Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
Health officials are grappling with how to prevent potential COVID-19 outbreaks from the delta variant that is spreading rapidly across the U.S.
Concern over the highly transmissible delta strain prompted Los Angeles County this week to recommend that all people wear masks indoors, even if they’re vaccinated. The World Health Organization (WHO) has also encouraged fully vaccinated people to continue using masks.
But the Centers for Disease Control and Prevention (CDC) has not signaled any plans to revise its mask guidance, with Biden administration officials and some experts say that fully vaccinated Americans are safe from all existing COVID-19 variants.
“If you have been vaccinated, the message we’re conveying is you’re safe,” White House press secretary Jen Psaki said Wednesday. “Vaccines are effective, and that is something we want to be very clear with the public about.”
Still, the move by officials in Los Angeles County raises the prospect that mask recommendations and even mandates could make a return to certain parts of the country.
The CDC projected the delta variant made up more than a quarter of cases in the U.S. in the most recent two-week period, ending June 19 — a jump from 10 percent the previous two weeks.
Los Angeles County issued a statement Monday saying it “strongly recommends” all people wear masks in indoor settings where they don’t know everyone’s vaccination status.
Barbara Ferrer, director of the county’s Department of Public Health, told The Hill that officials want to take time to get more people vaccinated as research is conducted on delta variant transmission from the fully vaccinated.
“While we’re doing that work with building confidence, we’re going to go ahead and offer as much protection as possible for everyone,” she said.
Leana Wen, an emergency physician and public health professor at George Washington University, praised the county’s decision as the “right move,” saying she hopes other jurisdictions follow suit to protect both vaccinated and unvaccinated residents.
“People who are fully vaccinated are still at risk, albeit a low risk, from those who are unvaccinated,” Wen said.
“Fully vaccinated people can be around others who are fully vaccinated without any limitations,” she added. “However, if they’re going to be around unvaccinated people or vaccination status is not being checked, then those could be high-risk settings” where masks should be worn.
For now, Los Angeles County is an outlier as cities and states continue to loosen mask requirements. Washington’s King County, home to Seattle, and Pennsylvania were the latest jurisdictions to end their mandates, taking that step this week.
CDC Director Rochelle Walensky told NBC’s “Today” on Wednesday that the agency’s guidance that fully vaccinated people don’t need masks in most settings has not changed. She said the WHO has given conflicting instructions, saying the international organization is focused on the global community, which has a lower vaccination rate than the U.S.
“We have always said that local policymakers need to make policies for their local environment,” Walensky said. “But those masking policies are not to protect the vaccinated, they’re to protect the unvaccinated.”
So far, the delta strain has not led to any changes in masking policies at the White House or the Capitol.
The White House does not require masks if a person is vaccinated, although the administration is not checking to see whether all maskless people have gotten their COVID-19 shots.
In recent weeks, the House has ended its universal mask requirement, and few people in the Capitol continue to wear them. The overwhelming majority of lawmakers in both parties have shed masks and freely gather in large groups on the House floor.
The Senate, which never had a mask requirement since nearly all senators voluntarily wore facial coverings when it was recommended, has also relaxed its pandemic restrictions.
But the delta variant threat is influencing other activities in the House. Speaker Nancy Pelosi (D-Calif.) announced this week that proxy voting would be extended through Aug. 17, and House Majority Leader Steny Hoyer (D-Md.) said that was due to the global spread of the delta variant.
“As we know, there are some countries in the world that are seeing a virulent resurgence of this new variant of the COVID-19. Israel is a perfect example of that,” Hoyer told reporters, referring to Israel reimposing its indoor mask mandate despite having one of the world’s highest vaccination rates. “But even in Israel, where they have the vaccine available, they’re seeing a resurgence.”
“So, the Speaker correctly, along with the medical advice that she’s gotten, determined that there was still justification for staying on guard,” Hoyer said.
Recent studies have found that COVID-19 vaccines are effective against the strain. Both doses of Pfizer-BioNTech were found to be 88 percent effective against symptomatic disease.
There is “less data” on how Johnson & Johnson performs, Walensky said Wednesday, but “right now we have no information to suggest that you need a second shot after J&J, even with the delta variant.”
Jen Kates, senior vice president and director of global health & HIV policy at the Kaiser Family Foundation, said research shows the CDC guidance “still stands,” although she acknowledged the agency needs to be prepared to adjust.
Kates expressed concern that the resurgence of the mask debate could affect the vaccination effort, noting the variant is spreading mostly among unvaccinated people.
“The worst outcome, I think, is that people choose not to get vaccinated because they think the vaccines aren’t as effective against variants,” she said.
As most Americans have gotten vaccinated, COVID-19 cases, hospitalizations and deaths have declined significantly. But the U.S. is expected to fall short of President Biden’s goal to have 70 percent of adults receiving at least one vaccine dose by the Fourth of July.
The White House still plans to move forward with Independence Day festivities. The administration sent 1,000 invitations for people to gather at 1600 Pennsylvania Ave. on Sunday, with vaccinated people allowed to go without masks. All guests were instructed to get tested one to three days before arriving.
“We certainly feel comfortable and confident moving forward with our event here at the White House and individuals having barbecues in their backgrounds this week to celebrate the Fourth of July,” Psaki said on Wednesday.
It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,”AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
As the delta variant of the coronavirus spreads, especially among the unvaccinated, the Biden administration is gearing up for a new push to vaccinate the so-called “movable middle”—and some public health experts say FDA could advance that goal by fully approving Covid-19 vaccines.
Analysis reveals toll of US Covid-19 deaths among unvaccinated patients
According to an analysis by the Associated Press, nearly all recent Covid-19 deaths have occurred in unvaccinated individuals.
The AP analysis is based on data from CDC, although CDC has not itself released estimates of the share of Covid-19 deaths among unvaccinated patients.
According to the AP analysis, just 0.8% of Covid-19 deaths in May were among the fully vaccinated. Meanwhile, the share of hospitalized patients who were fully vaccinated was just 0.1% in May, with fewer than 1,200 fully vaccinated people hospitalized out of more than 853,000 hospitalizations.
Meanwhile, according to CDC, 54% of the U.S. population, including 66% of American adults, have received at least one dose of a Covid-19 vaccine, while 46.1% of the total population and 56.8% of American adults have received all required doses.
In many places across the United States, COVID-19 feels over. Unmasked citizens run rampant. New York City is planning an August mega-concert in Central Park. I’m as hopeful as the rest of us, but I think we may be suffering from memory loss.
Let’s start from this time last year, when many Americans were exuberantly returning to newly reopened beaches, parks and restaurants after a seemingly eternal three months—three whole months!—of quarantine. Universal observance of safety guidelines was surely going to be sufficient to limit viral spread.
We know how that turned out. By mid-June 2020, there were already signs that our bleary-eyed re-emergence was premature. On June 22, 2020, the number of new daily cases of COVID-19 (33,485) surpassed the high-water mark hit on the worst day of the horrific first surge, when that figure peaked at just over 32,000.
A year later, the daily case count is not as foreboding—nor is it nearly as low it may appear.
You’ll notice that this graph covers only the past 12 weeks, while virtually every chart you’ll find (including the one on TIME’s dashboard) graphs COVID-19 cases from the beginning of the outbreak. This is intentional. The toll of the pandemic in the U.S. has persisted for so long, and reached such catastrophic heights in the first weeks of 2021, that patterns such as this one are nearly impossible to see on the typical chart. Here’s what the same graph looks like against that backdrop:
My fear is that the pandemic remains much more deadly than how it looks on the page. Yes, deaths remain on a steady decline, having recently sunk below 300 people a day on average for the first time since March 24, 2020, right around the time that many offices were shuttering. But a surge in cases, particularly among the large number of unvaccinated Americans, could quickly reverse that decline.
As you can see, it has been less than a month since the 2021 case count sunk below the year-over-year figure, on May 26. The massive nationwide vaccine rollout is undoubtedly a major factor, but it’s difficult to quantify the impact of vaccination on the currently low case and death figures. There are only weak correlations between states’ vaccination rates and some key indicators, like the rate at which cases have risen or fallen in recent weeks.
What we can quantify is that, in the 27 days since the lines crossed, the vaccination rate in the U.S. has only crawled upward, from 39.7% to 45.3% of Americans who have received a complete dosage. While the official vaccination rate applies to the entire population, data from the U.S. Centers for Disease Control and Prevention (CDC) also includes percentages for several age groups. By TIME’s calculations, there are 97.4 million adults age 18 and over who have been eligible for vaccination for two months but who have not yet received even a first dose. This group trends heavily younger, with those 65 and over representing only 7.8% of the unvaccinated population. (These figures do no include those under 18, who constitute a small portion of the eligible population.)
On May 13, two weeks before daily case numbers in 2021 fell below the year-over-year figures from the same day in 2020, the CDC issued guidance liberating fully vaccinated individuals from wearing masks in many scenarios. I do not have conclusive proof that any of the country’s 97.4 million unvaccinated adults have abused this privilege. All I can state with confidence is that, based on the number of people I’ve seen not wearing a mask in places like stores, which often have signs imploring those who are not fully vaccinated to continue to mask up, it is mathematically almost certain that more than a few have done so.
Which is to say: the situation today, if one can momentarily rewind to Memorial Day of 2020, feels very familiar. There appears to be a lambent light at the end of the tunnel, yet cavalier attitudes towards the pandemic, particularly among younger people who, as a group, are under-vaccinated, resembles what we saw last summer just before the second wave.
Watching these trends, I grow more concerned every day that the country is positioned for yet another surge in cases, despite our defensive upgrades in the off-season. I hope I’m wrong, but the numbers are not nearly as comforting as they first look. The fact that the Delta variant, which is both more transmissible and appears to cause more severe disease, is on pace to become the dominant form of COVID-19 in the U.S. in the coming months is further reason for alarm. Moreover, some states have significantly higher vaccination rates than others, leaving those with less protection more vulnerable to future spikes.
Forgive me for being a buzzkill, but unless we can institute a functional vaccine passport system, which appears unlikely, I do not think it is wise to assume that every unmasked individual is fully dosed. Short of a passport system, and with dangerous variants competing for dominance and the duration of vaccine protection still unclear, we ought to continue to ration physical space in public areas—a policy that is hastily being relaxed at places like Major League Baseball parks. I love baseball and eagerly look forward to buzzing up to Philadelphia to take in a game at Citizen’s Bank Park, which is operating at full capacity. But not while the policy is that “Unvaccinated fans are strongly encouraged to wear their masks in all indoor and outdoor areas in and around the ballpark.”
I also think there might be a backdoor to a digital passport system. Based on polling data, it appears there is a substantial population of people who aren’t categorically opposed to vaccination, just unmotivated to get around to it—what we’ve termedvaccine “meh-sitance,” not hesitance. My proposal is that bars, restaurants and other popular venues merely require each person who enters to verbally affirm that they are fully vaccinated.
This might sound about as effective as asking passengers in the exit row to individually verify that they listened to the instructions. But while it’s one thing to ignore a sign at the grocery store, it’s another to lie in front of your friends. Peer pressure is a powerful motivator, and if even a fraction of the unvaccinated would take the time to resolve that dissonance, or risk missing out on trivia night, it could substantially push up the percentages. I call this the “FOMO method,” and though we are still a long, long way from eliminating the disease altogether, it could help us avert a fourth wave this summer.
An argument for humility in the face of pandemic forecasting unknown unknowns.
“Are we battling an unprecedented pandemic or panicking at a computer generated mirage?” I asked at the beginning of the COVID-19 pandemic on March 18, 2020. Back then the Imperial College London epidemiological model’s baseline scenario projected that with no changes in individual behaviors and no public health interventions, more than 80 percent of Americans would eventually be infected with novel coronavirus and about 2.2 million would die of the disease. This implies that 0.8 percent of those infected would die of the disease. This is about 8-times worse than the mortality rate from seasonal flu outbreaks.
Spooked by these dire projections, President Donald Trump issued on March 16 his Coronavirus Guidelines for America that urged Americans to “listen to and follow the directions of STATE AND LOCAL AUTHORITIES.” Among other things, Trump’s guidelines pressed people to “work or engage in schooling FROM HOME whenever possible” and “AVOID SOCIAL GATHERINGS in groups of more than 10 people.” The guidelines exhorted Americans to “AVOID DISCRETIONARY TRAVEL, shopping trips and social visits,” and that “in states with evidence of community transmission, bars, restaurants, food courts, gyms, and other indoor and outdoor venues where people congregate should be closed.”
Let’s take a moment to recognize just how blindly through the early stages of the pandemic we—definitely including our public health officials—were all flying at the time. The guidelines advised people to frequently wash their hands, disinfect surfaces, and avoid touching their faces. Basically, these were the sort of precautions typically recommended for influenza outbreaks. On July 9, 2020, an open letter from 239 researchers begged the World Health Organization and other public health authorities to recognize that COVID-19 was chiefly spread by airborne transmission rather than via droplets deposited on surfaces. The U.S. Centers for Disease Control and Prevention (CDC) didn’t update its guidance on COVID-19 airborne transmission until May 2021. And it turns out that touching surfaces is not a major mode of transmission for COVID-19.
The president’s guidelines also advised, “IF YOU FEEL SICK, stay home. Do not go to work.” This sensible advice, however, missed the fact that a huge proportion of COVID-19 viral transmission occurred from people without symptoms. That is, people who feel fine can still be infected and, unsuspectingly, pass along their virus to others. For example, one January 2021 study estimated that “59% of all transmission came from asymptomatic transmission, comprising 35% from presymptomatic individuals and 24% from individuals who never develop symptoms.”
The Imperial College London’s alarming projections did not go uncontested. A group of researchers led by Stanford University medical professor Jay Bhattacharya believed that COVID-19 infections were much more widespread than the reported cases indicated. If the Imperial College London’s hypothesis were true, Bhattacharya and his fellow researchers argued, that would mean that the mortality rate and projected deaths from the coronavirus would be much lower, making the pandemic much less menacing.
The researchers’ strategy was to blood test people in Santa Clara and Los Angeles Counties in California to see how many had already developed antibodies in response to coronavirus infections. Using those data, they then extrapolated what proportion of county residents had already been exposed to and recovered from the virus.
Bhattacharya and his colleagues preliminarily estimated that between 48,000 and 81,000 people had already been infected in Santa Clara County by early April, which would mean that COVID-19 infections were “50-85-fold more than the number of confirmed cases.” Based on these data the researchers calculated that toward the end of April “a hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%.” As I optimistically reported at the time, that would imply that COVID-19’s lethality was not much different than for seasonal influenza.
Bhattacharya and his colleagues conducted a similar antibody survey in Los Angeles County. That study similarly asserted that COVID-19 infections were much more widespread than reported cases. The study estimated 2.8 to 5.6 percent of the residents of Los Angeles County had been infected by early April. That translates to approximately 221,000 to 442,000 adults in the county who have had the infection. “That estimate is 28 to 55 times higher than the 7,994 confirmed cases of COVID-19 reported to the county by the time of the study in early April,” noted the accompanying press release. “The number of COVID-related deaths in the county has now surpassed 600.” These estimates would imply a relatively low infection fatality rate of between 0.14 and 0.27 percent.
Unfortunately, from the vantage of 14 months, those hopeful results have not been borne out. Santa Clara County public health officials report that there have been 119,712 diagnosed cases of COVID-19 so far. If infections were really being underreported by 50-fold, that would suggest that roughly 6 million Santa Clara residents would by now have been infected by the coronavirus. The population of the county is just under 2 million. Alternatively, extrapolating a 50-fold undercount would imply that when 40,000 diagnosed cases were reported on July 11, 2020, all 2 million people living in Santa Clara County had been infected by that date.
Los Angeles County reports 1,247,742 diagnosed COVID-19 cases cumulatively. Again, if infections were really being underreported 28-fold, that would imply that roughly 35 million Angelenos out of a population of just over 10 million would have been infected with the virus by now. Again turning the 28-fold estimate on its head, that would imply that all 10 million Angelenos would have been infected when 360,000 cases had been diagnosed on November 21, 2020.
COVID-19 cases are, of course, being undercounted. Data scientist Youyang Gu has been consistently more accurate than many of the other researchers parsing COVID-19 pandemic trends. Gu estimates that over the course of the pandemic, U.S. COVID-19 infections have roughly been 4-fold greater than diagnosed cases. Applying that factor to the number of reported COVID-19 cases would yield an estimate of 480,000 and 5,000,000 total infections in Santa Clara and Los Angeles respectively. If those are ballpark accurate, that would mean that the COVID-19 infection fatality rate in Santa Clara is 0.46 percent and is 0.49 percent in Los Angeles. Again, applying a 4-fold multiplier to take account of undercounted infections, those are both just about where the U.S. infection fatality rate of 0.45 percent is now.
The upshot is that, so far, we have ended up about half-way between the best case and worst case scenarios sketched out at the beginning of the pandemic.
One half of America is protected. The other is approaching a perilous moment in the pandemic.
Lineage B.1.617.2, now known as the Delta variant, was first detected in India, in December, 2020. An evolved version of sars-CoV-2, Delta has at least a dozen mutations, including several on its spike protein that make it vastly more contagious and possibly more lethal and vaccine-resistant than other strains. In India,the Delta variant contributed to the most devastating coronavirus wave the world has seen so far; now, it has been detected in dozens of countries, including the United States. In the U.S., it accounts for a minority of cases—but it is rapidly outcompeting other variants, and will likely soon become our dominant lineage.
Much of what we know about Delta is preliminary, and based on reports from India and, more recently, the U.K., where it now accounts for more than ninety per cent of new cases. Four-fifths of British adults have received at least one shot of a covid-19 vaccine, and more than half are fully vaccinated—but the variant has spread widely enough among those who remain vulnerable to fuel a quadrupling of cases and a doubling of hospitalizations in the past month. The vast majority of Delta-variant cases seem to have occurred in adults under fifty, whose rates of vaccination remain lower than those of older people. Last week, Prime Minister Boris Johnson announced that the U.K.’s full reopening, originally scheduled for June 21st, would be postponed.
Earlier this year, scientists estimated that lineage B.1.1.7—the Alpha variant, first isolated in England—could be some sixty per cent more transmissible than the original version of sars-CoV-2.Now, experts believe that the Delta variant is sixty per cent more transmissible than Alpha—making it far more contagious than the virus that tore through the world in 2020. It hasn’t yet been conclusively shown that Delta is more lethal, but early evidence from the U.K. suggests that, compared to Alpha, it doubles the risk of a person’s being hospitalized. Even if the variant turns out to be no deadlier within any one person, its greater transmissibility means that it can inflict far more damage across a population, depending on how many people remain unvaccinated when it strikes.
In this regard, India’s apocalyptic surge is Exhibit A. In May, at the crest of the wave, the role of the Delta variant was still unclear. A number of factors—the return of large gatherings, a decline in mask-wearing, and a sluggish vaccination campaign—had made a disaster of some kind more or less unavoidable. But it now seems likely that the rise of Delta accelerated the crisis into a shockingly rapid and widespread viral catastrophe. In the course of weeks, millions of people were infected and tens of thousands died; the country’s medical system buckled under the weight of a mutated virus. One of the most disturbing aspects of India’s surge was that many children fell ill. And yet there is currently no data to suggest that Delta causes severe illness in a greater proportion of kids; instead, it seems likely that the sheer transmissibility of the variant simply resulted in a higher absolute number of infected children.
One vitally important finding to emerge from the U.K. and India is that the covid vaccines are still spectacularly effective against Delta. According to one study from the U.K., a full course of the Pfizer-BioNTech vaccine is ninety-six per cent effective at preventing hospitalizations due to the Delta variant; AstraZeneca’s vaccine is in the same ballpark, reducing the chance of hospitalization by ninety-two per cent. But these findings come with caveats. The first is that, with Delta, partial immunization appears to be less effective at preventing disease: a different study found that, for people who have received only the first shot, the vaccines were just thirty-three per cent effective at preventing symptomatic illness. (A first dose still appears to offer strong protection against hospitalization or death.) The second is that even full courses of the vaccines appear somewhat less effective at preventing infection from Delta. This may be especially true of the non-mRNA vaccines. A team of scientists in Scotland has found that both doses of AstraZeneca’s vaccine reduced the chance of infection with Delta by just sixty per cent—a respectable showing, but less impressive than what the same vaccine offers against other strains of the virus. (The Pfizer-BioNTech vaccine demonstrated seventy-nine per cent efficacy against Delta infection—a significant, but smaller, decrease.)
Taken together, these findings have led some experts to propose adjustments in vaccination strategy. Muge Cevik, an infectious-diseases expert at St. Andrews University and an adviser to the British government, told me that, given the arrival of Delta, it was important to ask “what our main aim of vaccination is.” She went on, “If our primary objective is to reduce hospitalizations and deaths, a first dose still gives very good protection. If it’s to stamp out transmission, then the second dose becomes quite important. I think that, especially in hot spots, we need to expedite second shots.” Others have proposed the idea of mRNA-vaccine booster shots for Americans who have received the Johnson & Johnson vaccine, which, like AstraZeneca’s, uses non-mRNA technology. The C.D.C.’s official guidelines tell Americans that “the best covid-19 vaccine is the first one that is available to you. Do not wait for a specific brand.” But that advice was minted when vaccine supply was constrained. The accumulated evidence has led many people to wonder whether the mRNA vaccines, from Moderna and Pfizer, are preferable to the one offered by Johnson & Johnson, and whether the Delta variant makes them even more so.
“It’s likely that J. & J. offers strong protection against severe disease, but because it’s a one-shot regimen it might not offer the same protection against infection for a highly transmissible variant like Delta,” Angela Rasmussen, a virologist at the Vaccine and Infectious Disease Organization, told me. “A second shot reëxposes the immune system to the vaccine, and allows the body to make even better antibodies.” Rasmussen received the J. & J. vaccine; she lives in Canada, where health authorities have encouraged people to mix and match the vaccines. “I’m considering topping off my immune system with a dose of Pfizer,” she said. “It’s something worth thinking about.”
To a significant degree, the emergence of a variant like Delta was predictable, and, with rapid and widespread immunization, the threat that it poses can be subdued. But its arrival is still incredibly consequential. Delta drives an even wider wedge between vaccinated and unvaccinated people. They have already been living in separate worlds, facing vastly different risks of illness and death; now, their risk levels will diverge further. People who’ve been fully vaccinated can, by and large, feel confident in the immunity that they’ve received. But those who remain susceptible should understand that, for them, this is probably the most dangerous moment of the pandemic.
“The good news is that we have vaccines that can squash the Delta variant,” Eric Topol, the director of the Scripps Research Translational Institute, told me. “The bad news is that not nearly enough people have been vaccinated. A substantial share of Americans are sitting ducks.” He went on, “We haven’t built a strong enough vaccination wall yet. We need a Delta wall”—a level of vaccination that will prevent the new variant from spreading. “There are still large unvaccinated pockets in the country where this could get ugly,” Topol added. Because about half of Americans are vaccinated, and millions more have some immunity from prior infection, the Delta variant “won’t cause monster spikes that overwhelm the health system,” Topol said. But Delta spreads so easily among the unvaccinated that some communities could experience meaningful increases in death and disease this summer and fall.
In America, the speed of vaccination is slowing. In some states, mainly in the South, only about a third of the population has been fully vaccinated. Big differences in the covid-19 toll are already visible: cases and hospitalizations have plummeted in some places with higher vaccination rates but are holding steady or rising in others. Fortunately, nearly ninety per cent of older Americans—the group most at risk for severe covid—have received at least one shot, and three-quarters are fully vaccinated. But, as is clear from the Indian and U.K. experiences, the Delta variant could still lead to major spikes in infection among younger, unvaccinated people.
In a recent piece, I likened a society that’s reopening while partially vaccinated to a ship approaching an iceberg. The ship is the return to normal life and the viral exposure that it brings; the iceberg is the population of unvaccinated people. Precautions such as social distancing can slow the speed of the ship, and vaccination can shrink the size of the iceberg. But, in any reopening society that’s failed to vaccinate everyone, a collision between the virus and the vulnerable is inevitable.
Because of its exceptional transmissibility, the Delta variant is almost certain to intensify the force of the collision. The U.K., by postponing a full reopening, is trying to soften the blow. But the U.S. is pressing ahead—perhaps out of hubris, or because officials hope that our vaccination campaign can outrun the spread of Delta. Last week, New York and California, among the pandemic’s hardest-hit states, did away with virtually all restrictions. Meanwhile, states with half the vaccination rates of New York or California have been open for weeks. A lot depends on where, and how fast, Delta is spreading.
Federal, state, and local officials are trying to accelerate vaccination. Governors have announced incentives such as lotteries, college scholarships, gift cards, and free beer for those who get immunized; California alone plans to spend more than a hundred million dollars on vaccine incentives. The Biden Administration has made immunizing seventy per cent of American adults by the Fourth of July a central priority, and has declared June a “national month of action.” The Administration has offered tax credits to employers that provide paid time off for people to get immunized, erected mass-vaccination sites, sent funds to community health centers, and partnered with local organizations, celebrities, and volunteers to get shots in arms. The White House recently announced that four of the nation’s largest child-care providers would offer free services to parents who want to get immunized before July 4th; Uber and Lyft have been offering free rides to vaccination sites for weeks.
And yet, the pace of vaccinations hasn’t picked back up. Topol, for his part, believes that a major impediment to wider vaccination is the fact that the F.D.A. has not yet fully approved the covid vaccines; right now, they’ve received only an emergency-use authorization, or E.U.A. About a third of unvaccinated Americans say that F.D.A. approval would make them more likely to get immunized. Full approval could also pave a clearer path for vaccine mandates in schools, businesses, and the military. Topol argues that mandates would allow us to build a Delta wall more quickly—along with walls for Epsilon, Zeta, and the rest of the Greek alphabet. Both Pfizer and Moderna have applied for F.D.A. approval, but it’s unclear how soon they will receive it; the usual process takes six to ten months. “Hundreds of millions of people have safely taken these vaccines, but there’s still a perception among some that they’re experimental,” Topol said. “E.U.A. versus full approval may sound like semantics, but it’s actually a B.F.D.”
Globally, more people died of the coronavirus in the first half of this year than in all of last year—an astounding fact, given the emergence of the vaccines. The tragic truth is that, for much of the world, the vaccines may as well not exist. On the one hand, the U.S. is vaccinating children as young as twelve; on the other hand, health-care workers, elderly people, and cancer patients in many other countries remain defenseless. Three-quarters of covid-vaccine shots have been administered in just ten countries, whereas the poorest nations have received less than one half of one per cent of the supply. Tedros Adhanom Ghebreyesus, the W.H.O. director-general, has called this a “scandalous inequity.”
The Biden Administration recently announced that the U.S. would donate half a billion doses to the global vaccination effort; it hopes to deliver two hundred million by the end of the year. The U.K. and other European countries have also committed hundreds of millions of doses to covax, the international initiative to distribute vaccines to low- and middle-income countries. These efforts are important, and they will help immensely—but not for months, and perhaps not until 2022. In the meantime, many countries will continue to grapple with the social and economic challenges created by variant-catalyzed surges and the public-health measures needed to thwart them. Even where the political will for continuing such measures exists, it’s not infinite; countries can’t remain in lockdown forever.
In a sense, Delta is the first post-vaccination variant. Pockets of the human race—perhaps five hundred million people out of 7.6 billion—are protected against it, despite its transmissibility; for them, the pandemic’s newest chapter is something of an epilogue, since the main story has, in effect, already concluded. But, for those who remain unvaccinated, by choice or by chance, Delta represents the latest installment in an ongoing series of horrors. It’s a threat more sinister than any other—one that imperils whatever precarious equilibrium has taken root. In a partially vaccinated world, Delta exposes the duality in which we now live and die.
In the first federal ruling on vaccine mandates, a Houston judge Saturday dismissed a lawsuit by hospital employees who declined the COVID-19 shot – a decision that could have a ripple effect across the nation.
The case involved Houston Methodist, which was the first hospital system in the country to require that all its employees get vaccinated. U.S. District Judge Lynn N. Hughes said federal law does not prevent employers from issuing that mandate.
The hospital already had made it clear it means what it says: It fired the director of corporate risk – Bob Nevens – and another manager in April when they did not meet the earlier deadline for bosses.
Houston Methodist’s CEO Marc Boom predicts more hospitals soon will join the effort. Many hospitals and employers were waiting for legal clarification before acting.
“We can now put this behind us and continue our focus on unparalleled safety, quality, service and innovation,” Boom said after the ruling. “Our employees and physicians made their decisions for our patients, who are always at the center of everything we do.”
Learning of the dismissal from USA TODAY, Bridges vowed not to give up. She has initiated a change.org petition that as of Saturday had drawn more than 9,000 signatures and a GoFundMe to pay for the lawsuit that has raised $130,000.
“This doesn’t surprise me,” she said. “Methodist is a very large company and they are pretty well protected in a lot of areas. We knew this was going to be a huge fight and we are prepared to fight it.”
The lawsuit claimed that federal law prohibits employees from being required to get vaccinated without full U.S. Food and Drug Administration approval of the vaccines. Currently, the FDA has authorized the Moderna, Pfizer and Johnson & Johnson vaccines under a special provision for emergencies.
The judge dismissed this argument as well, saying that law does not apply to private employers. He also dismissed an argument that anyone who gets the vaccine is effectively a human subject in an experimental trial.
“The hospital’s employees are not participants in a human trial,” he wrote. “They are licensed doctors, nurses, medical technician, and staff members. The hospital has not applied to test the COVID-19 vaccines on its employees.”
The lawsuit originally was filed in Texas state court but was moved to federal court at Houston Methodist’s request. The federal judge ruled Saturday that Texas state law only protects workers from being fired if they are forced to commit a crime.
The country is reopening. What does the future hold?
The story of the American pandemic has unfolded in three chapters.The first began last January, when the coronavirus emerged and the world was plunged into uncertainty about how covid-19 could be treated, how the virus spread, and when it might be defeated. The second started on the morning of November 9, 2020, when Pfizer-BioNTech announced the extraordinary efficacy of its vaccine. Those results made clear that this pandemic would end not through infection but vaccination. Our goals shifted from merely slowing the spread to beginning immunization as quickly as possible. In America, much of the past half year has been devoted to administering vaccines and gathering evidence on how well they work in the real world.
Earlier this month, the Centers for Disease Control and Prevention ushered in the American pandemic’s third chapter. The agency announced that vaccinated people could go without masks or social distancing indoors and outside, in crowds large and small. It carved out a few exceptions—for hospitals, public transportation, and the like—and noted that people still needed to obey federal and local laws. But the broad message was that vaccinated Americans could resume their pre-pandemic lives. The C.D.C. is an agency known for caution, and its new guidance shocked many public-health experts; just two weeks earlier, it had issued far more restrictive recommendations. During the same period, a survey of nearly six hundred epidemiologists found that more than three-quarters of them believed that indoor mask-wearing might remain necessary for another year or more. Still, immediately after the announcement, a number of states lifted their mask mandates. Others will surely follow, as the pressure to return to normal grows. America is now moving swiftly toward reopening.
Despite the C.D.C.’s early stumbles on communication, masks, and tests, it remains perhaps the world’s preëminent public-health agency. Its recommendations carry unparalleled scientific force in the U.S. and beyond. Ultimately, the C.D.C.’s decision reflects real shifts in the weight of the evidence on several fundamental epidemiological questions: Are the vaccines as effective as they were in the trials? Can they protect us against the coronavirus variants? And do they prevent not just illness but transmission? The answers to these questions give us good reason to think that the pandemic’s newest chapter will be its last. Read The New Yorker’s complete news coverage and analysis of the coronavirus pandemic.
On the first question, the nationwide rollout of covid-19 vaccines has proved, beyond any doubt, that they are astonishingly effective at preventing serious illness, even for the most vulnerable people. So-called breakthrough infections, in which the virus weaves its way around some of an individual’s immune system, do occur. But such infections are extremely rare, and—because a person almost always has some effective antibodies and other immune-system defenses—they usually cause mild or no symptoms. In one study, the C.D.C. examined post-vaccination infections among nearly fifteen thousand nursing-home residents and staff members, and discovered only two covid-19 hospitalizations and one death. Another study, involving half a million health-care workers from around the country, found that getting two shots reduced the risk of a symptomatic infection by ninety-four per cent. Moving forward, we should expect to continue seeing breakthrough infections from time to time—but, for the most part, we shouldn’t worry about them. (At the same time, the covid vaccines have proved exceptionally safe. Few dangerous side effects have been linked to the vaccines from Pfizer-BioNTech or Moderna, and the over-all risk of concerning blood clots after receiving Johnson & Johnson’s vaccine is rare—as of last week, when more than nine million doses had been administered, there were thirty confirmed cases.)
The most striking vaccine-efficacy statistic draws on data shared by state governments. Around a hundred and thirty million Americans are fully vaccinated, and the C.D.C. has said that it has received reports of fewer than fourteen hundredcovid-19 hospitalizations and three hundred deaths among them. This means that, after vaccination, one’s chances of dying of covid-19 are currently about two in a million, with the likelihood of being hospitalized only slightly higher. Statistics reported by hospitals tend to be accurate; still, even if state governments have missed a few cases here and there, the results are staggeringly good. “The evidence on vaccines just keeps getting better and better,” Robert Wachter, a physician and the chair of medicine at the University of California, San Francisco, told me. “When the trial results first came out, I thought, They can’t actually be this good. The real world is always messier than the trials. What we’ve learned since then is that the vaccines are probably even more spectacular than we initially believed.”
The answer to the second question—whether the vaccines work against the major coronavirus variants—is also now clear. Earlier this month, a study conducted in Qatar, where the B.1.1.7 and B.1.351 variants predominate, found that the Pfizer-BioNTech vaccine was ninety-seven per cent effective at preventing severe disease. Vaccines from Moderna and Johnson & Johnson also appear to be highly effective against the variants; in fact, these vaccines are already successfully fighting them here in the United States. The B.1.1.7 variant, which is vastly more contagious than the original virus and caused a devastating surge in the U.K. this past winter, now accounts for three-quarters of new U.S. cases—and yet, largely thanks to vaccination, daily infections in this country have fallen by nearly ninety per cent since their peak in January, and are now lower than at any point in the past eight months. The existence of more contagious variants isn’t a reason to doubt the vaccines but to vaccinate people as quickly as possible.
As for the final question—whether vaccinated people can spread the virus to others, especially unvaccinated people, including children—the evidence is similarly encouraging. Because vaccinated people are unlikely to contract the virus, the vast majority won’t be passing it on. And even the small number of vaccinated people who experience breakthrough infections have much less of the virus circulating in their bodies, and may be less infectious. Real-world data from Israel, which has mounted one of the world’s fastest and most effective vaccination campaigns, is instructive. The country’s progress in immunizing its adults has been linked to significant declines in infections among unvaccinated people; according to one preliminary estimate, each twenty-percentage-point increase in adult vaccination rates reduces infections for unvaccinated children by half. When vaccinated people remove their masks, they pose little threat to others, and they face little peril themselves.
The shift toward reopening is not without risk. The first issue is timing. Less than half of Americans have received even one shot of a covid-19 vaccine, and only around four in ten have been fully vaccinated. This means that the majority of the country remains susceptible to infection and disease. Meanwhile, the pace of vaccinations has slowed: in April, the U.S. was routinely vaccinating about three million people per day, but the daily average is now nearly two million. It’s unclear whether the new guidance will encourage or deter unvaccinated Americans from getting immunized. In a recent survey, unvaccinated Republicans said that they would be nearly twenty per cent more likely to get the shots if it meant that they wouldn’t have to wear a mask anymore. We’ll now find out how they really feel.
Vaccine hesitancy is only part of the picture. Some thirty million Americans—a group larger than anti-vaxxers or the vaccine-hesitant—say that they want to get immunized but haven’t yet done so. Some face language barriers, or fear immigration problems; others have difficulty navigating the health system, or can’t take time off from work. Many of the willing-but-unvaccinated are working-class Americans; four in five don’t have a college degree. The Biden Administration has sent billions of dollars to health centers serving low-income populations, offered tax credits to businesses that provide paid time off for employees to get immunized, and helped assemble thousands of volunteers—known as the covid-19 Community Corps—to assist with vaccine outreach to underserved populations. States, too, are trying to reduce barriers to vaccination, and offering incentives—including payments in Maryland, a lottery in Ohio, and a “Shot and a Beer” program in New Jersey—for residents who remain on the fence. There are, in short, real efforts under way to sway the vaccine-hesitant and make vaccines more accessible.
Still, the new C.D.C. guidance makes these efforts even more urgent. Until now, unvaccinated people have been shielded from high levels of viral exposure by government mandates and social norms that have kept their friends, neighbors, and colleagues masked and distanced, to varying degrees. But, in the coming weeks, those protections will likely erode. For unvaccinated Americans, this could be the most dangerous moment in the pandemic. In most contexts, there is no reliable mechanism for verifying who has and hasn’t been vaccinated. Inevitably, against the C.D.C.’s advice, many unvaccinated people will resume normal life, too, threatening their own health and that of others. When asked how businesses are to know which customers can enter unmasked, Anthony Fauci, the nation’s top infectious-disease expert, told CNN, “They will not be able to know. You’re going to be depending on people being honest enough to say whether they were vaccinated or not.”
“Unvaccinated people are now going to have much higher levels of exposure,” Wachter told me. “That’s especially true in places with lots of community spread and in places where more contagious variants are circulating.” Wachter suggested that the C.D.C. could be making an epidemiological bet. The move “will cause some additional covid cases that otherwise would not have occurred,” he said—but, “if it leads to even a small uptick in vaccination, it will save lives in aggregate.”
Since the start of the pandemic’s second chapter, public-health officials have been working to prevent a catastrophic collision between the ship of reopening and the iceberg of the unvaccinated. By slowing the speed of the ship or shrinking the size of the iceberg, we have sought to reduce the force of the collision. But barring a hundred-per-cent vaccination rate, or something close to it—an outcome that the U.S. was never likely to achieve—a crash of some sort has been inevitable.India’s collision has been titanic—it reopened with a population of more than a billion, even though hardly anyone was vaccinated. In the U.S., the situation is different. Our iceberg has been melting, and we’ve been approaching it slowly. Now we’re taking off the brakes.
The C.D.C. issues guidance, not laws; there are several quantitative measures that states, counties, cities, companies, and individuals can consult in pacing their reopening and squaring the agency’s broad recommendations with local realities. A community’s immunization rate is perhaps the most obvious statistic to track. Experts have argued for meeting a seventy-per-cent immunity threshold before relaxing masking and distancing requirements. No states have got there yet, although some, such as Vermont and Maine, are well on their way. The Biden Administration has said that it hopes to hit the seventy-per-cent target for first shots by the Fourth of July.
Because the vaccines prevent almost all cases of severe covid-19, the number of covid-19 hospitalizations is another good metric to watch. “With vaccines, cases become uncoupled from severe disease,” Monica Gandhi, an infectious-disease doctor at the University of California, San Francisco, who has studied asymptomatic coronavirus transmission, told me. Gandhi was among the first researchers to show that masks protect not just others but wearers, too; when we spoke, before the C.D.C.’s announcement, she said that, in her view, most precautions could end when half of Americans had received their first shot and covid-19 hospitalizations had fallen below sixteen thousand nationally, or about five per hundred thousand people. (At the peak of most flu seasons, the U.S. records five to ten influenza hospitalizations per hundred thousand.) Hospitalizations appear to be falling, unevenly, across the country. However, there are currently thirty thousand Americans hospitalized with covid-19—roughly a quarter of the January peak, but still about twice Gandhi’s threshold.
Herd immunity offers a third benchmark for reopening. The idea is that, once about eighty per cent of the population has been vaccinated or infected, the virus will struggle to spread. Recently, some experts have argued that we might never get to herd immunity because of variants, vaccine hesitancy, and the fact that children under twelve, who make up some fifteen per cent of the U.S. population, are unlikely to be immunized for some time. But the C.D.C.’s recommendation could change the equation. As states lift restrictions and unvaccinated people face higher levels of exposure, more of them are likely to get infected, pushing us closer to the herd immunity threshold. In all likelihood, the U.S. will be able to reach sixty-per-cent vaccination in the coming weeks; meanwhile, perhaps a third of Americans have already been infected. Even assuming significant overlap between the two groups, the combination of vaccination and infection is likely to make it harder for the virus to find new hosts. Marc Lipsitch, the director of Harvard’s Center for Communicable Disease Dynamics, emphasized that, because some parts of the country may reach herd immunity, or something close to it, before others—Connecticut’s current covid-19 immunization rate, for instance, is nearly twice Mississippi’s—unvaccinated adults will face different levels of risk depending on where they live. “There won’t be one national end,” Lipsitch told me. “We’re going to see a fundamental change in terms of what it means to live in this country, but there’s also going to be a lot of local variation.”
Covid-19 deaths give us another way of tracking the pandemic. Experts have argued that the U.S., with a population of three hundred and thirty-two million, should aim for fewer than a hundred coronavirus deaths daily—roughly the toll of a typical flu season. Right now, America is seeing about six hundred covid-19 deaths each day; according to the Institute for Health Metrics and Evaluation, which generates one of the country’s most widely cited pandemic models, that number will likely fall to about a hundred in August. “Things will look very good this summer,” Christopher Murray, the director of the I.H.M.E., told me. “A lot of people will think that we’re done, that it’s all over. But what happens in the fall is the tricky part.” Murray believes that a confluence of factors—the spread of variants, in-person schooling, meaningful numbers of still-unvaccinated people, and the seasonality of the virus—will produce a small winter spike, concentrated in communities with low vaccination rates. It won’t be the apocalyptic surge of New York City in the spring of 2020—or, more recently, those of India or Brazil—but, each week, several thousand unvaccinated Americans could die.
It’s possible, given all this, to imagine a plausible scenario for the conclusion of the American pandemic. The coronavirus disease toll continues to fall throughout the summer. States do away with mask mandates and capacity restrictions; people increasingly return to bars, spin classes, and airports, then to stadiums, movie theatres, and concerts. By midsummer, in communities with high vaccination rates, covid-19 starts to fade from view. In those places, even people who remain unvaccinated are protected, because so little of the virus circulates. But, in other parts of the country, low immunization rates combined with reopening allow the disease to register again. Hospitals aren’t overwhelmed—there’s no need to build new I.C.U.s or call in extra staff—but the collision between ship and iceberg is forceful, and each week thousands of people fall ill and hundreds die. Some victims are vaccine-hesitant; others were unable, for whatever reason, to get vaccinated. Still, perhaps unfairly, these outbreaks come with an aura of culpability: to people in safe parts of the country, the ill seem like smokers who get lung cancer.
In the fall, many unvaccinated children return to school. Scattered infections among them capture headlines, but serious illnesses are exceedingly rare; the overwhelming majority of children remain safe, and, with time, they, too, are immunized. The U.S. approaches something like herd immunity. Some people may still fall ill and die of covid-19—perhaps they are immunocompromised, elderly, or just unlucky—but, by and large, America has gained the upper hand. Meanwhile, in poor nations with few vaccines, the pandemic continues. As crisis wanes in one country, catastrophe ignites in another. Every so often, we learn of a new variant that’s thought to be more contagious, lethal, or vaccine-resistant than the rest; we rush to institute travel bans, only to learn that the variant, or a close cousin, is already circulating in the U.S. and has been largely subdued by the vaccines, as all previous variants have been. In the fall, Americans line up for covid booster shots alongside flu vaccines. The pandemic’s final chapter comes to a close not through official decree but with the gradual realization that covid-19 no longer dominates our lives.
Reopening a country after a pandemic isn’t like flipping a giant switch. It’s more like lighting a series of candles, illuminating one part, then another, until the whole place shines. Many states, counties, cities, and businesses will further loosen their restrictions; others will wait. Communities and individuals will approach the end of the crisis differently, as they’ve approached the rest of it. Some unvaccinated people have already been forgoing precautions; on the other hand, I’ve been vaccinated for months and, since the C.D.C. announcement, have yet to leave my mask behind—whether because of a lingering, irrational fear or simply to avoid dirty looks, I can’t say. Social norms take time to change, even when one of the world’s most respected public-health agencies is telling you to change them.
The pandemic has created not just chaos and suffering but uncertainty. It’s easy, therefore, to be doubtful about the fortunate position in which we seem to find ourselves now. As a physician, I spent the early months of the pandemic caring for covid-19 patients in New York City; they streamed into the hospital day after day, deathly ill. We raced to build covid wards, I.C.U.s, and hospice units. At the time, we had little to offer. There were no proven therapies, and certainly no vaccines. There were weeks when thousands of New Yorkers died, many of them alone in their final moments, while more people were dying across the world. I felt fear, anxiety, and sometimes despair. The scale of the damage—the lives lost, businesses shuttered, dreams shattered, children orphaned, seniors isolated—was crushing, and the path forward was both frightening and unknown.
As good news began to arrive, I greeted it with a blend of guarded skepticism and cautious optimism. First came evidence that outdoor transmission was unlikely. Then we learned that contaminated surfaces rarely spread disease; that some patients can breathe better simply by lying on their bellies; that P.P.E. works; that dexamethasone saves lives. We discovered that immunity lasts many months, perhaps years; that repeat infections are unlikely; and that variants present a surmountable challenge.
Now, study after study, in country after country, has shown that the vaccines are capable of transforming a lethal pathogen into a manageable threat. Examining and reëxamining the vaccine results, I’ve gone through stages, too—caution, hope, and, finally, clarity. We really are that close. The beginning of the end is here.
The Food and Drug Administration cleared the first coronavirus vaccine for emergency use in children as young as 12 on Monday, expanding access to the Pfizer-BioNTech shot to adolescents ahead of the next school year and marking another milestone in the nation’s battle with the virus.
The decision that the two-shot regimen is safe and effective for younger adolescents had been highly anticipated by many parents and pediatricians, particularly with the growing gap between what vaccinated and unvaccinated people may do safely. Evidence suggests that schools can function at low risk with prevention measures, such as masks and social distancing.But vaccines are poised to increase confidence in resuming in-person activities and are regarded as pivotal to returning to normalcy.
“Adolescents, especially, have suffered tremendously from the covid pandemic. Even though they’re less likely than adults to be hospitalized or have severe illness, their lives really have been curtailed in many parts of the country,” said Kawsar R. Talaat, an assistant professor of international health at the Johns Hopkins Bloomberg School of Public Health. “A vaccine gives them an extra layer of protection and allows them to go back to being kids.”
Expert advisers to the Centers for Disease Control and Prevention are scheduled to meet Wednesday to recommend how the vaccine should be used in that age group, and the vaccine can be administered as soon as the CDC director signs off on the recommendation.
In a news briefing Monday evening after the announcement, FDA officials said the Pfizer authorization for 12- to 15-year-olds was a straightforward decision because the data showed that the vaccine was safe and that the response to the vaccine was even better than among the 18- to 25-year-olds who got the shots.
Children rarely suffer serious bouts of covid-19, the illness caused by the coronavirus. But there is no way to predict the few who will become dangerously sick or develop a rare, dangerous inflammatory syndrome. Out of more than 581,000 covid-19 deaths in the United States, about 300 have been people under 18 — a tiny fraction of the total. But that exceeds the number of children who die in a bad flu season.
Children appear to be less efficient at spreading the virus, although their role in transmission is still not fully understood — another reason for pediatric vaccinations.
Clinicians also worry that with a new virus with many unknowns, the possibility exists for long-term impacts of infection, even from the mild or asymptomatic courses of illness common among children.
The Pfizer-BioNTech vaccine, already authorized for adolescents 16 and older, was the first to be tested in younger adolescents. The FDA’s decision will provide a potential path for other vaccine-makers to follow, most of which have launched or plan to initiate trials of their vaccines in teenagers and younger children.
The agency based its authorization on a trial of nearly 2,300 adolescents between 12 and 15 years old, half of whom received the same two-shot regimen shown effective and safe in adults. Researchers took blood samples and measured antibody levels triggered by the shots and foundstronger immune responses in the teens than those found in young adults. There were 16 cases of covid-19 in the trial, all of them among adolescents who received a placebo, suggesting the regimen offered similar protection to younger recipients as it does to adults.
Robert W. Frenck Jr., the researcher who led the adolescent trial at Cincinnati Children’s Hospital Medical Center, said the study was designed to test whether it triggered immune responses, not whether it prevented disease. But because of the number of children who became ill in the placebo arm of the trial, it also became evident the vaccine offered robust protection.
“That really points out how much covid there is in the adolescent community,” Frenck said.
The data has not been published or peer-reviewed, but Kathryn M. Edwards, a pediatric infectious-disease specialist at Vanderbilt University Medical Center, said the results announced by Pfizer were “pretty exciting — it looked very effective and the immune responses were really good.”
Edwards said she is comfortable the benefits of vaccinations are clear among teens, noting that while children, in general, are at lower risk of severe covid-19 than adults, older adolescents seem to be more like adults in their risk for covid-19 than the very youngest children.
Audrey Baker, 15, and Sam Baker, 12, rolled up their sleeves for shots in the Pfizer-BioNTech trial at Cincinnati Children’s Hospital Medical Center. Audrey said she had no hesitation about signing up, and misses little things about how life used to be — eating out in restaurants and seeing family.
“I just trusted the science,” Audrey said. “I knew it was tested in adults. I was really just joining, hoping that maybe I could get vaccinated and help out science.”
Sam said he was more hesitant, in part because participating meant many follow-up lab tests. But he decided to do it and thinks he may have gotten the vaccine in the trial because he developed a headache and fever after his second dose.
Their mother, Rachel Baker, said she felt relief because of Sam’s symptoms.
“The biggest benefit has been that I feel a weight off my shoulders,” Rachel said. “We haven’t changed how we do anything. … We’re still masking, we’re still social distancing, but we’re a bit calmer about it all.”
H. Cody Meissner, a pediatrician at Tufts Medical Center and a member of an external advisory committee to the FDA, said he thinks a pediatric vaccine is needed. But he said he would like to see more safety data because the messenger RNA technology at the core of vaccines from Pfizer-BioNTech and the biotechnology company Moderna does not have a long, established safety record, and its first large-scale use began in December.
Meissner abstained from the December vote that overwhelmingly recommended authorization of the Pfizer-BioNTech vaccine for people 16 and older, because he thought the vaccine should be authorized in people 18 and older.
“For those who are eager to get it, it’s important for them to understand that this is very rarely a severe disease in young adolescents, number one, and this is an entirely new vaccine,” Meissner said. “I just don’t want people to get too swept up in fear of hospitalization and death from covid-19 for the first few decades of life.”
But many other physicians take comfort knowing that 250 million shots of messenger RNA vaccine have been given in the United States alone.Serious side effects, such as a risk of anaphylaxis, are extremely rare. Because the trial in teens was an “immune bridging” trial designed to test whether the vaccine triggered immune responses similar to those in adults, researchers did not need to recruit tens of thousands of people to see if those who received a vaccine were protected against illness. The immunebridging technique is commonly used to expand access to vaccines that have been proved effective and safe to adolescents or other populations.
The expansion of eligibility to children will probably ignite debates in families about when to get vaccinated, and among policymakers about whether it should be required.
Dorit Reiss, a law professor focused on vaccine policy at the University of California Hastings College of Law, said she thinks it is unlikely children will be mandated to receive a coronavirus shot until the vaccines win full approval and not just emergency use authorization.
She predicted that acceptance of the vaccine will evolve as more children are vaccinated and depend on the state of the pandemic. She noted that when vaccines are introduced, the rollout often starts slowly before accelerating.
“Nervousness about a new vaccine is normal, especially when it’s for kids,” Reiss said. “Parents that are nervous now might feel different in a few months, once their friends’ kids have gotten vaccinated. And the views of the kids are also going to matter — if teens are going to think this is going to make their lives easier.”
Opening up vaccinations to children may sharpen a debate unfolding globally about the equity of vaccine access. Talaat said that while she can’t wait for her kids to have access to a vaccine, she is troubled by the global inequities as high-risk front-line workers or older people still don’t have access to vaccines in countries where the coronavirus is out of control.
Moderna announced Thursday that an initial analysis of its teen trial found its vaccine was 96 percent effective among participants who received at least one dose. Moderna is in discussions with regulators about the data. Pfizer-BioNTech and Moderna are testing their vaccines in children as young as infants. Johnson & Johnson is planning pediatric trials of its single-shot vaccine.
Trials in younger children are expected to take longer, because researchers must step down gradually in age and determine a safe and effective dose. William Gruber, senior vice president of vaccine clinical research and development at Pfizer, said data from tests in children as young as 2 years old may be available by September or October, with data on children as young as 6 months possible by the end of the year.
Within each age category, a separate risk-benefit assessment may take place. In the youngest children, given the low risk from the coronavirus, side effects may figure more prominently into the analysis, for example. Researchers may end up choosing a lower dose of vaccine. The understanding of children’s role in transmission may also evolve and help guide vaccine use and public policy.
“We are proceeding carefully, cautiously,” Edwards said. “We’re using the same rigid guidelines we use in all vaccines, and we take this very seriously. I think as time goes on and more information becomes available, some of the questions may be easier to address.”

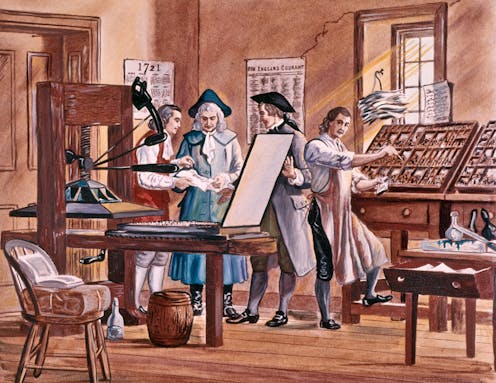
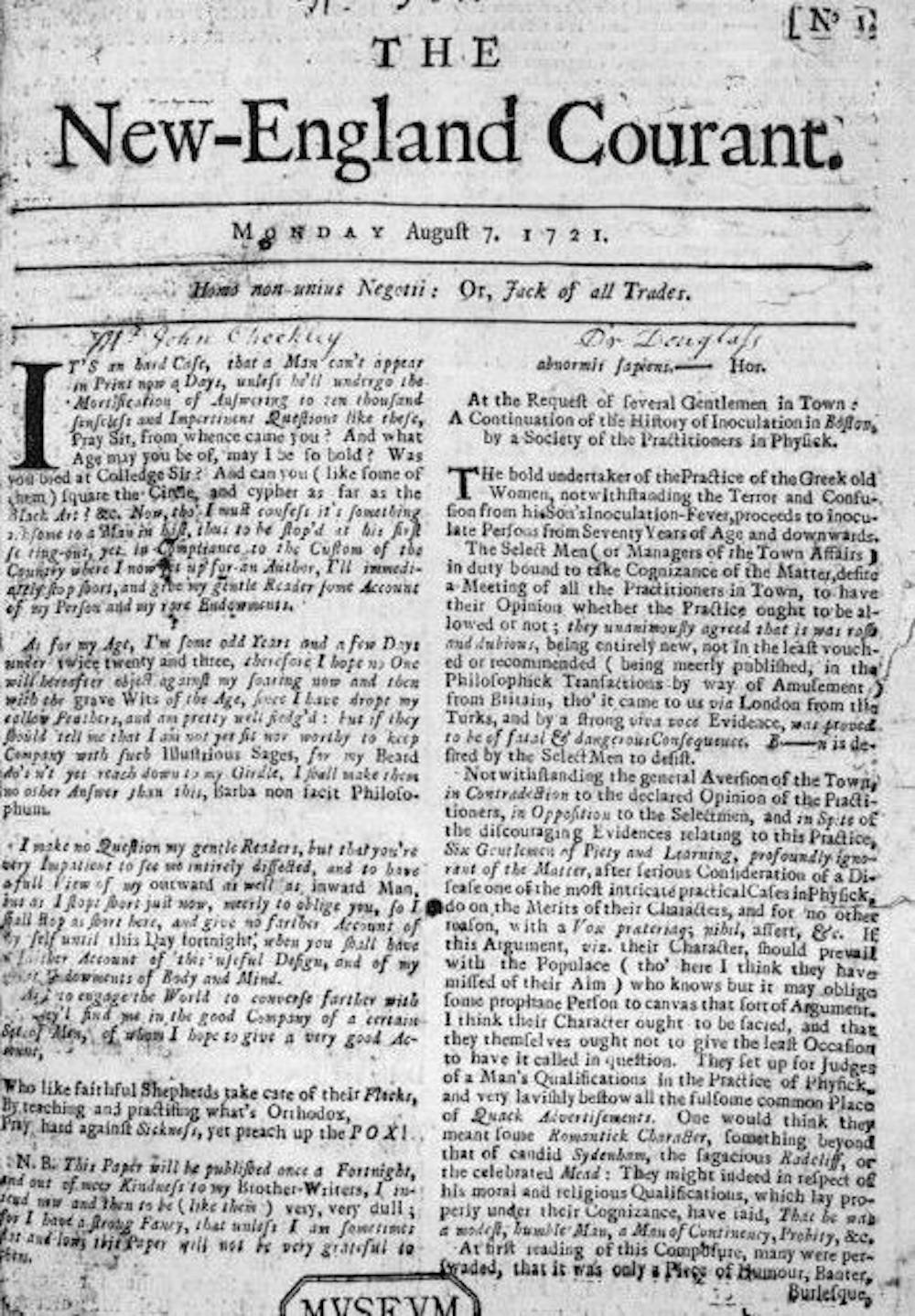



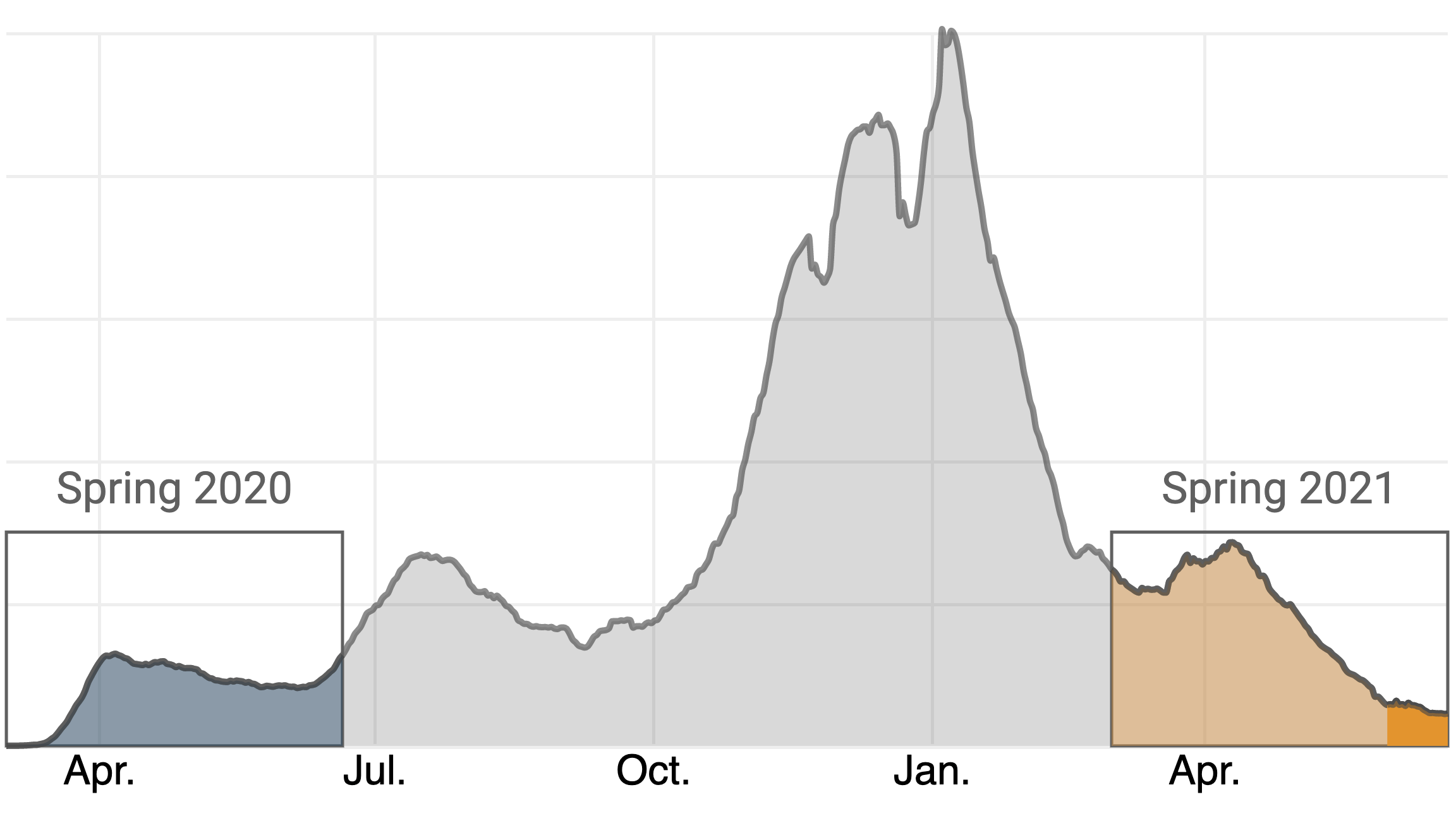





{kind=link}