month, when the Centers for Medicare and Medicaid Services blocked four Medicare Advantage plans from enrolling new members in 2022 because they didn’t spend the minimum threshold on medical benefits. Three UnitedHealthcare plans and one Anthem plan failed to hit the required 85% mark three years in a row.
Medicare Advantage plans are required to spend a minimum of 85% of premium dollars on medical expenses. Failure to do so for three consecutive years triggers the sanctions.
For UHC, the penalties apply to its MA plans in Arkansas, New Mexico and the Midwest, which encompasses Missouri, Kansas, Nebraska and Iowa. UHC plans cover about 83,000 members, and the Anthem plan covers about 1,200 members. They cannot offer select plans to members until 2023, assuming they hit the 85% threshold next year – what’s called the medical loss ratio. If they fail to hit the threshold for five years in a row, the government will terminate the contracts.
UHC representatives told Bloomberg that it missed the 85% benchmark in certain markets in part because of patients deferring medical care due to the COVID-19 pandemic.
Los Angeles-based Prospect Medical Holdings has inked deals to sell its seven hospitals in Connecticut and Pennsylvania.
The company announced Feb. 10 that it is selling three Connecticut hospitals with a combined 708 beds to Yale New Haven (Conn.) Health System. The deal is expected to close later this year. If the deal is finalized, the hospitals will transition from for-profit to nonprofit organizations.
Prospect Medical Holdings announced Feb. 11 that it is selling Crozer Health, a four-hospital system based in Springfield, Pa., to Newark, Del.-based ChristianaCare. Under the deal, ChristianaCare would acquire Crozer’s hospitals, medical group, ambulatory centers and clinics. Crozer’s hospitals have more than 800 beds combinded.
The deal with ChristianaCare was announced the same day Crozer got a new CEO. The health system appointedKevin Spiegel, senior vice president of strategy and revenue development at Prospect, as its new CEO. He replaced Peter Adamo, who served in that role at Crozer for two years. Mr. Adamo’s last day at Crozer was Feb. 11, according to the Philadelphia Business Journal.
“The pandemic has demonstrated the vital importance of working together to meet the clinical needs of the communities we serve,” Mr. Spiegel said in a Feb. 11 news release. “We are excited by the potential to join these two great organizations so that we can continue to provide the high-quality, accessible care that our communities — Delaware County and beyond — rely on.”
The sale of the hospitals to ChristianaCare is expected to close in the second half of this year. If the deal is finalized, Crozer would become a nonprofit organization.
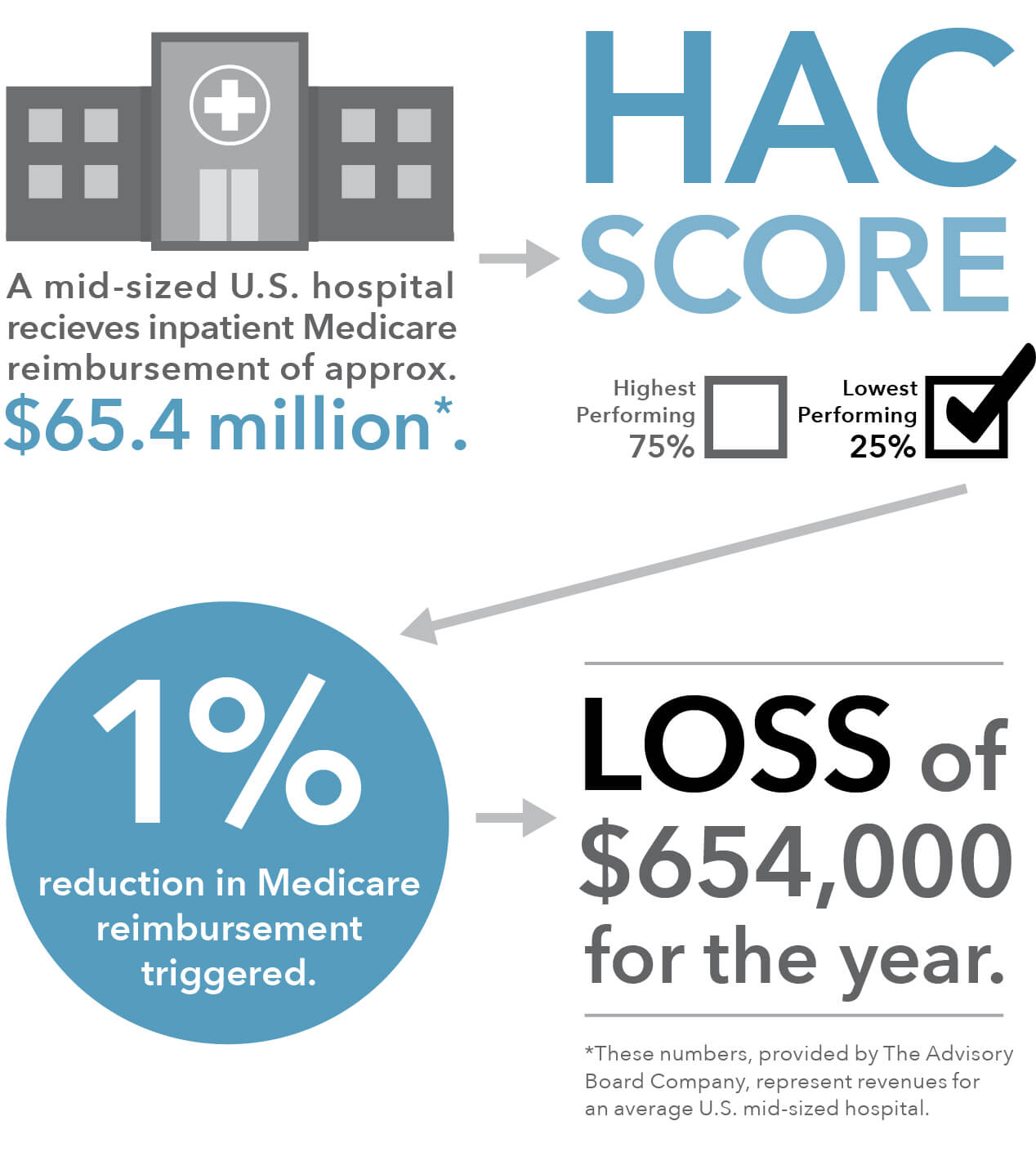
Of the 764 hospitals the Centers for Medicare and Medicaid Services (CMS) is penalizing this year with a one percent reduction in Medicare payments for scoring in the bottom quartile in the Hospital-Acquired Condition Reduction (HAC) Program, 38 also earned a five-star rating from CMS for overall quality of care.
This paradox is in part because Medicare’s star ratings compare a hospital’s safety and quality to a calculated average, whereas the HAC program requires Medicare to penalize the lowest-performing quartile of hospitals each year, even if they are showing improvement, or if the difference between low- and high-performing hospitals is miniscule.
The Gist: The promise of Medicare’s pay-for-performance incentive programs has not materialized, and is unlikely to be driving true clinical improvement. In addition to being confusing and tedious to comply with, the programs lack impact because penalties and rewards are too small to impact a hospital’s bottom line—the benefits don’t justify the costs of redesigning care processes or changing behavior. With years of evidence that many of these ACA-era quality programs aren’t producing the desired results, it’s time to find more effective ways of improving patient outcomes.
Nurses who worked at hospitals owned or operated by Vancouver, Wash.-based PeaceHealth are accusingthe health system of retaliating against them when they raised concerns about patient and worker safety, NBC News reported Feb. 6.
Nurses spoke to the news division about their experiences, including Marian Weber, a travel nurse who was contracted to work at PeaceHealth Ketchikan (Alaska) Medical Center. She told NBC News that she raised concerns about critically ill COVID-19 patients who were placed in a unit with no central monitoring system and spoke up against the hospital’s suggestion of keeping a nurse in the room for 12 hours.
She said PeaceHealth terminated her contract in August 2021.
Ms. Weber filed a complaint with the National Labor Relations Board after her contract was terminated, and a hearing is scheduled for June 7, according to radio station KRBD. She seeks reimbursement for travel expenses, among other things.
In addition to Ms. Weber, Sarah Collins told NBC News that she lost her staff nursing job at PeaceHealth Southwest Medical Center in Vancouver after raising safety concerns, specifically regarding staffing and nurse-to-patient ratios.
According to the news division, Ms. Collins was put on a three-month leave in September after giving a local news interview. She told NBC News she was terminated for “operating outside her scope of practice” and “failing to follow policy.” She also has a complaint pending with the National Labor Relations Board.
Separately, NBC News reported, there is an ongoing lawsuit, filed in April 2020, claiming that PeaceHealth Southwest prevented workers from taking required meal and rest breaks allowed under law and that workers were discouraged from reporting missed breaks.
In a statement shared with Becker’s, PeaceHealth declined to comment on personnel issues or pending cases but said it emphasizes ensuring safety of employees and patients.
“We can wholeheartedly reinforce that the voices and opinions of our caregivers matter, and any concern brought forward is thoroughly reviewed,” the statement said. “We have hardwired safety into all our processes, including a longstanding ‘safe to share’ platform that empowers every caregiver — no matter their role — with the ability to confidentially raise opportunities to ensure safer care. This best-practice approach is part of our commitment to continuously improve and vision to ensure 100 percent safe care.”
“PeaceHealth medical centers’ overall quality and safety outcomes have been maintained in spite of the challenges presented by the pandemic, and our approach continues to ensure top-tier care in the communities we serve,” the health system added.
Read the NBC News report here. Read the KRBD report here.
Despite the gains, employment in healthcare is down by about 378,000 jobs (2.3%) from where it was in February 2020.
After a rough end to 2021 in terms of job losses,healthcare appears to be on the rebound – for now. The latest jobs report from the U.S. Bureau of Labor Statistics showed hospitals gaining jobs in January, though the industry is still below the levels seen before the COVID-19 pandemic.
In total, the healthcare sector saw a gain of 18,000 jobs last month. It lost 3,100 jobs in December; the prior month, November 2021, was the last time the sector saw job gains, when it posted a net gain of 2,100.
Hospitals made up for some, but not all, of the job losses seen during the tail end of 2021. They gained 3,400 jobs in January, after losing 5,100 jobs in December and 3,900 in November.
The last time hospitals gained jobs was in October, when 1,100 were added. Hospitals lost 8,100 jobs in September.
The biggest increase was in ambulatory healthcare services, which gained 14,700 jobs during the month. Physicians’ offices added 9,700 jobs. Nursing and residential-care facilities lost about 100 jobs in January.
Despite the gains, employment in healthcare is down by about 378,000 jobs (2.3%) from where it was in February 2020, at the dawn of the pandemic, according to BLS.
The broader U.S. economy added 467,000 jobs in January, after gaining 199,000 jobs in December, while the unemployment rate held fairly steady at about 4%.
WHAT’S THE IMPACT?
In a preview of the jobs report by economic research firm Glassdoor, researchers predicted that job losses in healthcare and leisure and hospitality would drag down overall payroll employment. Other coronavirus-sensitive sectors, such as retail and education, were also impacted, though seasonal factors helped mute job losses in those sectors.
Over the course of the pandemic, new COVID-19 cases have been somewhat predictive of job market data, but current record levels represent a situation without precedent, and there are few good comparisons, Glassdoor found. Since September 2020, each new 1,000 daily cases has been correlated with 4,000 fewer job gains, but the level of cases seen in January is unlike any other previous point in the pandemic, leading to uncertainty heading into the BLS jobs report.
The Bureau of Labor Statistics’ preliminary benchmark estimates forecast a modest downward revision in payroll employment of 166,000 for March 2021.
THE LARGER TREND
The Great Resignation hit the healthcare sector hard in November. BLS released job numbers in January showing that healthcare is among the top three industries cited in a 3% rise in the monthly “quits rate,” matching a high from September. The number of quits surged to 4.53 million for the month.
The numbers coincide with an already-strapped healthcare staffing market. Shortages and burnout among healthcare staff are a pervasive issue.
Multiple factors are contributing to labor pressures, including staff burnout stemming from the enduring pandemic and an overall shortage of qualified help, which has resulted in higher costs to hire temporary staff, as well as wage inflation.
Further, a Fitch Ratings report in November noted that lack of staff is forcing some in-patient behavioral health and senior housing operators to lower admission rates.