More than two-thirds of U.S. physicians have changed their mind about generative AI and now view it as beneficial to healthcare. But as AI grows more powerful and prevalent in medicine, apprehensions remain high among medical professionals.
For the last 18 months, I’ve examined the potential uses and misuses of generative AI in medicine; research that culminated in the new book ChatGPT, MD: How AI-Empowered Patients & Doctors Can Take Back Control of American Medicine. Over that time, I’ve seen the concerns of clinicians evolve—from worries about AI’s reliability and, consequently, patient safety to a new set of fears: Who will be held liable when something goes wrong?
From safety to suits: A new AI fear emerges
Technology experts have grown increasingly certain that next-gen AI technologies will prove vastly safer and more reliable for patients, especially under expert human oversight. As evidence, recall that Google’s first medical AI model, Med-PaLM, achieved a mere “passing score” (>60%) on the U.S. medical licensing exam in late 2022. Five months later, its successor, Med-PaLM 2, scored at an “expert” doctor level (85%).
Since then, numerous studies have shown that generative AI increasingly outperforms medical professionals in various tasks. These include diagnosis, treatment decisions, data analysis and even expressing empathy.
Despite these technological advancements, errors in medicine can and will occur, regardless of whether the expertise comes from human clinicians or advanced AI.
Fault lines: Navigating AI’s legal terrain
Legal experts anticipate that as AI tools become more integrated into healthcare, determining liability will come down to whether errors result from AI decisions, human oversight or a combination of both.
For instance, if doctors use a generative AI tool in their offices for diagnosing or treating a patient and something goes wrong, the physician would likely be held liable, especially if it’s deemed that clinical judgement should have overridden the AI’s recommendations.
But the scenarios get more complex when generative AI is used without direct physician oversight. As an example, who is liable when patients rely on generative AI’s medical advice without ever consulting a doctor? Or what if a clinician encourages a patient to use an at-home AI tool for help interpreting wearable device data, and the AI’s advice leads to a serious health issue?
In a working paper, legal scholars from the universities of Michigan, Penn State and Harvard explored these challenges, noting: “Demonstrating the cause of an injury is already often hard in the medical context, where outcomes are frequently probabilistic rather than deterministic. Adding in AI models that are often nonintuitive and sometimes inscrutable will likely make causation even more challenging to demonstrate.”
That paper, published earlier this year in the New England Journal of Medicine, is based on hundreds of software-related tort cases and offers insights into the murky waters of AI liability, including how the courts might handle AI-related malpractice cases.
However, Mello pointed out that direct case law on any type of AI model remains “very sparse.” And when it comes to liability implications of using generative AI, specifically, there’s no public record of such cases being litigated.
“At the end of the day, it has almost always been the case that the physician is on the hook when things go wrong in patient care,” she noted but also added, “As long as physicians are using this to inform a decision with other information and not acting like a robot, deciding purely based on the output, I suspect they’ll have a fairly strong defense against most of the claims that might relate to their use of GPTs.”
She emphasized that while AI tools can improve patient care by enhancing diagnostics and treatment options, providers must be vigilant about the liability these tools could introduce. To minimize risk, she recommends four steps.
Understand the limits of AI tools: AI should not be seen as a replacement for human judgment. Instead, it should be used as a supportive tool to enhance clinical decisions.
Negotiate terms of use: Mello urges healthcare professionals to negotiate terms of service with AI developers like Nvidia, OpenAI, Google and others. This includes pushing back on today’s “incredibly broad” and “irresponsible” disclaimers that deny any liability for medical harm.
Apply risk assessment tools: Mello’s team developed a framework that helps providers assess the liability risks associated with AI. It considers factors like the likelihood of errors, the potential severity of harm caused and whether human oversight can effectively mitigate these risks.
Stay informed and prepared: “Over time, as AI use penetrates more deeply into clinical practice, customs will start to change,” Mello noted. Clinicians need to stay informed as the legal landscape shifts.
The high cost of hesitation: AI and patient safety
While concerns about the use of generative AI in healthcare are understandable, it’s critical to weigh these fears against the existing flaws in medical practice.
Each year, misdiagnoses lead to 371,000 American deaths while another 424,000 patients suffer permanent disabilities. Meanwhile, more than 250,000 deaths occur due to avoidable medical errors in the United States. Half a million people die annually from poorly managed chronic diseases, leading to preventable heart attacks, strokes, cancers, kidney failures and amputations.
Our nation’s healthcare professionals don’t have the time in their daily practice to address the totality of patient needs. That’s because the demand for medical services is higher than ever at a time when health insurers—with their restrictive policies and bureaucratic requirements—make it harder than ever to provide excellent care. Generative AI can help.
But it is imperative for policymakers, legal experts and healthcare professionals to collaborate on a framework that promotes the safe and effective use of this technology. As part of their work, they’ll need to address concerns over liability. Ultimately, they must recognize that the risks of not using generative AI to improve care will far outweigh the dangers posed by the technology itself. Only then can our nation reduce the enormous human toll resulting from our current medical failures.
Expenses per provider remained considerably higher than revenue generated in the first quarter of 2024, although there are signs the gap could be closing, according to the Kaufman Hall “Physician Flash Report,” released May 2.
Kaufman Hall based their findings on a monthly report from Syntellis Performance Solutions, part of Strata. The report gathered data from more than 200,000 employed providers, including physicians and advanced practice providers.
Net patient revenue per provider full-time equivalent was $383,881 for the first quarter, up 4% from the same period last year. Total direct expenses per provider FTE hit $620,729 for the quarter. Expense growth has slowed over the last three years, with a 5% growth from 2022 to 2023 and just 3% growth from 2023 to 2024.
“Labor expenses are a growing proportion of total expenses, a trend that is unlikely to change significantly. Organizations should shift from optimizing downstream revenue to optimizing downstream margins,” the report authors advised, noting hospitals and physician organizations can evaluate provider specialties by outcomes or other metrics when they aren’t big revenue drivers.
Provider productivity was up 4% as measured by work relative value units. Physician wRVU per FTE was 5,979 for the first quarter, up 6% year over year. Physician compensation jumped 3% to $364,319, down from 6% growth between 2022 to 2023.
Labor expenses continue to rise while support staff decline across specialties. Labor was 84% of total expenses in the first quarter, and support staff per 10k provider wRVUs dropped 6% year over year to 3.14, even after an 8% drop from 2022 to 2023. Report authors recommended organizations find better ways to use APPs for higher physician productivity.
Here are specific data points from the first quarter report.
Median net patient revenue per provider FTE by specialty cohort were:
Last Tuesday (April 23), the Federal Trade Commission (FTC) issued a 570-page final rule in a partisan 3-2 vote prohibiting employers from binding most American workers to post-employment non-competition agreements (the “Final Rule”):
“Pursuant to sections 5 and 6(g) of the Federal Trade Commission Act (“FTC Act”), the Federal Trade Commission (“Commission”) is issuing the Non-Compete Clause Rule (“the final rule”). The final rule provides that it is an unfair method of competition—and therefore a violation of section 5—for persons to, among other things, enter into non-compete clauses (“non-competes”) with workers on or after the final rule’s effective date. With respect to existing non-competes—i.e., non-competes entered into before the effective date—the final rule adopts a different approach for senior executives than for other workers. For senior executives (in policy setting/executive positions who earned more than $151,164 last year), existing non-competes can remain in force, while existing non-competes with other workers are not enforceable after the effective date.” (p.1)
“Concerns about non-competes have increased substantially in recent years in light of empirical research showing that they tend to harm competitive conditions in labor, product, and service markets. … When a company interferes with free competition for one of its former employee’s services, the market’s ability to achieve the most economically efficient allocation of labor is impaired. Moreover, employee-noncompetition clauses can tie up industry expertise and experience and thereby forestall new entry… competes by employers tends to negatively affect competition in labor markets, suppressing earnings for workers across the labor force—including even workers not subject to noncompete. This research has also shown that non-competes tend to negatively affect competition in product and service markets, suppressing new business formation and innovation… Yet despite the mounting empirical and qualitative evidence confirming these harms and the efforts of many States to ban them, non-competes remain prevalent in the U.S. economy. Based on the available evidence, the Commission estimates that approximately one in five American workers—or approximately 30 million workers—is subject to a non-compete. The evidence also indicates that employers frequently use non-competes even when they are unenforceable under State law.” (p.6)
On its home page, the FTC says “with a comprehensive ban on new non-competes, Americans could see an increase in wages, new business formation, reduced health care costs and more.”(www.ftc.gov)
The rule takes effect 120 days following its publication in the Federal Register and is applicable to every employer including specified operations in not-for-profit organizations (which represents the majority of hospitals, nursing homes and others). The agency noted it received 26,000 comment letters since the proposed rule was published January 19, 2023 including significant reaction from healthcare organizations. By the end of last week, two lawsuits were filed: one by the Chamber of Commerce in the United States District Court for the Eastern District of Texas and the second by a global tax services and software company in the Northern District of Texas – each challenging the Final Rule and arguing that the FTC lacked the authority. Others are likely to follow and its implementation will be delayed as arguments about its merits and the FTC’s standing to make the rule find their way thru the courts.
Special attention to hospitals and physicians in the rule
Notably, the use of non-competes in healthcare is a central theme in the rule, particularly in tax-exempt hospital and medical practice settings. Noting that one in 5 workers (30 million) and up to 45% of physicians work under non-compete agreements today, the Commissioners illustrated the need for the rule by inserting vignettes from 14 workers in their introduction: 4 of these were healthcare workers– 2 physicians and employees of a hospital and electronic health record provider (p.11-13). Throughout its exhaustive commentary, the Commissioners took issue with assertions by healthcare organizations about the potential negative consequences of the rule citing lack of empirical evidence to justify opposition claims. References to tax-exempt hospitals, their for-profit activities and their employment arrangements with physicians are frequent in the commentary justifying the application of the rule as follows:
“Many commenters representing healthcare organizations and industry trade associations stated that the Commission should exclude some or all of the healthcare industry from the rule because they believe it is uniquely situated in various ways. The Commission declines to adopt an exception specifically for the healthcare industry. The Commission is not persuaded that the healthcare industry is uniquely situated in a way that justifies an exemption from the final rule. The Commission finds use of non-competes to be an unfair method of competition that tends to negatively affect labor and product and services markets, including in this vital industry; the Commission also specifically finds that non-competes increase healthcare costs. Moreover, the Commission is unconvinced that prohibiting the use of non-competes in the healthcare industry will have the claimed negative effects.” (p.303)
Not surprisingly rule, responses from the hospital trade groups were swift, direct and harshly critical:
American Hospital Association (www.aha.org):” The FTC’s final rule banning non-compete agreements for all employees across all sectors of the economy is bad law, bad policy, and a clear sign of an agency run amok. The agency’s stubborn insistence on issuing this sweeping rule — despite mountains of contrary legal precedent and evidence about its adverse impacts on the health care markets — is further proof that the agency has little regard for its place in our constitutional order. Three unelected officials should not be permitted to regulate the entire United States economy and stretch their authority far beyond what Congress granted it–including by claiming the power to regulate certain tax-exempt, non-profit organizations. The only saving grace is that this rule will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities.”
Federation of American Hospitals (www.fah.org):“This final rule is a double whammy. In n a time of constant health care workforce shortages, the FTC’s vote today threatens access to high-quality care for millions of patients.”
By contrast, the American Medical Association (www.ama-assn.org) response was positive, linking its support for the rule to AMA’s ethical principles of physician independence and clinical autonomy.
Four implicit messages to healthcare are evident in the rule
It is unlikely the rule will become law in its current form. Opposing trade groups, employers dependent on non-competes for protections of trade secrets and business relationships and many others will actively pursue its demise in courts actions. But a review of the text makes clear the FTC is intensely focused on competition and consumer protections in healthcare akin to its ongoing challenges to hospital consolidation.
Four messages emerge from the text of the rule:
1-‘The healthcare industry is a business which needs more regulation to protect consumers and its workforce by lowering costs and stimulating competition. ‘
“Many commenters representing healthcare organizations and industry trade associations stated that the Commission should exclude some or all of the healthcare industry from the rule because they believe it is uniquely situated in various ways. The Commission declines to adopt an exception specifically for the healthcare industry. The Commission is not persuaded that the healthcare industry is uniquely situated in a way that justifies an exemption from the final rule. The Commission finds use of non-competes to be an unfair method of competition that tends to negatively affect labor and product and services markets, including in this vital industry; the Commission also specifically finds that non-competes increase healthcare costs. Moreover, the Commission is unconvinced that prohibiting the use of non-competes in the healthcare industry will have the claimed negative effects.” (p.373)
2-‘Physicians play a unique role in healthcare and deserve protection.’
“Some healthcare businesses and trade organizations opposing the rule argued that, without non-competes, physician shortages would increase physicians’ wages beyond what the commenters view as fair. The commenters provided no empirical evidence to support these assertions, and the Commission is unaware of any such evidence. Contrary to commenters’ claim that the rule would increase physicians’ earnings beyond a “fair” level, the weight of the evidence indicates that the final rule will lead to fairer wages by prohibiting a practice that suppresses workers’ earnings by preventing competition; that is, the final rule will simply help ensure that wages are determined via fair competition. The Commission also notes that it received a large number of comments from physicians and other healthcare workers stating that non-competes exacerbate physician shortages.” (p.157)
“Hundreds of physicians and other commenters in the healthcare industry stated that non-competes negatively affect physicians’ ability to provide quality care and limit patient access to care, including emergency care. Many of these commenters stated that non-competes restrict physicians from leaving practices and increase the risk of retaliation if physicians object to the practices’ operations, poor care or services, workload demands, or corporate interference with their clinical judgment. Other commenters from the healthcare industry said that, like other industries, non-competes bar competitors from the market and prevent providers from moving to or starting competing firms, thus limiting access to care and patient choice. Physicians and physician organizations said non-competes contribute to burnout and job dissatisfaction, and said burnout negatively impacts patient care.” (p.202)
“…the Commission notes that while the study finds that non-competes make physicians more likely to refer patients to other physicians within their practice—increasing revenue for the practice—it makes no findings on the impact on the quality of patient care. The Commission further notes that pecuniary benefits to a firm cannot justify an unfair method of competition.” (p.206)
3.’Tax exempt hospitals that operate like for-profit entities deserve special scrutiny from regulators and are thus subject to the rule’s provisions.’
“Merely claiming tax-exempt status in tax filings is not dispositive. At the same time, if the Internal Revenue Service (“IRS”) concludes that an entity does not qualify for tax-exempt status, such a finding would be meaningful to the Commission’s analysis of whether the same entity is a corporation under the FTC Act.” (p.53)
“As stated in Part II.E, entities claiming tax exempt status are not categorically beyond the Commission’s jurisdiction, but the Commission recognizes that not all entities in the healthcare industry fall under its jurisdiction. “(p.374)
“While the Commission shares commenters’ concerns about consolidation in healthcare, it disagrees with commenters’ contention that the purported competitive disadvantage to for-profit entities stemming from the final rule would exacerbate this problem. As some commenters stated, the Commission notes that hospitals claiming tax-exempt status as nonprofits are under increasing public scrutiny. Public and private studies and reports reveal that some such hospitals are operating to maximize profits, paying multi-million-dollar salaries to executives, deploying aggressive collection tactics with low-income patients, and spending less on community benefits than they receive in tax exemptions.943 Economic studies by FTC staff demonstrate that these hospitals can and do exercise market power and raise prices similar to for-profit hospitals.944 Thus, as courts have recognized, the tax-exempt status as nonprofits of merging hospitals does not mitigate the potential for harm to competitive conditions.” (p.383)
“Conversely, many commenters vociferously opposed exempting entities that claim tax exempt status as nonprofits from coverage under the final rule. Several commenters contended that, in practice, many entities that claim tax-exempt status as nonprofits are in fact “organized to carry on business for [their] own profit or that of [their] members” such that they are “corporations” under the FTC Act. These commenters cited reports by investigative journalists to contend that some hospitals claiming tax-exempt status as nonprofits have excess revenue and operate like for-profit entities. A few commenters stated that consolidation in the healthcare industry is largely driven by entities that claim tax-exempt status as nonprofits as opposed to their for-profit competitors, which are sometimes forced to consolidate to compete with the larger hospital groups that claim tax-exempt status as nonprofits. Commenters also contended that many hospitals claiming tax-exempt status as nonprofits use self-serving interpretations of the IRS’s “community benefit” standard to fulfill requirements for tax exemption, suggesting that the best way to address unfairness and consolidation in the healthcare industry is to strictly enforce the IRS’s standards and to remove the tax-exempt status of organizations that do not comply. An academic commenter argued that the distinction between for-profit hospitals and nonprofit hospitals has become less clear over time, and that the Commission should presumptively treat hospitals claiming nonprofit tax-exempt status as operating for profit unless they can establish that they fall outside of the Commission’s jurisdiction.” (p.377-378)
“After carefully considering commenters’ arguments, the Commission declines to exempt for-profit healthcare employers or to exempt the healthcare industry altogether.” (p.380)
4. ‘The net impact of non-compete agreements is harmful to the workforce and the public. ‘
“The Commission finds that with respect to these workers, these practices are unfair methods of competition in several independent ways:
The use of non-competes is restrictive and exclusionary conduct that tends to negatively affect competitive conditions in labor markets.
The use of non-competes is restrictive and exclusionary conduct that tends to negatively affect competitive conditions in product and service markets.
The use of non-competes is exploitative and coercive conduct that tends to negatively affect competitive conditions in labor markets.
The use of non-competes is exploitative and coercive conduct that tends to negatively affect competitive conditions in product and service markets.” (p.105)
“The Commission notes that the vast majority of comments from physicians and other stakeholders in the healthcare industry assert that non-competes result in worse patient care. The Commission further notes that the American Medical Association discourages the use of non-competes because they “can disrupt continuity of care, and may limit access to care.” In addition, there are alternatives for improving patient choice and quality of care, and for retaining physicians, that burden competition to a much less significant degree than non-competes…commenters asserted that a ban on non-competes would upend healthcare labor markets, thereby exacerbating healthcare workforce shortages, especially in rural and underserved areas. A medical society argued that non-competes can allow groups to meet contractual obligations to hospitals, as physicians leaving can prevent the group from ensuring safe care. As the Commission notes, there are not reliable empirical studies of these effects, and these commenters do not provide any. However, the Commission notes that the rule will increase labor mobility generally, which makes it easier for firms to hire qualified workers.” (p.208)
“The Commission also noted that in three States—California, North Dakota, and Oklahoma—employers generally cannot enforce non-competes, so they must protect their investments using one or more of these less restrictive alternatives…Commenters provide no empirical evidence, and the Commission is unaware of any such evidence, to support the theory that prohibiting non-competes would increase consolidation or raise prices. “384
The bottom line:
Odds are this rule will not become law anytime soon allowing healthcare organizations to consider alternatives to the non-competes they use. Work-arounds for protection of intellectual property, talent acquisition, employment agreements are likely as HR professionals, benefits and compensation consultancies huddle to consider what’s next.
Those that operate in 3 states (CA, ND, OK) already face state reg’s limiting non-competes and more states are adding measures. As noted in the rule, the health systems in these states have not been debilitated by non-compete limitations nor empirical evidence of public/worker harm produced, so no harm no foul.
The bigger takeaways from this rule for healthcare—especially hospitals—are 2:
The rule may fuel already growing antipathy between the workforce and senior management. Physicians are frustrated and burned out. Mid-level clinicians, techs and nurses are not happy. The hourly workforce is insecure. The hospital workplace—its clinics, programs and services—is not a happy place these days. The rule might fuel increased union organizing activity among some work groups at a critical time when demand is high, utilization is increasing, resources are stretched, reimbursement is shrinking and conditions for solvency and sustainability in question for rural, safety net and community hospitals in areas of declining population. And employed physicians will push-back harder against pressure from their hospital and private equity partners to work harder and produce more. The rule gives physicians a moral premise on which to oppose employer demands, whether the rule is implemented in its current form or not.
And the second equally notable takeaway is the rule’s specific attention to tax-exempt hospitals that operate as “for-profit” organizations. The FTC Commissioners question their tax exemptions and their investor-owned competitors are happy they noticed. They’re joined by investigations in 5 Committee’s of Congress with Bipartisan support for a fresh look at their bona fide eligibility despite strong pushback by the American Hospital Association and others.
This rule was introduced as a proposed rule last year with a comment period of 90 days allowed. Fifteen months and 26,000 comments later, it’s the latest reminder that the future of healthcare is everyone’s business and hospitals and physicians see that future state differently.
In its summation, the FTC estimates that this final rule will lead to new business formation growing by 2.7% per year, create 8,500 additional new businesses annually, produce 17,000-29,000 patents for innovation, increase earnings for workers and lower health care costs by up to $194 billion over the next decade. Maybe.
What’s clear is that the FTC and regulators in DC and many states are watching the industry closely and many aren’t buying what we’re selling.
In a world where change is the only constant, the swift currents of modern life contrast starkly with the sluggish pace of genetic evolution—and of American healthcare, too.
Two relatively recent scientific discoveries demonstrate how the very genetic traits that once secured humanity’s survival are failing to keep up with the times, producing dire medical consequences. These important biological events offer insights into American medicine—along with a warning about what can happen when healthcare systems fail to change.
The Mysteries Of Sickle Cell And Multiple Sclerosis
For decades, scientists were baffled by what seemed like an evolutionary contradiction.
Sickle cell disease is a condition resulting from a genetic mutation that produces malformed red blood cells. It afflicts approximately 1 in 365 Black Americans, causing severe pain and organ failure.
Its horrific impact on people raises a question: How has this genetic mutation persisted for 7,300 years? Nature is a merciless editor of life, and so you would expect that across seven millennia, people with this inherited problem would be less likely to survive and reproduce. This curiosity seems to defy the teachings of Charles Darwin, who theorized that evolution discards what no longer serves the survival of a species.
People living with sickle cell disease have two abnormal genes, one inherited from each parent. While the disease, itself, affects a large population (roughly 100,000 African Americans), it turns out that a far larger population in the United States carries one “abnormal” gene and one normal gene (comprising as many as 3 million Americans).
This so called “sickle cell trait” presents milder symptoms or none at all when compared to the full disease. And, unlike those with the disease, individuals who with one (but not both) abnormal genes possess a distinct evolutionary advantage: They have a resistance to severe malaria, which every year claims more than 600,000 lives around the globe.
This genetic adaptation (a resistance to malaria) kept people alive for many millennia in equatorial Africa, protecting them from the continent’s deadliest infectious disease. But in present-day America, malaria is not a major public-health concern due to several factors, including the widespread use of window screens and air conditioning, controlled and limited habitats for the Anopheles mosquitoes (which transmit the disease), and a strong healthcare system capable of managing and containing outbreaks. Therefore, the sickle cell trait is of little value in the United States while sickle cell disease is a life-threatening problem.
The lesson: Genetic changes beneficial in one environment, such as malaria-prone areas, can become harmful in another. This lesson isn’t limited to sickle cell disease.
A similar genetic phenomenon was uncovered through research that was published last month in Nature. This time, scientists discovered an ancient genetic mutation that is, today, linked to multiple sclerosis (MS).
Their research began with data showing that people living in Northern Europe have twice the number of cases of MS per 100,000 individuals as people in the South of Europe. Like sickle cell disease, MS is a terrible affliction—with immune cells attacking neurons in the brain, interfering with both walking and talking.
Having identified this two-fold variance in the prevalence of MS, scientists compared the genetic make-up of the people in Europe with MS versus those without this devastating problem. And they discovered a correlation between a specific mutated gene and the risk of developing MS. Using archeological material, the researchers then connected the introduction of this gene into Northern Europe with cattle, goat and sheep herders from Russia who migrated west as far back as 5,000 years ago.
Suddenly, the explanation comes into focus. Thousands of years ago, this genetic abnormality helped protect herders from livestock disease, which at the time was the greatest threat to their survival. However, in the modern era, this same mutation results in an overactive immune response, leading to the development of MS.
Once again, a trait that was positive in a specific environmental and historical context has become harmful in today’s world.
Evolving Healthcare: Lessons From Our Genes
Just as genetic traits can shift from beneficial to detrimental with changing circumstances, healthcare practices that were once lifesaving can become problematic as medical capabilities advance and societal needs evolve.
Fee-for-service (FFS) payments, the most prevalent reimbursement model in American healthcare, offer an example. Under FFS, insurance providers, the government or patients themselves pay doctors and hospitals for each individual service they provide, such as consultations, tests, and treatments—regardless of the value these services may or may not add.
In the 1930s, this “mutation” emerged as a solution to the Great Depression. Organizations like Blue Cross began providing health insurance, ensuring healthcare affordability for struggling Americans in need of hospitalization while guaranteeing appropriate compensation for medical providers.
FFS, which linked payments to the quantity of care delivered, proved beneficial when the problems physicians treated were acute, one-time issues (e.g., appendicitis, trauma, pneumonia) and relatively inexpensive to resolve.
Today, the widespread prevalence of chronic diseases in 6 out of 10 Americans underlines the limitations of the fee-for-service (FFS) model. In contrast to “pay for value” models, FFS, with its “pay for volume” approach, fails to prioritize preventive services, the avoidance of chronic disease complications, or the elimination of redundant treatments through coordinated, team-based care. This leads to increased healthcare costs without corresponding improvements in quality.
This situation is reminiscent of the evolutionary narrative surrounding genetic mutations like sickle cell disease and MS. These mutations, which provided protective benefits in the past, have become detrimental in the present. Similarly, healthcare systems must adapt to the evolving medical and societal landscape to better meet current needs.
Research demonstrates that it takes 17 years on average for a proven innovation in healthcare to become common practice. When it comes to evolution of healthcare delivery and financing, the pace of change is even more glacial.
In 1934, the Committee on the Cost of Medical Care (CCMC) concluded that better clinical outcomes would be achieved if doctors (a) worked in groups rather than as fragmented solo practices and (b) were paid based on the value they provided, rather than just the volume of work they did.
Nearly a century later, these improvements remain elusive. Well-led medical groups remain the minority of all practices while fee-for-service is still the dominant healthcare reimbursed method.
Things progress slowly in the biological sphere because chance is what initiates change. It takes a long time for evolution to catch up to new environments.
But change in healthcare doesn’t have to be random or painfully slow. Humans have a unique ability to anticipate challenges and proactively implement solutions. Healthcare, unlike biology, can advance rapidly in response to new medical knowledge and societal needs. We have the opportunity to leverage our knowledge, technology, and collaborative skills to address and adapt to change much faster than random genetic mutations. But it isn’t happening.
Standing in the way is a combination of fear (of the risks involved), culture (the norms doctors learn in training) and lack of leadership (the ability to translate vision into action).
Genetics teaches us that evolution ultimately triumphs. Mutations that save lives and improve health become dominant in nature over time. And when those adaptations no longer serve a useful purpose, they’re replaced.
I hope the leaders of American medicine will learn to adapt, embracing the power of collaborative medicine while replacing fee-for-service payments with capitation (a single annual payment to group of clinicians to provide the medical care for a population of patients.) If they wait too long, dinosaurs will provide them with the next set of biological lessons.
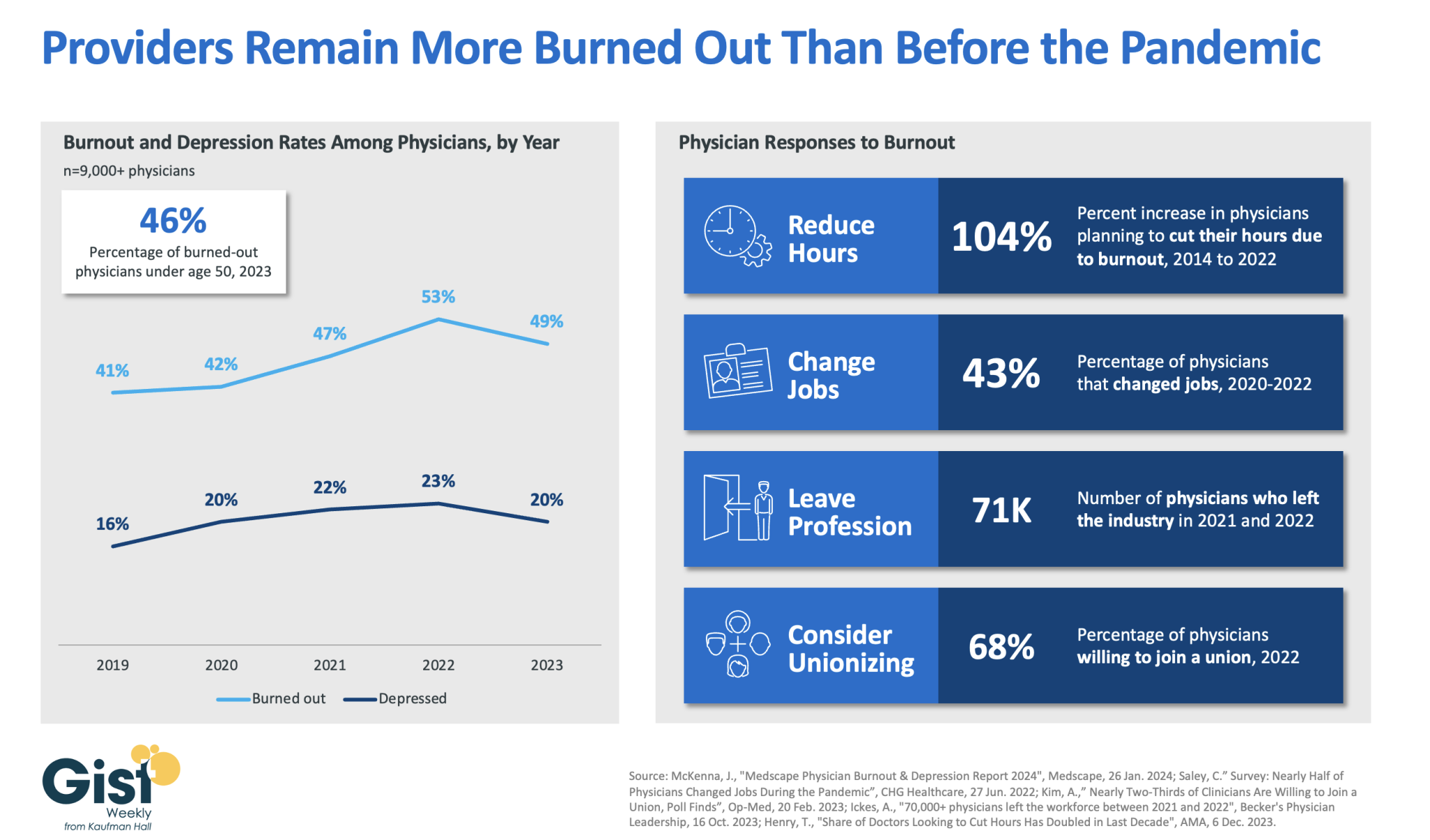
In 2023, nearly half of physicians reported feeling burned out, and a fifth reported feeling depressed. Although this does represent a drop from 2022’s peak, physicians remain more distressed than they were before the pandemic.
These numbers reveal some of the toll that the continued labor shortages, financial challenges, and payment changes of the past few years have taken on providers. In response to feeling burned out, an increased number of physicians say they are planning to cut their hours and over a third say they actually have changed jobs. Many have left the industry all together and the majority now say they are willing to join a union.
Health systems have long prioritized addressing provider burnout, but tighter operating margins have heightened both the challenge and the importance of helping to relieve it.
Continuing to find solutions to reduce administrative tasks, enhance team-based care models, and empower providers in decision-making processes are as important as ever for provider organizations today.
Day one of the healthcare strategy course I teach in the Stanford Graduate School of Business begins with this question: “Who here receives excellent medical care?”
Most of the students raise their hands confidently. I look around the room at some of the most brilliant young minds in business, finance and investing—all of them accustomed to making quick yet informed decisions. They can calculate billion-dollar deals to the second decimal point in their heads. They pride themselves on being data driven and discerning.
Then I ask, “How do you know you receive excellent care?”
The hands slowly come down and room falls silent. In that moment, it’s clear these future business leaders have reached a conclusion without a shred of reliable data or evidence.
Not one of them knows how often their doctors make diagnostic or technical errors. They can’t say whether their health system’s rate of infection or medical error is high, average or low.
What’s happening is that they’re conflating service with clinical quality. They assume a doctor’s bedside manner correlates with excellent outcomes.
These often false assumptions are part of a multi-millennia-long relationship wherein patients are reluctant to ask doctors uncomfortable but important questions: “How many times have you performed this procedure over the past year and how many patients experienced complications?” “What’s the worst outcome a patient of yours had during and after surgery?”
The answers are objective predictors of clinical excellence. Without them, patients are likely to become a victim of the halo effect—a cognitive bias where positive traits in one area (like friendliness) are assumed to carry over to another (medical expertise).
This is just one example of the many subconscious biases that distort our perceptions and decision-making.
From the waiting room to the operating table, these biases impact both patients and healthcare professionals with negative consequences. Acknowledging these biases isn’t just an academic exercise. It’s a crucial step toward improving healthcare outcomes.
Here are four more cognitive errors that cause harm in healthcare today, along with my thoughts on what can be done to mitigate their effects:
Availability bias
You’ve probably heard of the “hot hand” in Vegas—a lucky streak at the craps table that draws big cheers from onlookers. But luck is an illusion, a product of our natural tendency to see patterns where none exist. Nothing about the dice changes based on the last throw or the individual shaking them.
This mental error, first described as “availability bias” by psychologists Amos Tversky and Daniel Kahneman, was part of groundbreaking research in the 1970s and ‘80s in the field of behavioral economics and cognitive psychology. The duo challenged the prevailing assumption that humans make rational choices.
Availability bias, despite being identified nearly 50 years ago, still plagues human decision making today, even in what should be the most scientific of places: the doctor’s office.
Physicians frequently recommend a treatment plan based on the last patient they saw, rather than considering the overall probability that it will work. If a medication has a 10% complication rate, it means that 1 in 10 people will experience an adverse event. Yet, if a doctor’s most recent patient had a negative reaction, the physician is less likely to prescribe that medication to the next patient, even when it is the best option, statistically.
Confirmation bias
Have you ever had a “gut feeling” and stuck with it, even when confronted with evidence it was wrong? That’s confirmation bias. It skews our perceptions and interpretations, leading us to embrace information that aligns with our initial beliefs—and causing us to discount all indications to the contrary.
This tendency is heightened in a medical system where physicians face intense time pressures. Studies indicate that doctors, on average, interrupt patients within the first 11 seconds of being asked “What brings you here today?” With scant information to go on, doctors quickly form a hypothesis, using additional questions, diagnostic testing and medical-record information to support their first impression.
Doctors are well trained, and their assumptions prove more accurate than incorrect overall. Nevertheless, hasty decisions can be dangerous. Each year in the United States, an estimated 371,000 patients die from misdiagnoses.
Patients aren’t immune to confirmation bias, either. People with a serious medical problem commonly seek a benign explanation and find evidence to justify it. When this happens, heart attacks are dismissed as indigestion, leading to delays in diagnosis and treatment.
Framing effect
In 1981, Tversky and Kahneman asked subjects to help the nation prepare for a hypothetical viral outbreak. They explained that if the disease was left untreated, it would kill 600 people. Participants in one group were told that an available treatment, although risky, would save 200 lives. The other group was told that, despite the treatment, 400 people would die. Although both descriptions lead to the same outcome—200 people surviving and 400 dying—the first group favored the treatment, whereas the second group largely opposed it.
The study illustrates how differently people can react to identical scenarios based on how the information is framed. Researchers have discovered that the human mind magnifies and experiences loss far more powerfully than positive gains. So, patients will consent to a chemotherapy regiment that has a 20% chance of cure but decline the same treatment when told it has 80% likelihood of failure.
Self-serving bias
The best parts about being a doctor are saving and improving lives. But there are other perks, as well.
Pharmaceutical and medical-device companies aggressively reward physicians who prescribe and recommend their products. Whether it’s a sponsored dinner at a Michelin restaurant or even a pizza delivered to the office staff, the intention of the reward is always the same: to sway the decisions of doctors.
And yet, physicians swear that no meal or gift will influence their prescribing habits. And they believe it because of “self-serving bias.”
In the end, it’s patients who pay the price. Rather than receiving a generic prescription for a fraction of the cost, patients end up paying more for a brand-name drug because their doctor—at a subconscious level—doesn’t want to lose out on the perks.
Thanks to the “Sunshine Act,” patients can check sites like ProPublica’s Dollars for Docs to find out whether their healthcare professional is receiving drug- or device-company money (and how much).
Reducing subconscious bias
These cognitive biases may not be the reason U.S. life expectancy has stagnated for the past 20 years, but they stand in the way of positive change. And they contribute to the medical errors that harm patients.
A study published this month in JAMA Internal Medicine found that 1 in 4 hospital patients who either died or were transferred to the ICU had been affected by a diagnostic mistake. Knowing this, you might think cognitive biases would be a leading subject at annual medical conferences and a topic of grave concern among healthcare professionals. You’d be wrong. Inside the culture of medicine, these failures are commonly ignored.
The recent story of an economics professor offers one possible solution. Upon experiencing abdominal pain, he went to a highly respected university hospital. After laboratory testing and observation, his attending doctor concluded the problem wasn’t serious—a gallstone at worst. He told the patient to go home and return for outpatient workup.
The professor wasn’t convinced. Fearing that the medical problem was severe, the professor logged onto ChatGPT (a generative AI technology) and entered his symptoms. The application concluded that there was a 40% chance of a ruptured appendix. The doctor reluctantly ordered an MRI, which confirmed ChatGPT’s diagnosis.
Future generations of generative AI, pretrained with data from people’s electronic health records and fed with information about cognitive biases, will be able to spot these types of errors when they occur.
Deviation from standard practice will result in alerts, bringing cognitive errors to consciousness, thus reducing the likelihood of misdiagnosis and medical error. Rather than resisting this kind of objective second opinion, I hope clinicians will embrace it. The opportunity to prevent harm would constitute a major advance in medical care.
Around 400 primary and urgent care physicians, along with 150 nurse practitioners and physician assistants, employed by Minneapolis, MN-based Allina Health System have voted to unionize with the Service Employees International Union, forming the largest private-sector union of physicians in the country.
Allina, which operates 12 hospitals across Minnesota and Wisconsin, already saw over 100 inpatient physicians at its Mercy Hospital vote to unionize earlier this year. While Mercy’s physicians organized against pressure to adhere to the hospital’s new length-of-stay guidelines, this larger group of clinic-based providers say they are motivated by chronic understaffing that they claim has caused burnout and threatened patient safety. Allina Health laid off 350 workers this summer after posting a nearly $200M operating loss in 2022.
The Gist:When health systems originally recruited physicians into their newly developed employed medical groups, many pitched the arrangement as more of a partnership than traditional employment.
However, now that a majority of the nation’s physicians are employed by hospitals, some physicians are rethinking their relationships with their employers.
Only six percent of doctors were unionized in 2021, but a recent spate of unionization efforts by residents and physicians suggest that number is on the rise.
Health systems hoping to address physicians’ concerns and unionization activity should note that the motivating factors cited by organizing physicians surround working conditions, including a lack of support staff and professional autonomy, rather than personal wage demands.
Hospitals and health systems are seeing some signs of stabilization in 2023 following an extremely difficult year in 2022. Workforce-related challenges persist, however, keeping costs high and contributing to issues with patient access to care. The percentage of respondents who report that they have run at less than full capacity at some time over the past year because of staffing shortages, for example, remains at 66%, unchanged from last year’s State of Healthcare Performance Improvement report. A solid majority of respondents (63%) are struggling to meet demand within their physician enterprise, with patient concerns or complaints about access to physician clinics increasing at approximately one-third (32%) of respondent organizations.
Most organizations are pursuing multiple strategies to recruit and retain staff. They recognize, however, that this is an issue that will take years to resolve—especially with respect to nursing staff—as an older generation of talent moves toward retirement and current educational pipelines fail to generate an adequate flow of new talent. One bright spot is utilization of contract labor, which is decreasing at almost two-thirds (60%) of respondent organizations.
Many of the organizations we interviewed have recovered from a year of negative or breakeven operating margins. But most foresee a slow climb back to the 3% to 4% operating margins that help ensure long-term sustainability, with adequate resources to make needed investments for the future. Difficulties with financial performance are reflected in the relatively high percentage of respondents (24%) who report that their organization has faced challenges with respect to debt covenants over the past year, and the even higher percentage (34%) who foresee challenges over the coming year. Interviews confirmed that some of these challenges were “near misses,” not an actual breach of covenants, but hitting key metrics such as days cash on hand and debt service coverage ratios remains a concern.
As in last year’s survey, an increased rate of claims denials has had the most significant impact on revenue cycle over the past year. Interviewees confirm that this is an issue across health plans, but it seems particularly acute in markets with a higher penetration of Medicare Advantage plans. A significant percentage of respondents also report a lower percentage of commercially insured patients (52%), an increase in bad debt and uncompensated care (50%), and a higher percentage of Medicaid patients (47%).
Supply chain issues are concentrated largely in distribution delays and raw product and sourcing availability. These issues are sometimes connected when difficulties sourcing raw materials result in distribution delays. The most common measures organizations are taking to mitigate these issues are defining approved vendor product substitutes (82%) and increasing inventory levels (57%). Also, as care delivery continues to migrate to outpatient settings, organizations are working to standardize supplies across their non-acute settings and align acute and non-acute ordering to the extent possible to secure volume discounts.
Survey Highlights
98% of respondents are pursuing one or more recruitment and retention strategies
90%have raised starting salaries or the minimum wage
73%report an increased rate of claims denials
71% are encountering distribution delays in their supply chain
70%are boarding patients in the emergency department or post-anesthesia care unit because of a lack of staffing or bed capacity
66% report that staffing shortages have required their organization to run at less than full capacity at some time over the past year
63% are struggling to meet demand for patient access to their physician enterprise
60% see decreasing utilization of contract labor at their organization
44%report that inpatient volumes remain below pre-pandemic levels
32% say that patients concerns or complaints about access to their physician enterprise are increasing
24%have encountered debt covenant challenges during the past 12 months
None of our respondents believe that their organization has fully optimized its use of the automation technologies in which it has already invested
Artificial intelligence (AI) has long been heralded as an emerging force in medicine. Since the early 2000s, promises of a technological transformation in healthcare have echoed through the halls of hospitals and at medical meetings.
But despite 20-plus years of hype, AI’s impact on medical practice and America’s health remains negligible (with minor exceptions in areas like radiological imaging and predictive analytics).
As such, it’s understandable that physicians and healthcare administrators are skeptical about the benefits that generative AI tools like ChatGPT will provide.
They shouldn’t be. This next generation of AI is unlike any technology that has come before.
The launch of ChatGPT in late 2022 marked the dawn of a new era. This “large language model” developed by OpenAI first gained notoriety by helping users write better emails and term papers. Within months, a host of generative AI products sprang up from Google, Microsoft and Amazon and others. These tools are quickly becoming more than mere writing assistants.
In time, they will radically change healthcare, empower patients and redefine the doctor-patient relationship. To make sense of this bold vision for the future, this two-part article explores:
The massive differences between generative AI and prior artificial intelligences
How, for the first time in history, a technological innovation will democratize not just knowledge, but also clinical expertise, making medical prowess no longer the sole domain of healthcare professionals.
To understand why this time is different, it’s helpful to compare the limited power of the two earliest generations of AI against the near-limitless potential of the latest version.
Generation 1: Rules-Based Systems And The Dawn Of AI In Healthcare
The latter half of the 20th century ushered in the first generation of artificial intelligence, known as rule-based AI.
Programmed by computer engineers, this type of AI relies on a series of human-generated instructions (rules), enabling the technology to solve basic problems.
In many ways, the rule-based approach resembles a traditional medical-school pedagogy where medical students are taught hundreds of “algorithms” that help them translate a patient’s symptoms into a diagnosis.
These decision-making algorithms resemble a tree, beginning with a trunk (the patient’s chief complaint) and branching out from there. For example, if a patient complains of a severe cough, the doctor first assesses whether fever is present. If yes, the doctor moves to one set of questions and, if not, to a different set. Assuming the patient has been febrile (with fever), the next question is whether the patient’s sputum is normal or discolored. And once again, this leads to the next subdivision. Ultimately each end branch contains only a single diagnosis, which can range from bacterial, fungal or viral pneumonia to cancer, heart failure or a dozen other pulmonary diseases.
This first generation of AI could rapidly process data, sorting quickly through the entire branching tree. And in circumstances where the algorithm could accurately account for all possible outcomes, rule-based AI proved more efficient than doctors.
But patient problems are rarely so easy to analyze and categorize. Often, it’s difficult to separate one set of diseases from another at each branch point. As a result, this earliest form of AI wasn’t as accurate as doctors who combined medical science with their own intuition and experience. And because of its limitations, rule-based AI was rarely used in clinical practice.
Generation 2: Narrow AI And The Rise Of Specialized Systems
As the 21st century dawned, the second era of AI began. The introduction of neural networks, mimicking the human brain’s structure, paved the way for deep learning.
Narrow AI functioned very differently than its predecessors. Rather than researchers providing pre-defined rules, the second-gen system feasted on massive data sets, using them to discern patterns that the human mind, alone, could not.
In one example, researchers gave a narrow AI system thousands of mammograms, half showing malignant cancer and half benign. The model was able to quickly identify dozens of differences in the shape, density and shade of the radiological images, assigning impact factors to each that reflected the probability of malignancy. Importantly, this kind of AI wasn’t relying on heuristics (a few rules of thumb) the way humans do, but instead subtle variations between the malignant and normal exams that neither the radiologists nor software designers knew existed.
In contrast to rule-based AI, these narrow AI tools proved superior to the doctor’s intuition in terms of diagnostic accuracy. Still, narrow AI showed serious limitations. For one, each application is task specific. Meaning, a system trained to read mammograms can’t interpret brain scans or chest X-rays.
But the biggest limitation of narrow AI is that the system is only as good as the data it’s trained on. A glaring example of that weakness emerged when United Healthcare relied on narrow AI to identify its sickest patients and give them additional healthcare services.
In filtering through the data, researchers later discovered the AI had made a fatal assumption. Patients who received less medical care were categorized as healthier than patients who received more. In doing so, the AI failed to recognize that less treatment is not always the result of better health. This can also be the result of implicit human bias.
Indeed, when researchers went back and reviewed the outcomes, they found Black patients were being significantly undertreated and were, therefore, underrepresented in the group selected for additional medical services.
Media headlines proclaimed, “Healthcare algorithm has racial bias,” but it wasn’t the algorithm that had discriminated against Black patients. It was the result of physicians providing Black patients with insufficient and inequitable treatment. In other words, the problem was the humans, not narrow AI.
Generation 3: The Future Is Generative
Throughout history, humankind has produced a few innovations (printing press, internet, iPhone) that transformed society by democratizing knowledge—making information easier to access for everyone, not just the wealthy elite.
Now, generative AI is poised to go one step further, giving every individual access to not only knowledge but, more importantly, expertise as well.
Already, the latest AI tools allow users to create a stunning work of art in the style of Rembrandt without ever having taken a painting class. With large language models, people can record a hit song, even if they’ve never played a musical instrument. Individuals can write computer code, producing sophisticated websites and apps, despite never having enrolled in an IT course.
Future generations of generative AI will do the same in medicine, allowing people who never attended medical school to diagnose diseases and create a treatment plan as well as any clinician.
Already, one generative AI tool (Google’s Med-PaLM 2) passed the physician licensing exam with an expert level score. Another generative AI toolset responded to patient questions with advice that bested doctors in both accuracy and empathy. These tools can now write medical notes that are indistinguishable from the entries that physicians create and match residents’ ability to make complex diagnoses on difficult cases.
Granted, current versions require physician oversight and are nowhere close to replacing doctors. But at their present rate of exponential growth, these applications are expected to become at least 30 times more powerful in the next five years. As a result, they will soon empower patients in ways that were unimaginable even a year ago.
Unlike their predecessors, these models are pre-trained on datasets that encompass the near-totality of publicly available information—pulling from medical textbooks, journal articles, open-source platforms and the internet. In the not-distant future, these tools will be securely connected to electronic health records in hospitals, as well as to patient monitoring devices in the home. As generative AI feeds on this wealth of data, its clinical acumen will skyrocket.
Within the next five to 10 years, medical expertise will no longer be the sole domain of trained clinicians. Future generations of ChatGPT and its peers will put medical expertise in the hands of all Americans, radically altering the relationship between doctors and patients.
Whether physicians embrace this development or resist is uncertain. What is clear is the opportunity for improvement in American medicine. Today, an estimated 400,000 people die annually from misdiagnoses, 250,000 from medical errors, and 1.7 million from mostly preventable chronic diseases and their complications.
In the next article, I’ll offer a blueprint for Americans as they grapple to redefine the doctor-patient relationship in the context of generative AI. To reverse the healthcare failures of today, the future of medicine will have to belong to the empowered patient and the tech-savvy physician. The combination will prove vastly superior to either alone.