Blueprint includes cuts for care in hospital outpatient departments, teaching hospitals and post-acute care providers, AHA says.
President Trump’s proposed $4.8 trillion budget slashes billions of dollars from Medicaid, food stamps and other safety net programs in an attempt to shrink the federal deficit.
Medicaid and the Affordable Care Act see about $1 trillion in cuts over the next decade, according to The Hill. The budget eliminates the enhanced federal match for Medicaid expansion enrollees. An additional $150 billion is expected to be shaved off of Medicaid from the implementation of work requirements, which is expected to result in people losing their healthcare coverage.
The “President’s health reform vision” to ax the Affordable Care Act takes $844 billion over 10 years from the ACA, the report said.
The decrease in federal spending on Medicare would total about $750 billion over 10 years, but that includes shifting two programs out of the budget. After accounting for those changes, the reduction is just over $500 billion, according to CNN. Much of that cut comes from reducing payments to providers.
The budget needs Congressional approval and is not expected to get past a Democratic-controlled House without changes.
House Speaker Nancy Pelosi tweeted: “The budget is a statement of values. Once again, the #TrumpBudget makes it painfully clear how little the President values the good health, financial security and well-being of America’s hard-working families.”
Ways and Means Committee Chairman Richard E. Neal, D-MA, said, “When I saw the President’s proposed budget today, I felt an immense sense of relief – relief that there is absolutely no chance of his ruthless cuts to critical programs ever becoming law. Slashing billions from Medicare and Medicaid will only make it harder for Americans to access the healthcare they need.
Cutting nutrition assistance and Social Security benefits for the disabled won’t enable people to get back on their feet financially.”
Senator Lamar Alexander, R-Tenn said, “Under the Constitution, it is Congress’ job to set spending priorities and pass appropriations bills, and as a member of the Senate Appropriations Committee, my priorities will continue to be making sure our national defense, national laboratories, the National Institutes of Health and national parks have the resources they need. I am encouraged to see the president is calling to end surprise medical billing.”
The budget adds money to the National Institutes of Health. The NIH will invest $50 million for new research on chronic diseases, using AI and related approaches, according to the White House briefing. It adds $7 billion over 10 years to fight opioid abuse and for mental health in the Medicaid program.
WHY THIS MATTERS
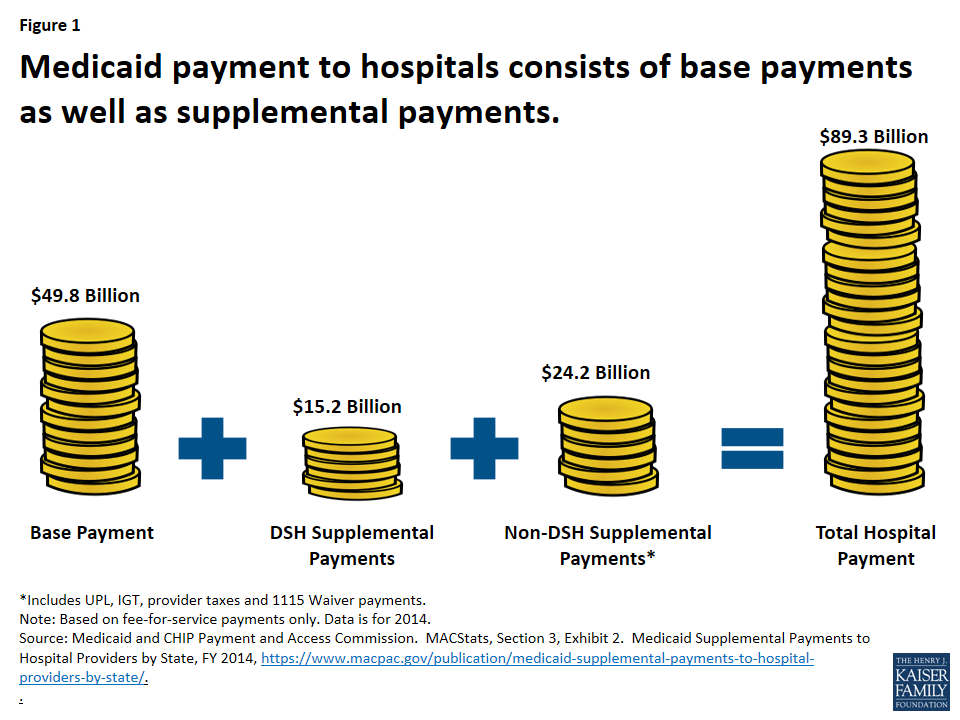
Cuts to Medicare and Medicaid mean uncompensated care to providers, or a reduction in the government payments.
The American Hospital Association said, “The budget request, which is not binding, proposes hundreds of billions of dollars in reductions to Medicare and Medicaid over 10 years.”
AHA President and CEO Rick Pollack said, “Every year, we adapt to a constantly changing environment, but every year, the Administration aims to gut our nation’s healthcare infrastructure. The proposals in this budget would result in hundreds of billions of dollars in cuts that sacrifice the health of seniors, the uninsured and low-income individuals. This includes the one in five Americans who depend on Medicaid, of which 43% of enrollees are children.
“In addition to the hundreds of billions in proposed reductions to Medicare, the blueprint includes cuts we strongly oppose for care in hospital outpatient departments, teaching hospitals and post-acute care providers. These cuts fail to recognize the crucial role hospitals serve for their communities, such as providing 24/7 emergency services. Post-acute cuts threaten care for patients with the most medically complex conditions.”