A physician who has led the primary care enterprise for a large health system for over twenty years told us he’s never seen physician morale as low as it is now:
“Burnout is bad across the board for all specialties, but I’m having a really hard time finding the bright spots for primary care”.
We recalled a recent survey of primary care physicians that confirmed his observations, with 61 percent of doctors stating that primary care is “crumbling”. But it struck us that we’ve been seeing these kinds of dire surveys about the state of primary care for the entire quarter-century we’ve been doing this work.
What’s different now?
He posited one critical change. Ten years ago, during the heyday of accountable care, primary care was central to health system strategy. Systems were devoting resources to converting practices to patient-centered medical homes. “We felt like primary care was at the heart of transforming health systems, and that we were finally getting resources to help patients,” he shared.
“Now it feels like the health system has moved away from ‘value’, the focus is all on specialists and growing procedure volume again, and we’re being treated as a cost center and told to cut staff and up our referral targets.”
We agree. Although large independent primary care groups continue to command record valuations, overall, the transition to value has slowed, and work burden has increased given staffing shortages.
Where could optimism come from now?
We both agreed that workflow innovations to ease documentation burden and help the transition to virtual care appear closer to reality than ever before.
And the increased focus on “consumerism” has many systems recognizing that primary care is the first—and principal—touchpoint for most patients and will be key to winning consumer loyalty.
Running a health system recently has proven to be a very hard job. Mounting losses in the face of higher operating expenses, softer than expected volumes, deferred capex, and strained C-suite succession planning are just a few of the immediate issues with which CEOs and boards must deal.
But frankly, none of those are the biggest strategic issue facing health systems. The biggest strategic issue is the reorganization of the American healthcare landscape into an ambulatory care business that emphasizes competing for covered lives at scale in lower cost and convenient settings of care. This shift in business model has significant ramifications, if you own and operate acute care hospitals.
Village MD and Optum are two of the organizations driving the business model shift. They are owned by large publicly traded companies (Walgreens and UnitedHealth Group, respectively). Both Optum and Village MD have had a string of announced major patient care acquisitions over the past few years, none of which is in the acute care space.
The future of American healthcare will likely be dominated by large well-organized and well-run multi-specialty physician groups with a very strong primary care component. These physician service companies will be payer agnostic and focused on value-based care, though will still be prepared to operate in markets where fee-for-service dominates. They will deliver highly coordinated care in lower cost settings than hospital outpatient departments. And these companies will be armed with tools and analytics that permit them to manage the care for populations of patients, in order to deliver both better health outcomes and lower costs.
At the same time this is happening, we are experiencing steady growth in Medicare Advantage. And along with it, a stream of primary care groups who operate purpose-built clinics to take full risk on Medicare Advantage populations. These companies include ChenMed, Cano Health and Oak Street, among others. These organizations use strong culture, training, and analytics to better manage care, significantly reduce utilization, and produce better health outcomes and lower costs.
Public and private equity capital are pouring into the non-acute care sectors, fueling this growth. As of the start of 2022, nearly three quarters of all physicians in the US were employed by either corporate entities (such as private equity, insurance companies, and pharmacy companies), or employed by health systems. And this employment trend has accelerated since the start of the pandemic. The corporate entities, rather than health systems, are driving this increasing trend. Corporate purchases of physician practices increased by 86% from 2019 to 2021.
What can health systems do? To succeed in the future, you must be the nexus of care for the covered lives in your community. But that does not mean the health system must own all the healthcare assets or employ all of the physicians. The health system can be the platform to convene these assets and services in the community. In some respects, it is similar to an Apple iPhone. They are the platform that convenes the apps. Some of those apps are developed and owned by Apple. But many more apps are developed by people outside of Apple, and the iPhone is simply the platform to provide access.
Creating this platform requires a change in mindset. And it requires capital. There are many opportunities for health systems to partner with outside capital providers, such as private equity, to position for the future – from both a capital and a mindset point of view.
The change in mindset, and the access to flexible capital, is necessary as the future becomes more and more about reorganizing into an ambulatory care business that emphasizes competing for covered lives at scale in lower cost and convenient settings of care.
Late last week, Salt Lake City, Utah-based Intermountain Healthcare and University of Colorado-affiliated UCHealth, based in Aurora, CO, shared that they are jointly developing a clinically integrated network (CIN). It will initially comprise 700 primary care physicians working at UCHealth’s 12 hospitals and hundreds of clinics, but may expand in the future. The CIN will leverage Intermountain’s value-based care expertise and its SelectHealth insurance plans. The two health systems will remain independent and operate the CIN as a separate company.
The Gist: This partnership continues Intermountain’s expansion into Colorado, after it finalized its merger with SCL Health in April of last year.
It’s a smart way for Intermountain to strengthen its foothold in the state, especially as further health system acquisitions in the Denver area may raise antitrust concerns.
Intermountain will be able to tap into a larger network ofphysician relationships that it can use tobolster its health plan, with significantly lower infrastructure costs compared to employment.
These types of partnership strategies may also be bed-warming for deeper relationships, with the opportunity to demonstrate value before a full-on merger.
A certain segment of the health policy world spends a lot of time trying to get more states to expand Medicaid and reduce underinsurance.
But are we doing enough to make sure care is accessible once people enroll? One issue is access to physicians, who are less likely to treat patients on Medicaid than Medicare or private insurance because Medicaid payment rates are lower.
A new paper in Health Affairs by Avital Ludomirsky and colleagues looked at how well the networks of physicians supposedly participating in Medicaid reflect access to care. The researchers used claims data and provider directories from Medicaid managed care plans (the private insurers that most states contract with to run their Medicaid programs) in Kansas, Louisiana, Michigan and Tennessee from 2015 and 2017 to assess how the delivery of care to Medicaid patients was distributed among participating doctors. Their results were striking:
One-quarter of primary care physicians provided 86% of the care; one-quarter of specialists provided 75%.
One-third of both types of physicians saw fewer than 10 Medicaid patients per year, hardly contributing any “access” at all.
There was only one psychiatrist for every 8,834 Medicaid enrollees after excluding those seeing fewer than 10 Medicaid patients per year. This is especially concerning given that the COVID-19 pandemic has worsened mental health in the U.S., particularly among children.
The authors note that their study only covers primary care and mental health providers in four states, so it is not necessarily generalizable to other states or specialties. But these results are still concerning.
States have so-called network adequacy standards for their Medicaid managed care plans that are supposed to make sure there are enough providers. These standards typically rely on either a radius (a certain number of providers for a geographic area) or ratio (number of providers per enrollee), but the authors’ findings show these methods fall short if they are based on directories alone.
The authors specifically recommend states use claims-based assessments like the ones in the study and “secret shopper” programs — like this recently published one from Maryland by Abigail Burman and Simon Haeder — to better evaluate whether plans are offering adequate access to physicians. We absolutely need people to have coverage, but it needs to be more than just a card in their wallet.
We recently caught up with a health system chief clinical officer, who brought up some recent news about CVS. “I was really disappointed to hear that they’re going to start employing doctors,” he shared, referring to the company’s announcement earlier this month that it would begin to hire physicians to staff primary care practices in some stores. He said that as his system considered partnerships with payers and retailers, CVS stood out as less threatening compared to UnitedHealth Group and Humana, who both directly employ thousands of doctors: “Since they didn’t employ doctors, we saw CVS HealthHUBs as complementary access points, rather than directly competing for our patients.”
As CVS has integrated with Aetna, the company is aiming to expand its use of retail care sites to manage cost of care for beneficiaries. CEO Karen Lynch recently described plans to build a more expansive “super-clinic” platform targeted toward seniors, that will offer expanded diagnostics, chronic disease management, mental health and wellness, and a smaller retail footprint. The company hopes that these community-based care sites will boost Aetna’s Medicare Advantage (MA) enrollment, and it sees primary care physicians as central to that strategy.
It’s not surprising that CVS has decided to get into the physician business, as its primary retail pharmacy competitors have already moved in that direction. Last month, Walgreens announced a $5.2B investment to take a majority stake in VillageMD, with an eye to opening of 1,000 “Village Medical at Walgreens” primary care practices over the next five years. And while Walmart’s rollout of its Walmart Health clinics has been slower than initially announced, its expanded clinics, led by primary care doctors and featuring an expanded service profile including mental health, vision and dental care, have been well received by consumers. In many ways employing doctors makes more sense for CVS, given that the company has looked to expand into more complex care management, including home dialysis, drug infusion and post-operative care. And unlike Walmart or Walgreens, CVS already bears risk for nearly 3M Aetna MA members—and can immediately capture the cost savings from care management and directing patients to lower-cost servicesin its stores.
But does this latest move make CVS a greater competitive threat to health systems and physician groups? In the war for talent, yes. Retailer and insurer expansion into primary care will surely amp up competition for primary care physicians, as it already has for nurse practitioners. Having its own primary care doctors may make CVS more effective in managing care costs, but the company’s ultimate strategy remains unchanged: use its retail primary care sites to keep MA beneficiaries out of the hospital and other high-cost care settings.
Partnerships with CVS and other retailers and insurers present an opportunity for health systems to increase access points and expand their risk portfolios. But it’s likely that these types of partnerships are time-limited. In a consumer-driven healthcare market, answering the question of “Whose patient is it?” will be increasingly difficult, as both parties look to build long-term loyalty with consumers.
The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers (about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services. The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
Figure 1: MA HMO Out-of-Network Payments
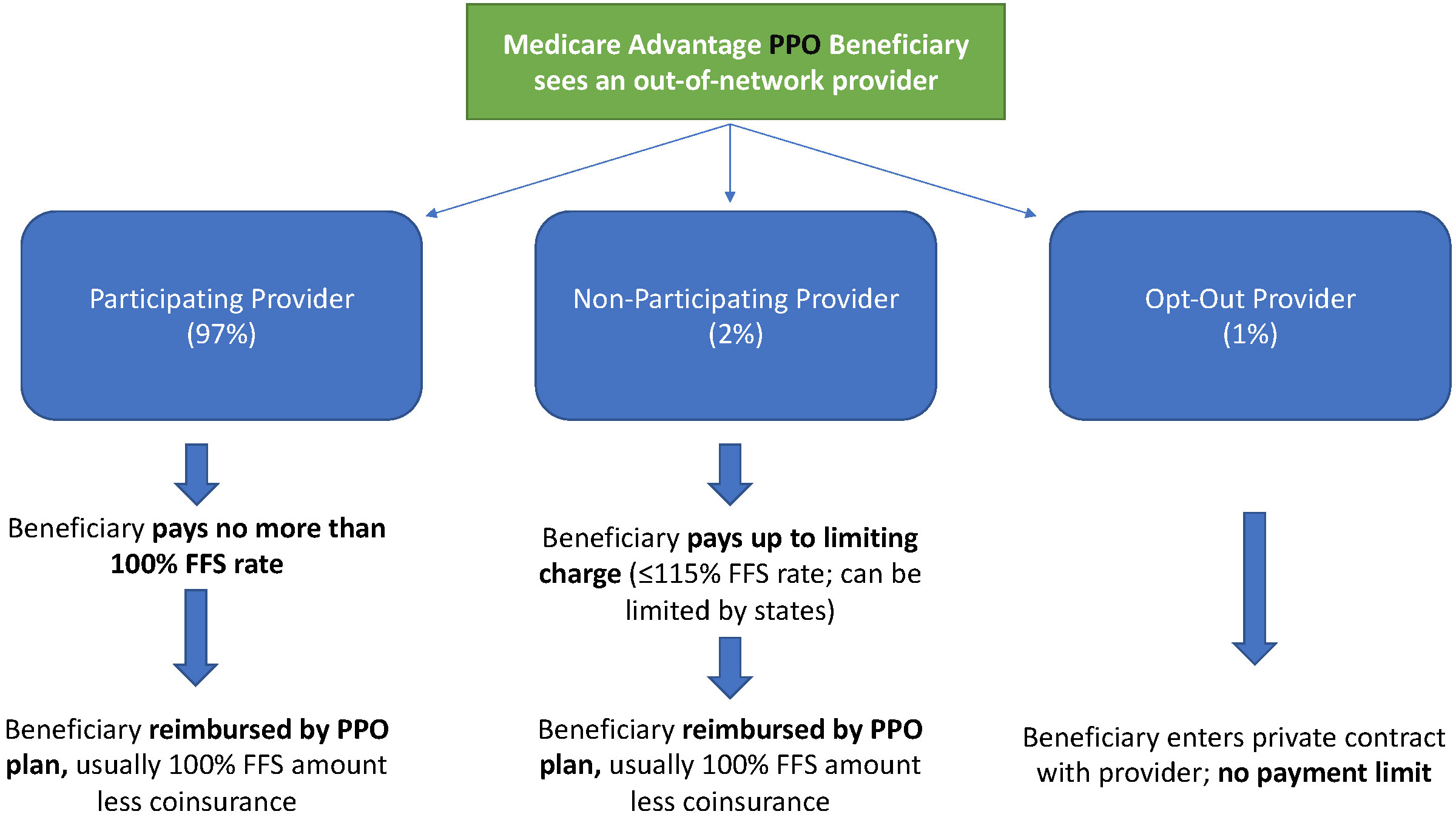
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (See Figure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.