President Trump repeated baseless claims at the final presidential debate that the coronavirus “will go away” and that the U.S. is “rounding the turn,” while Joe Biden argued that any president that has allowed 220,000 Americans to die on his watch should not be re-elected.
Why it matters: The U.S. is now averaging about 59,000 new coronavirus infections a day, and added another 73,000 cases on Thursday, according to the Covid Tracking Project. The country recorded 1,038 deaths due to the virus Thursday, the highest since late September.
What they’re saying: “More and more people are getting better,” Trump said. We have a problem that’s a worldwide problem. This is a worldwide problem. But I’ve been congratulated by the heads of many countries on what we’ve been able to do … It will go away and as I say, we’re rounding the turn. We’re rounding the corner. It’s going away.”
Trump later disputed warnings by public health officials in his administration that the virus would see a resurgence in the winter, claiming: “We’re not going to have a dark winter at all. We’re opening up our country.”
Biden responded: “Anyone responsible for that many deaths should not remain as president of the United States of America.”
“What I would do is make sure we have everyone encouraged to wear a mask all the time. I would make sure we move in the direction of rapid testing, investing in rapid testing.”
“I would make sure that we set up national standards as to how to open up schools and open up businesses so they can be safe and give them the wherewithal, the financial resources, to be able to do that.”
The bottom line:Biden and Trump are living in two different pandemic realities, but Biden’s is the only one supported by health experts.
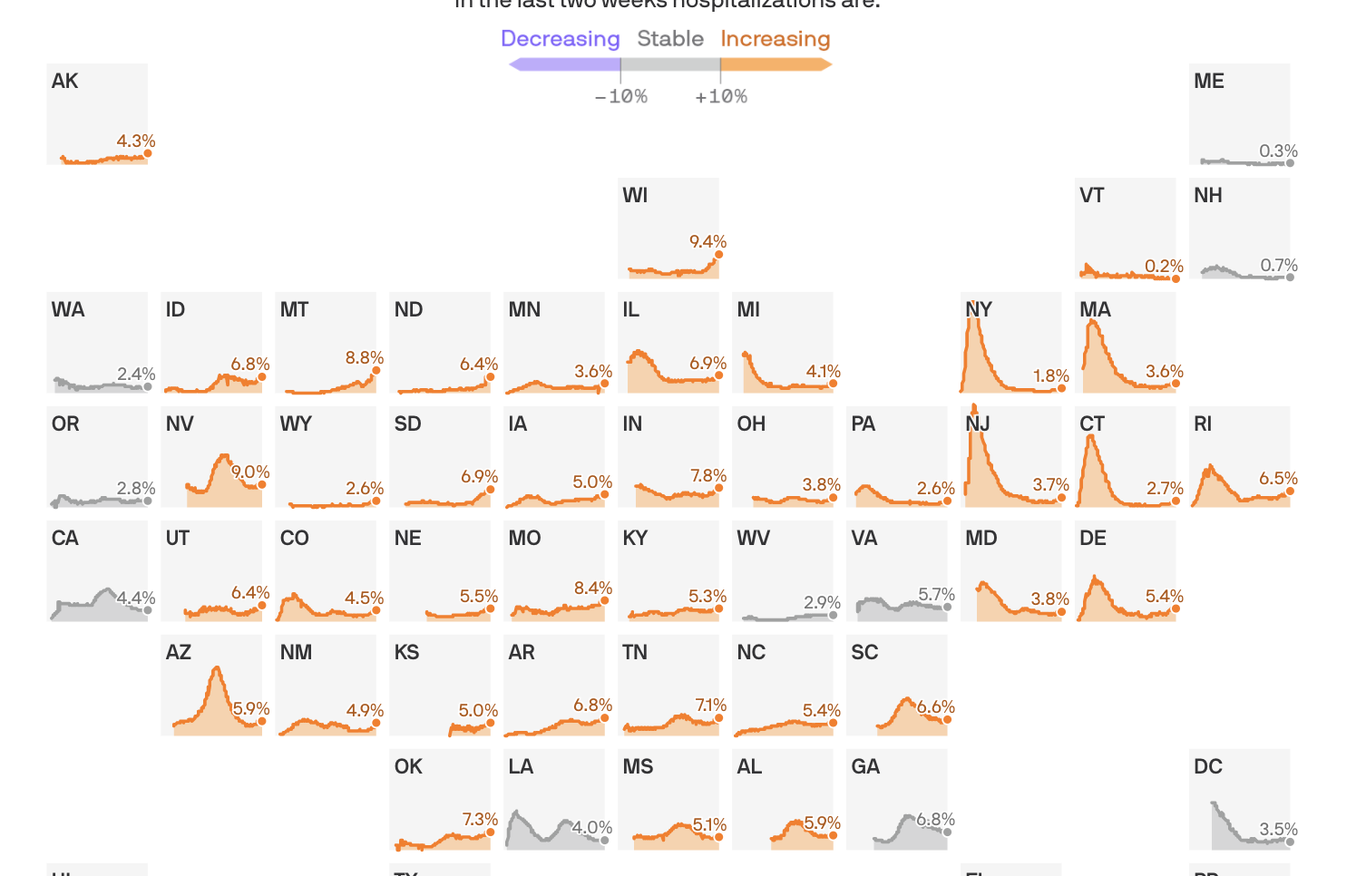
Share of hospital beds occupied by COVID-19 hospitalizations
States shown from first date of reported data, from March 17 to Oct. 17, 2020
In the last two weeks hospitalizations are:
Coronavirus hospitalizations are increasing in 39 states, and are at or near their all-time peak in 16.
The big picture: No state is anywhere near the worst-case situation of not having enough capacity to handle its COVID-19 outbreak. But rising hospitalization rates are a sign that things are getting worse, at a dangerous time, and a reminder that this virus can do serious harm.
By the numbers: 39 states saw an increase over the past two weeks in the percentage of available hospital beds occupied by coronavirus patients.
Wisconsin is faring the worst, with 9.4% of the state’s beds occupied by COVID patients.
Sixteen states are at or near the highest hospitalization rates they’ve seen at any point in the pandemic.
Yes, but: The all-time peak of coronavirus hospitalizations happened in the spring, when 40% of New Jersey’s beds were occupied by COVID patients. Thankfully, even the the worst-performing states today are still a far cry from that.
Between the lines:These numbers, combined with the nationwide surge in new infections, confirm that the pandemic in the U.S. is getting worse — just as cold weather begins to set in in some parts of the country, which experts have long seen as a potentially dangerous inflection point.
They also suggest that most parts of the country won’t need to pause or scale back non-coronavirus treatments, as hospitals did in the spring when no one was quite sure how bad things could get.
In rural areas, however, even a modestly sized outbreak can strain local hospital capacity.
As a new wave of coronavirus cases hits the U.S. and Europe, governments are shifting away from total shutdowns toward more geographically targeted lockdowns to stifle the virus’ spread.
Why it matters:Precision shutdowns can slow emerging outbreaks while lessening the overall economic impact of the response. But they risk a backlash from those who are targeted, and may not be strong enough to keep a highly contagious virus under control.
Driving the news: New York City tried to control a flare-up of new coronavirus cases this month by instituting partial shutdowns on a neighborhood-by-neighborhood basis, curtailing economic and social activity in areas harder hit by the virus while continuing reopening elsewhere.
British Prime Minister Boris Johnson on Monday instituted a similar response for the U.K., putting in place a three-tier escalating system of lockdowns on a city or regional basis.
“We don’t want to go back to another national lockdown,” Johnson told the British Parliament. But “we can’t let the virus rip.”
What’s new: Some early research indicates more-targeted lockdowns can effectively smother outbreaks while leaving broader city and regional economies mostly intact.
A paper published by a team of economists in July found a more precise shutdown focused on places where viral spread was most common could have reduced economic losses in New York by as much as 50% compared to a uniform lockdown.
As long as new outbreaks are still in the relatively low flare-up stage, targeted lockdowns can efficiently cut off the oxygen to new spread. That seems to be the case in New York, where data released on Thursday indicates transmission has slowed in six of the ZIP codes that had been the focus of targeted lockdowns.
Yes, but: Individuals move around a city, and some epidemiologists worry that over time cases will break out of targeted lockdown areas and spark a wider outbreak.
A preprint paper published in August found people were willing to travel outside of lockdown areas to get services they needed, potentially spreading the virus along the way.
That was especially true for religious services. The paper found that during March, even as the total number of visits to churches declined, between 10% and 30% of churches nationwide saw increases in attendance. Those who were motivated to go simply went to churches outside of restricted areas.
The small, seemingly geographically isolated outbreaks officials are focusing on may actually be the first signs that a city or region’s control measures simply aren’t working. As a result, “targeted measures can end up chasing the outbreak wider and wider, to the point where restrictions are equivalent to a broader blanket policy,” epidemiologist Adam Kucharski told Wired.
What to watch:A targeted lockdown is inevitably going to appear to single out specific groups of people, which risks creating a backlash that can undermine public support for long-term control measures.
That’s already been the case in New York, where Orthodox Jewish communities have taken to the street to protest targeted lockdowns in their neighborhoods.
In New York’s Queens borough, stores and restaurants in one mall have been ordered closed, while those in an adjacent mall are still open, simply because of which side of the line they fall on.
The experience of COVID-19 has already been a deeply unfair one, with both the direct health effects and indirect economic costs falling on those who can least afford it, and focused lockdowns will exacerbate that unfairness.
The bottom line:Targeted lockdowns can throttle the virus while minimizing economic damage, at least in the short term. But one thing we’ve learned is that if COVID-19 gets out of control in one place, it may be only a matter of time before it ends up everywhere else.
Dueling petitions about what to do about COVID19 — the Great Barrington Declaration and the John Snow Memorandum — are circulating online amongst physicians, public policy makers, and academics. I am not against policy statements, consensus building, or even petitions, but both of these documents trouble me. They are the dropping anchors when we should be open to sailing where the wind blows.
Let’s start with the obvious. SARS-CoV-2 kills people. When infected, older people and those with serious comorbidities are more likely to die than younger people. This age-gradient (extra risk of death among older people) is steep. At the same time, dramatic interventions to halt SARS-CoV-2 — such as closing schools, business, travel, economic activity, normal hospital functions — also kills people. Some of these deaths occur immediately — a person with a heart attack is dissuaded from seeking care, an uncontrolled tuberculosis epidemic in a low income nation, or even depression and suicide — and some of the downsides take a long time to kill: loss of upward mobility and economic potential for the next generation will shorten lives.
Downsides to lockdowns can also be hard to predict. Harms may include destabilizing democratic governments, civil unrest, and political turmoil. The goal of policy in each and every place on earth is to minimize the total harm to the people who live there. It may vary by place and even moment based on viral spread, age of population, safety nets (or lack there-of), and a number of other factors, including values and preferences.
First, consider the Great Barrington Declaration. It’s just 540 words long, and outlines a strategy of focused protection. Based on the idea that the risk of death varies dramatically with age, it proposes we shield and protect the vulnerable while allowing the young, and others at lower risk, to get on with life as normally as possible. It offers some ideas about how to guard nursing homes, which have experienced massive causalities, and endorses simple measures like handwashing. It nods to the idea that the herd immunity threshold (fraction of people in a population who have become immune before viral spread abates) is not a fixed value: it depends on the way in which populations mix and interact and on simple measures we choose to take, such as improved hygiene. It recommends that schools, universities, bars, and restaurants be allowed to open fully.
Limitations to the statement are its lack of guidance as to who exactly the vulnerable are, how they should shield themselves, and the fact that it lumps together very different things — such as bars and schools. Open bars can be replaced with drinking beers in the backyard with a friend seated at a distance with little loss of pleasure, but education, particularly for the poor, is one of the few ladders left in American society for a better life, a place to feed children, and a vehicle for detecting abuse. Another limitation is its lack of acknowledgement that in moments of explosive spread, temporary measures likely need to be taken to prevent, for example, hospitals from overflowing. Surely, policy responses must depend on the specifics of the time and place.
The John Snow Memorandum was filed in response. It’s longer, at 930 words. It calls Great Barrington’s suggestions to achieve immunity through naturally occurring infections a “dangerous fallacy unsupported by scientific evidence.” Instead it advocates for continued restrictions, along with social programs to minimize the harms of these restrictions. Signers believe this would lower viral spread to very low levels where contact tracing can be utilized to eliminate outbreaks. Finally, the strategy ends when we have an effective vaccine, which it predicts will occur in the coming months.
Limitations to the Snow memorandum include: How exactly will one create social programs to minimize the harms, and what exactly will those programs look like? What will you do in places like the U.S. where even basic economic stimulus talks have stalled? Millions of people are entering poverty in this country, and many more may face starvation globally. How precisely and quickly will you help them? Those who criticize the Barrington authors for not providing a plan to protect the vulnerable from the virus, must criticize the Snow authors for not explaining how they will shield the vulnerable from the harms of restrictions. Additionally, calling for contact tracing is easy, but practically, this faces severe limitations in a nation like the U.S. when many individuals contacted are reluctant to share information. Here too the Snow memorandum falls short on specifics.
The declaration and memorandum are both online and taking signatures, but is this how complex policy should be decided? I find the idea that the fate of the globe will hinge on who garners the most signatures to be Kafkaesque.
Worse, the dueling petitions further divide us, when we should be talking together and working together. It does not escape me that many forces seek to tie these petitions to the Republican and Democratic parties — a dangerous but growing movement to equate pandemic policy with politics.
Signing these petitions may already be a form of identity or virtue signaling, letting others in our political circles know that we are on the virtuous team. Moreover, having signed them, we may be less likely to be willing to change our mind: To think one moment “we ought to open universities,” and the next moment, “let’s consider alternative policies, if hospitalizations rise.”
Instead of these divisive petitions, surely there are things we can all agree to. There is a hierarchy of importance to activities and events in life. Bars, strip clubs, conferences for work — fall on the low end. Schools for young kids, particularly public schools in poor or minority communities, and hospitals are among the most important. There are simple interventions that we can test in controlled trials and implement in the meantime, such as face-shields, plexiglass barriers, widespread hand sanitizer, and masks. We must prioritize schools over bars, and policy must remain individualized (to specific nation/state/county and local preferences) and fluid — able to scale up and down, as we balance the harms of the virus with the harms of closure.
Finally, we have to separate rules from behavior. You can allow restaurants to open, but it won’t help the economy if no one eats there. And, you can close everything, but you won’t slow the spread if people have backyard barbecues with dozens of people. What are the best ways to encourage desired behavior? That’s a harder problem.
Finally, there is no one-size-fits-all solution. What works in a remote island nation with a strong safety net, that can cut off contact with the rest of the world, may not work in a nation with hundreds of millions who face the threat of starvation if the economy grinds to a halt.
We need fewer pompously named petitions and instead, a COVID policy response that engages with people who hold views and perspectives different than our own; which acknowledges the lives lost from the virus and lost through the response; which is nimble and responsive to new data, new facts, and new perspectives; which engages values and preferences and local norms and the messy reality of the world as it is, not as we wish it were.
And, almost most importantly, one which is bipartisan, spanning political ideology, which unites rather than divides us.
More Americans are now in the hospital with Covid-19 than at any other point since late August, causing some states to nearly run out of hospital beds, as coronavirus infections continue to increase nationwide ahead of a potential end-of-year surge.
KEY FACTS
Some 37,048 coronavirus patients were hospitalized as of Wednesday, the highest level in almost two months according to new data from the COVID Tracking Project, though total hospitalizations are still below their mid-April peak of almost 60,000.
Among hospitalized patients, 7,156 were in ICUs and 1,776 are currently on ventilators — both of those numbers have increased slightly in recent weeks.
Texas leads the nation with more than 4,000 patients in hospitals, followed by California and Florida, though all three states’ hospital counts declined since the summer.
Hospitalizations and new cases soared in Wisconsin over the last month, and officials opened an emergency field hospital near Milwaukee this week as medical centers across the state fear they will run out of space.
Hospital numbers are also on the rise across other parts of the Midwest and South: Missouri reported a new record this week, and levels in Kentucky and Ohio are both within striking distance of their summertime peaks.
BIG NUMBER
217,933. That’s the total number of Americans who have died from Covid-19, according to figures from Johns Hopkins University. Daily fatalities are still below their peak in April, but they remain steady at more than 700 per day.
KEY BACKGROUND
When the coronavirus first surged in the New York City area, some hospitals nearly buckled under the pressure, contending with thousands of sick patients and inadequate protective equipment. Covid-19 cases gradually decreased nationwide but never fully subsided. The West Coast and Deep South dealt with cascading upticks after states loosened coronavirus restrictions during the summer, and the Midwest and small states like South Dakota are now struggling to open up more hospital capacity as new infections surge. Some experts warncases could spike yet again over the fall and winter, straining the nation’s medical system and making it tough to get sick patients the medical attention they need.
CRUCIAL QUOTE
“When we see an overwhelming number of patients get infected, a lot of them are going to need hospitalization and support,” Dara Kass, a New York-based emergency room physician, told CBS News on Thursday. “We’re seeing hospitals in Wisconsin be overwhelmed with no ICU beds … This is a big concern of those of us who are looking to prevent as many deaths as possible.”
Dr. Anthony Fauci, the nation’s top infectious disease expert, tells CBS Evening News anchor and managing editor Norah O’Donnell that Americans need to “double down” on mask-wearing and social distancing to help control a surge in new coronavirus cases.
He also spoke about President Trump’s recovery from COVID-19, progress towards a vaccine, and how the pandemic will affect this year’s holiday gatherings. Watch the full interview.