The Centers for Medicare & Medicaid Services (CMS) released its 2022 Inpatient Prospective Payment System (IPPS) proposed rule this week. Overall, the rule brings good news for hospitals: Medicare reimbursement rates are slated to increase by 2.8 percent,resulting in a $2.5B payment boost to the industry.
In another win, hospitals will no longer be required to disclose their contract terms with Medicare Advantage (MA) insurers. Hospitals had previously been mandated by the 2021 rule to report median, payer-specific, negotiated charges for MA insurers on their Medicare cost reports. Medicare’s goal was to use this data to create a new, market-based, inpatient reimbursement methodology—an effort which has also been tabled, at least for now.
Led by the American Hospital Association, hospitals have been embroiled in lengthy legal challenges over a variety of CMS price transparency requirements, maintaining they are neither beneficial for consumers, nor helpful in lowering healthcare costs.
It’s too early to tell whether this step back from price transparency, which was a key goal of the Trump administration, signals anything about the Biden administration’s priorities; it’s possible CMS may just be slowing down the effort in the wake of the pandemic.
Other highlights of the proposed rule includefunding 1,000 more residency slots over the next five years, and extending payments for COVID-19 treatments to the end of 2022, as CMS expects COVID patients will need care beyond the duration of public health emergency. The agency also proposed several changes to its readmissions and other value-based purchasing programs, to ensure hospitals aren’t penalized by COVID-related impacts on quality measures.
Comments on the proposed rule are due by June 28th.
In his first address to a joint session of Congress, delivered on the eve of his 100th day in office, President Biden laid out his vision for two major legislative proposals to follow the $1.9T stimulus package he signed into law last month.
The first, described as an “infrastructure” bill, focuses largely on investing in transportation-related improvements, building projects, and “green” upgrades to the nation’s energy grid, along with a $400B investment in home-based care for the elderly and people with disabilities—which amounts to over 17 percent of the package’s $2.3T price tag.
The second, which he unveiled in Wednesday’s speech, is a $1.8T “families” bill, is largely aimed at expanding childcare subsidies, early childhood education, paid family and medical leave, and educational investments. Included in that package is $200B to extend the temporary subsidies—approved as part of last month’s stimulus law—for those seeking health insurance coverage on the individual marketplaces created by the Affordable Care Act (ACA).
Notably absent from either proposal were two categories of healthcare reform that received much focus and airtime during last year’s election campaign: reducing the cost of prescription drugs and lowering the eligibility age for Medicare to 60 or below. Given the closely divided makeup of the new Congress, and the relatively moderate position staked out by the Biden administration on healthcare issues (with a bias toward bolstering the ACA rather than pursuing sweeping changes), we’re not surprised to see the Medicare expansion go unmentioned.
But the bipartisan popularity of lowering prescription drug costs seems like a missed opportunity for Biden, who encouraged the Congress to return to it separately, later in the year. We’ll see. For now, with even some Democrats expressing concern about the $4.1T price tag of Biden’s proposals, we would be surprised if all $600B of the healthcare-related spending makes it to the final legislation. In particular, our guess is that some portion of the home-care spending will get traded away in favor of other components of the package. Expect negotiations to be intense.
The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
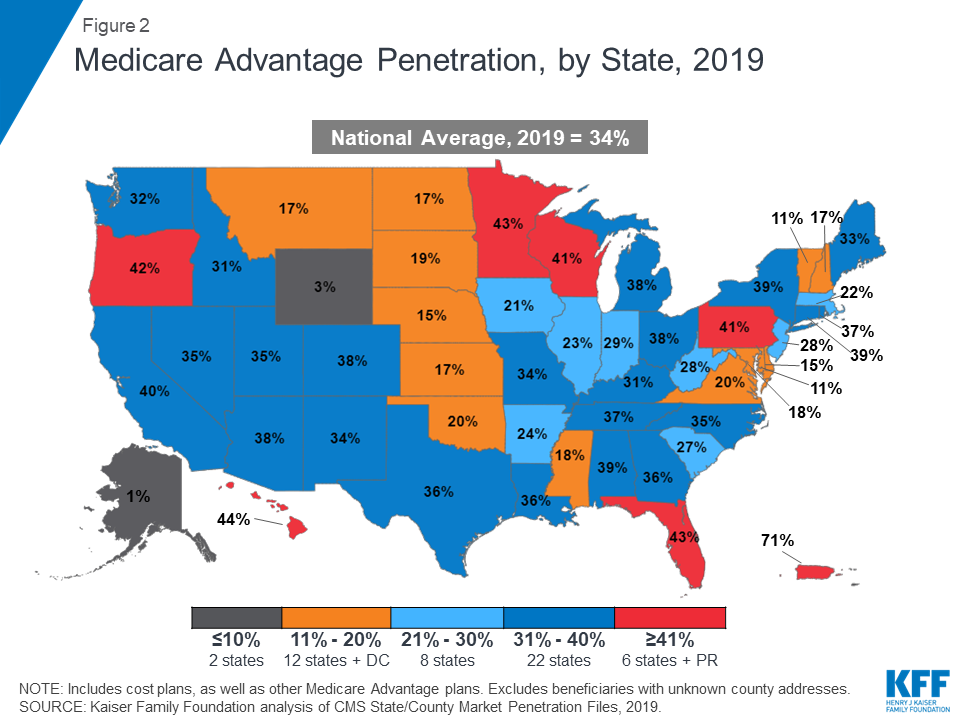
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers (about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services. The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
Figure 1: MA HMO Out-of-Network Payments
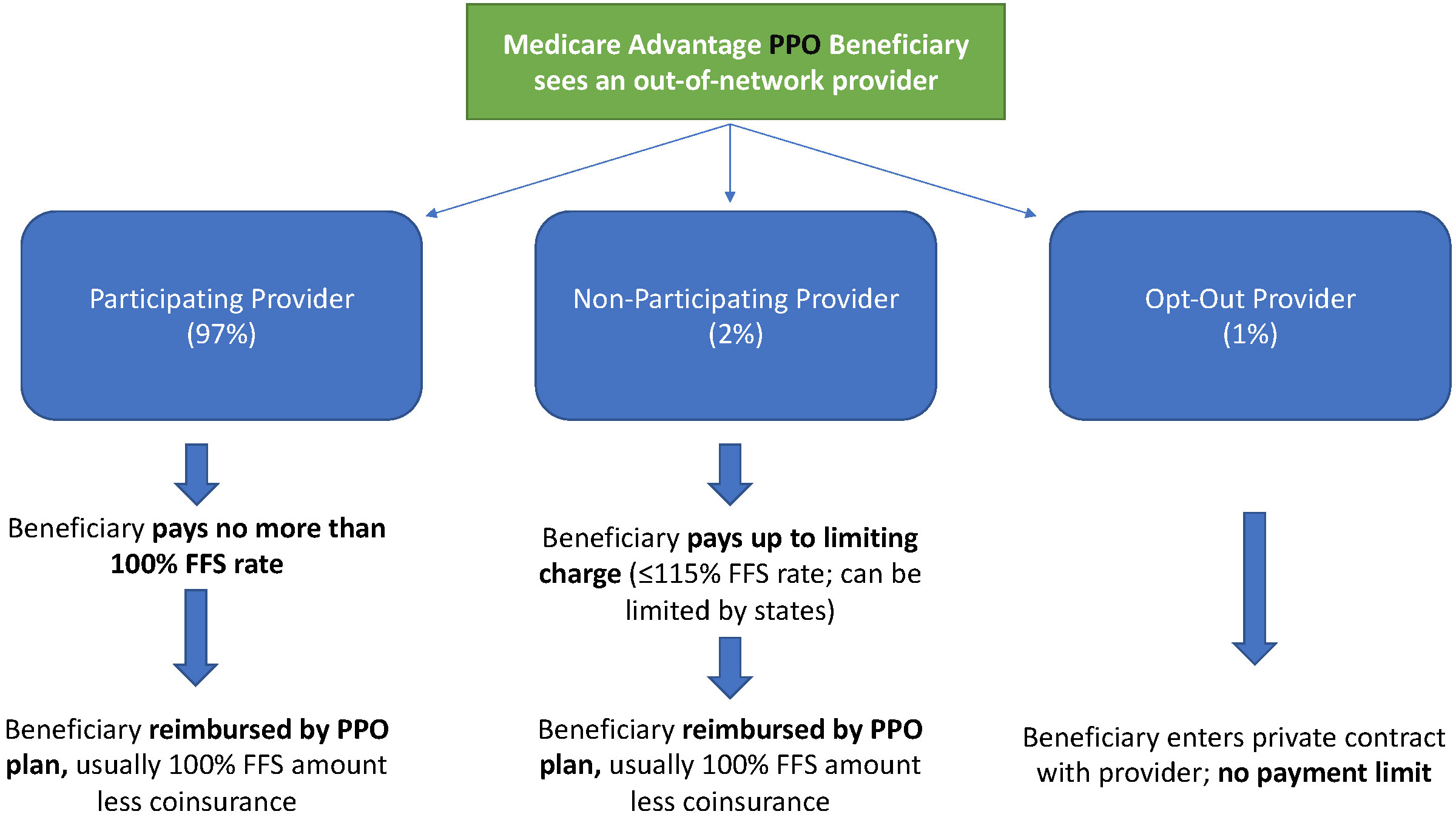
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (See Figure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
In a vote of 384-38, the House on Tuesday passed a bill that eliminates the 2% cut to Medicare payments until the end of 2021. However, the bill proposes to offset the change by increasing the sequester cuts in 2030.
WHY THIS MATTERS
The cuts were triggered by a federal budget sequestration.
Hospitals, physicians and other providers protested the 2% cuts as coming at a time when they were struggling financially and clinically to handle the COVID-19 pandemic.
The bill also makes several technical changes to the rural health clinic provisions that were included in the Consolidated Appropriations Act. Specifically, the CAA required that the payment rate for RHCs, including provider-based RHCs certified after Dec. 31, 2019, to be capped at $100 per visit, starting from April 1, 2021.
This rate will increase over time based on the Medicare Economic Index, but will remain well below typical provider-based RHC rates. The bill would correct the Dec. 31, 2019, date to Dec. 31, 2020, and include both Medicare-enrolled RHCs located in a hospital with less than 50 beds and RHCs that have submitted an application for Medicare enrollment as of this date, according to the AHA.
THE LARGER TREND
Last year, Congress paused the 2% Medicare cuts, but they were to resume on April 1.
The Centers for Medicare and Medicaid Services instructed Medicare administrative contractors to hold all claims with dates of service on or after April 1 for a short period until potential legislation was enacted.
In March, the House passed the bill to delay the cuts, and the Senate approved it later that month, but with an amendment to delay through December 31 and ensure that the cost of the delay is paid for.
PROVIDER REACTION
Providers have reacted positively to the news.
American Hospital Association president and CEO Rick Pollack said, “Even though our country is making great progress by vaccinating millions of people a day, it is clear that this pandemic is far from over and that there is an urgent need to keep hospitals, health systems and our heroic caregivers strong.”
American Medical Association president Dr. Susan R. Bailey said, “The Senate and House, Democrats and Republicans, have overwhelmingly acknowledged that cutting Medicare payments during a pandemic is ill-conceived policy. Physician practices are already distressed, and arbitrary 2% across-the-board Medicare cuts would have been devastating.”
America’s Essential Hospitals SVP of policy and advocacy Beth Feldpush said, “Extending the moratorium through the end of this year provides much-needed relief for essential hospitals, which continue to face heavy financial pressure from their frontline response to COVID-19. The sequester would weaken the ability of our hospitals to care for the communities of color that have suffered disproportionately from the pandemic.”
The Biden administration has proposed giving rehabilitation facilities a 2.2% payment increase for the 2022 federal fiscal year that starts in October.
The payment rate outlined in a proposed rule released late Thursday is slightly below the 2.4% that CMS gave rehab facilities for the 2021 federal fiscal year. CMS proposed in a separate rule a 2.3% increase for payments to inpatient psychiatric facilities as well.
Both payment rules also give updates on outlier payments, which help facilities deal with the costs of treating extremely costly beneficiaries.
For rehab facilities, CMS proposes to maintain outlier payments to 3% of the total facility payments for fiscal 2022, which begins on Oct. 1.
CMS also aims to keep the outlier payments for psychiatric facilities at 2% for 2022.
A major change for both rules is a new addition aimed to track coverage of COVID-19 vaccinations among healthcare personnel.
CMS also wants to add vaccination coverage among healthcare personnel as a measure to the quality reporting program for psychiatric facilities. The program outlines quality metrics that facilities need to meet.
“This measure would be reported using the COVID-19 modules on the [Centers for Disease Control and Prevention’s] National Healthcare Safety Network web portal,” a fact sheet on the psychiatric payment rule said.
The agency also is proposing a similar measure for rehab facilities to report any vaccinations of healthcare personnel for COVID-19.
“This proposed measure is designed to assess whether [IRFs] are taking steps to limit the spread of COVID-19 among their [healthcare personnel], reduce the risk of transmission within their facilities and help sustain the ability of [rehabilitation facilities] to continue serving their communities through the public health emergency and beyond,” a fact sheet on the rehab rule said.
In the rehab facility rule, CMS also asked for comments on how to improve health equity for all patients.
CMS is seeking comments on whether to add more measures that address patient equity in standardized patient assessment data elements, which must be collected by facilities after post-acute care.
The agency also wants comments on ways to attain health equity for psychiatric facilities as well.
“CMS is committed to addressing the significant and persistent inequities in health outcomes in the United States through improving data collection to better measure and analyze disparities across programs and policies,” the agency said in a fact sheet.
There’s widespread agreement that it’s important to help older adults and people with disabilities remain independent as long as possible. But are we prepared to do what’s necessary, as a nation, to make this possible?
That’s the challenge President Joe Biden has put forward with his bold proposal to spend $400 billion over eight years on home and community-based services, a major part of his $2 trillion infrastructure plan.
It’s a “historic and profound” opportunity to build a stronger framework of services surrounding vulnerable people who need considerable ongoing assistance, said Ai-jen Poo, director of Caring Across Generations, a national group advocating for older adults, individuals with disabilities, families and caregivers.
It comes as the coronavirus pandemic has wreaked havoc in nursing homes, assisted living facilities and group homes, killing more than 174,000 people and triggering awareness of the need for more long-term care options.
“There’s a much greater understanding now that it is not a good thing to be stuck in long-term care institutions” and that community-based care is an “essential alternative, which the vast majority of people would prefer,” said Ari Ne’eman, senior research associate at Harvard Law School’s Project on Disability.
“The systems we do have are crumbling” due to underfunding and understaffing, and “there has never been a greater opportunity for change than now,” said Katie Smith Sloan, president of LeadingAge, at a recent press conference where the president’s proposal was discussed. LeadingAge is a national association of more than 5,000 nonprofit nursing homes, assisted living centers, senior living communities and home care providers.
But prospects for the president’s proposal are uncertain. Republicans decry its cost and argue that much of what the proposed American Jobs Plan contains, including the emphasis on home-based care, doesn’t count as real infrastructure.
“Though this [proposal] is a necessary step to strengthen our long-term care system, politically it will be a challenge,” suggested Joseph Gaugler, a professor at the University of Minnesota’s School of Public Health, who studies long-term care.
Even advocates acknowledge the proposal doesn’t address the full extent of care needed by the nation’s rapidly growing older population. In particular, middle-income seniors won’t qualify directly for programs that would be expanded. They would, however, benefit from a larger, better paid, better trained workforce of aides that help people in their homes — one of the plan’s objectives.
“This [plan] isn’t everything that’s needed, not by any step of the imagination,” Poo said. “What we really want to get to is universal access to long-term care. But that will be a multistep process.”
Understanding what’s at stake is essential as communities across the country and Congress begin discussing Biden’s proposal.
The services in question.Home and community-based services help people who need significant assistance live at home as opposed to nursing homes or group homes.
Services can include home visits from nurses or occupational therapists; assistance with personal care such as eating or bathing; help from case managers; attendance at adult day centers; help with cooking, cleaning and other chores; transportation; and home repairs and modifications. It can also help pay for durable medical equipment such as wheelchairs or oxygen tanks.
The need. At some point, 70% of older adults will require help with dressing, hygiene, moving around, managing finances, taking medications, cooking, housekeeping and other daily needs, usually for two to four years. As the nation’s aging population expands to 74 million in 2030 (the year all baby boomers will have entered older age), that need will expand exponentially.
Younger adults and children with conditions such as cerebral palsy, blindness or intellectual disabilities can similarly require significant assistance.
The burden on families. Currently, 53 million family members provide most of the care that vulnerable seniors and people with disabilities require — without being paid and often at significant financial and emotional cost. According to AARP, family caregivers on average devote about 24 hours a week, to helping loved ones and spend around $7,000 out-of-pocket.
This reflects a sobering reality: Long-term care services are simply too expensive for most individuals and families. According to a survey last year by Genworth, a financial services firm, the hourly cost for a home health aide averages $24. Annually, assisted living centers charge an average $51,600, while a semiprivate room in a nursing home goes for $93,075.
Medicare limitations. Many people assume that Medicare — the nation’s health program for 61 million older adults and people with severe disabilities — will pay for long-term care, including home-based services. But Medicare coverage is extremely limited.
In the community, Medicare covers home health only for older adults and people with severe disabilities who are homebound and need skilled services from nurses and therapists. It does not pay for 24-hour care or care for personal aides or homemakers. In 2018, about 3.4 million Medicare members received home health services.
In nursing homes, Medicare pays only for rehabilitation services for a maximum of 100 days. It does not provide support for long-term stays in nursing homes or assisted living facilities.
Medicaid options. Medicaid — the federal-state health program for 72 million children and adults in low-income households — can be an alternative, but financial eligibility standards are strict and only people with meager incomes and assets qualify.
Medicaid supports two types of long-term care: home and community-based services and those provided in institutions such as nursing homes. But only care in institutions is mandated by the federal government. Home and community-based services are provided at the discretion of the states.
Although all states offer home and community-based services of some kind, there’s enormous variation in the types of services offered, who is served (states can set caps on enrollment) and state spending. Generally, people need to be frail enough to need nursing home care to qualify.
Nationally, 57% of Medicaid’s long-term care budget goes to home and community-based services — $92 billion in the 2018 federal budget year. But half of states still spend twice as much on institutional care as they do on community-based care. And 41 states have waiting lists, totaling nearly 820,000 people, with an average wait of 39 months.
Based on the best information available, between 4 million and 5 million people receive Medicaid-funded home and community-based services — a fraction of those who need care.
Workforce issues. Biden’s proposal doesn’t specify how $400 billion in additional funding would be spent, beyond stating that access to home and community-based care would be expanded and caregivers would receive “a long-overdue raise, stronger benefits, and an opportunity to organize or join a union.”
Caregivers, including nursing assistants and home health and personal care aides, earn $12 an hour, on average. Most are women of color; about one-third of those working for agencies don’t receive health insurance from their employers.
By the end of this decade, an extra 1 million workers will be needed for home-based care — a number of experts believe will be difficult, if not impossible, to reach given poor pay and working conditions.
“We have a choice to keep these poverty-wage jobs or make them good jobs that allow people to take pride in their work while taking care of their families,” said Poo of Caring Across Generations.
Next steps.Biden’s plan leaves out many details. For example: What portion of funding should go to strengthening the workforce? What portion should be devoted to eliminating waiting lists? What amount should be spent on expanding services?
How will inequities of the current system — for instance, the lack of accessible services in rural counties or for people with dementia — be addressed? “We want to see funding to states tied to addressing those inequities,” said Amber Christ, directing attorney of the health team at Justice in Aging, an advocacy organization.
Meanwhile, supporters of the plan suggest it could be just the opening of a major effort to shore up other parts of the safety net. “There are huge gaps in the system for middle-income families that need to be addressed,” said David Certner, AARP’s legislative counsel.
Reforms that should be considered include tax credits for caregivers, expanding Medicare’s home health benefit and removing the requirement that people receiving Medicare home health be homebound, said Christ of Justice in Aging.
”We should be looking more broadly at potential solutions that reach people who have some resources but not enough to pay for these services as well,” she said.
Hospitals enrolled in the 340B drug discount program may no longer be eligible after the pandemic shifted their payer mix, according to a Wednesday letter the American Hospital Association sent to HHS Secretary Xavier Becerra.
Depleted patient volumes and canceled elective surgeries lowered the proportion of hospital patients who are Medicaid and Medicare SSI patients in 2020, according to AHA. When hospitals file their Medicare cost reports reflecting those changes, they may no longer meet the criteria for the program and lose access.
AHA wants HHS to waive certain eligibility requirements for hospitals in the program to allow them continued access during the public health emergency, according to the letter.
Dive Insight:
Throughout the pandemic HHS has issued a number of regulatory flexibilities to help providers, and the hospital lobby is asking it to do so again by waiving the current eligibility requirements for the 340B drug discount program before providers experiencing a temporary shift in payer mix are kicked out.
The program requires drug companies to give discounts on outpatient drugs to providers serving a large share of low-income patients, particularly those in rural areas.
The discounts can range from 25% to 50% of the cost of the drugs, according to HRSA, which operates the program.
But many of those patients did not seek care last year, hampering hospitals’ finances and altering the mix of payers.
Hospitals currently qualify for the program based on their volume of inpatient Medicaid and Medicare SSI patients, reported through their most recently filed Medicare cost reports.
“Losing access to 340B discounted drugs and program savings could jeopardize the ability of these hospitals to provide critical services for their communities, which would be particularly catastrophic at a time when they remain on the front lines of the ongoing pandemic,” AHA said in its letter.
This latest issue comes after several years of clashes over the 340B program.
Last year, a federal appeals court sided against the hospital lobby, ruling that HHS’ significant rate cut for some 340B drugs could remain in place. HHS made the reimbursement cut arguing that the hospitals already received steep discounts for the drugs and could be incentivized to overuse them.
At the time, AHA said it was weighing its options over whether to appeal to the Supreme Court.
To head off other issues, HRSA finalized a rule late last year that created a dispute resolution process for when hospitals believed they were overcharged for 340B drugs. The drug manufacturers have a similar mechanism to raise concerns about whether hospitals received duplicate discounts.
Doctors and health systems with a significant portion of risk-based contracts weathered the pandemic better than their peers still fully tethered to fee-for-service payment. Lower healthcare utilization translated into record profits, just as it did for insurers.
We’re now seeing an increasing number of health systems asking again whether they should enter the health plan business—levels of interest we haven’t seen since the “rush to risk” in the immediate aftermath of the passage of the Affordable Care Act a decade ago.
The discussions feel appreciably different this time around (which is a good thing, since many systems who launched plans in the prior wave had trouble growing and sustaining them). First, systems are approaching the market this time with a focus on Medicare Advantage, having seen that growing a base of covered lives with their networks is much easier than starting with the commercial market, where large insurers, particularly incumbent Blues plans, dominate the market, and many employers are still reticent to limit choice.
But foremost, there is new appreciation for the scale needed for a health plan to compete. In 2010, many executives set a goal of 100K covered lives as a target for sustainability; today, a plan with three times that number is considered small. Now many leaders posit that regional insurers need a plan to get to half a million lives, or more. (Somehow this doesn’t seem to hold for insurance startups: see the recent public offerings of Clover Health and Alignment Health, who have just 57K and 82K lives, respectively, nationwide.)
We’re watching for a coming wave of health system consolidation to gain the financial footing and geographic footprint needed to compete in the Medicare Advantage market, and would expect traditional payers to respond with regional consolidation of their own.
If you’re looking for an issue that can unite a heavily divided Congress, it seems nearly all Senators can get behind delaying payment cuts to providers during a pandemic. On Thursday the Senate voted 90-2 to pause the 2 percent sequester cuts to Medicare payment slated to go into effect on April 1.
The bill is expected to be passed by the House and signed into law by President Biden, delaying the cuts through the coronavirus public emergency. While hospitals, many of whom are still recovering from increased costs and volume loss during the pandemic, can breathe a sigh of relief,providers face an even larger 4 percent payment cut in the fall due to the PAYGO, or “pay as you go”, statute, which would trigger automatic payments cuts due to the deficit increases caused by the COVID relief bill.
We’d gamble that intense industry lobbying to delay the PAYGO cuts will prove successful—again, legislators will be reticent to dock provider payment as pandemic recovery continues. But eventually, in a more normal world, hospitals can expect policymakers to shift their focus from pandemic relief to cost control—and it will likely not prove possible to delay the inevitable reckoning over the high cost of our health system.
— At stake: scheduled payment reductions totalling $54 billion
Healthcare groups are applauding efforts being made in Congress to stop two different cuts to the Medicare budget — both of which are due to “sequestration” requirements — before it’s too late.
One cut, part of the normal budget process, is a 2% — or $18 billion — cut in the projected Medicare budget under a process known as “sequestration.” Sequestration allows for prespecified cuts in projected agency budget increases if Congress can’t agree on their own cuts. Medicare’s budget had been slated for a 2% sequester cut in fiscal year 2020; however, due to the pandemic and the accompanying increased healthcare needs, Congress passed a moratorium on the 2% cut. That moratorium is set to expire on April 1.
Another projected cut — this one for 4%, or $36 billion — will be triggered by the COVID relief bill, formally known as the American Rescue Plan Act. That legislation, which President Biden signed into law last Thursday, must conform to the PAYGO (pay-as-you-go) Act, which requires that any legislation that has a cost to it that is not otherwise offset must be offset by sequestration-style budget cuts to mandatory programs, including Medicare.
There are now several bills in Congress to address these pending cuts. H.R. 1868, co-sponsored by House Budget Committee chairman John Yarmuth (D-Ky.), House Ways & Means Committee chairman Richard Neal (D-Mass.), and House Energy & Commerce Committee chairman Frank Pallone Jr. (D-N.J.), among others, would get rid of the PAYGO Act requirement and extend the 2% Medicare sequester moratorium through the end of 2021.
Another bill, H.R. 315, introduced in January by Reps. Bradley Schneider (D-Ill.) and David McKinley (R-W.Va.), would extend the 2% sequester moratorium until the end of the public health emergency has been declared. In the Senate, S. 748, introduced Monday by senators Susan Collins (R-Maine) and Jeanne Shaheen (D-N.H.) would do the same.
“For many providers, the looming Medicare payment cuts would pose a further threat to their ability to stay afloat and serve communities during a time when they are most needed,” Shaheen said in a press release. “Congress should be doing everything in its power to prevent these cuts from taking effect during these challenging times, which is why I’m introducing this bipartisan legislation with Senator Collins. I urge the Senate to act at once to protect our health care providers and ensure they can continue their work on the frontlines of COVID-19.”
Not surprisingly, provider groups were happy about the actions in Congress. “MGMA [Medical Group Management Association] supports recent bipartisan, bicameral efforts to extend the 2% Medicare sequester moratorium for the duration of the COVID-19 public health emergency,” said Anders Gilberg, senior vice president for government affairs at MGMA, in a statement. “Without congressional action, the country’s medical groups will face a combined 6% sequester cut — a payment cut that is unsustainable given the financial hardships due to COVID-19 and keeping up with the cost of inflation.”
Leonard Marquez, senior director of government relations and legislative advocacy at the Association of American Medical Colleges, said in a statement that it was “critical” that Congress extend the 2% sequester moratorium “to help ensure hospitals, faculty physicians, and all providers have the necessary financial resources to continue providing quality care to COVID-19 and all patients ... While we are making progress against COVID-19, cutting provider payments in the middle of a pandemic could jeopardize the nation’s recovery.”
The American Medical Association (AMA) also urged Congress to prevent both the 2% and the 4% Medicare cuts. “We strongly oppose these arbitrary across-the-board Medicare cuts, and the predictably devastating impact they would have on many already distressed physician practices,” AMA executive vice president and CEO James Madara, MD, said in a letter sent to congressional leaders at the beginning of March.
“And, while Medicare spending on physician services partially recovered from the April low, it was still 12% less than expected by the end of June 2020,” he continued. “During the first half of 2020, the cumulative estimated reduction in Medicare physician spending associated with the pandemic was $9.4 billion (19%). Results from an earlier AMA-commissioned survey of 3,500 practicing physicians conducted from mid-July through August 2020 found that 81% of respondents were still experiencing lower revenue than before the pandemic.”
Not everyone is a fan of extending the 2% cut moratorium, however. “Bad idea,” said James Capretta, resident fellow at the American Enterprise Institute, a right-leaning think tank, at an event Tuesday on Medicare solvency sponsored by the Bipartisan Policy Center. “There’s plenty of give in the revenue streams of these systems that creating a precedent where we’re going to go back to the pre-sequester level — it’s better to move forward and if there are struggling systems out there, deal with it on an ad hoc basis rather than just across the board paying out a lot more money, which I don’t think is necessary.” He added, however, that he agreed with the bill to get rid of the 4% cut. “The bigger cut associated with PAYGO enforcement I think would be too much.”